Acking pain on heel for women 45 years old differential diagnosis
Reading File
Finding Sources
Finding Sources
Searching PubMed
"heel pain" differential diagnosis
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have all the information needed for a thorough answer. Here is the complete differential diagnosis for aching heel pain in a 45-year-old woman:
Differential Diagnosis: Heel Pain in a 45-Year-Old Woman
Heel pain is extremely common - roughly 10% of people experience at least one episode in their lifetime. In a middle-aged woman, the differential spans several anatomical zones of the heel (plantar, posterior, medial), and the age/sex profile raises particular considerations around perimenopause-related bone changes, inflammatory arthritis, and foot mechanics.
Anatomy-Based Framework
Pain is best organized by location on the heel:
| Location | Primary Diagnoses |
|---|---|
| Plantar (undersurface) | Plantar fasciitis, heel pad atrophy, plantar fascia tear, lateral plantar nerve entrapment, calcaneal stress fracture, bursitis |
| Posterior | Achilles insertional tendinopathy, retrocalcaneal bursitis, Haglund deformity, Achilles bursitis |
| Medial/diffuse | Tarsal tunnel syndrome, inflammatory arthropathy, posterior tibial tendon dysfunction |
1. Plantar Fasciitis (Plantar Fasciopathy) - MOST COMMON
The most common cause of heel pain overall, accounting for the vast majority of cases.
- Pain location: Inferomedial heel (plantar surface, at calcaneal enthesis)
- Classic feature: Worst on first steps in the morning ("first-step pain") and after periods of rest; improves with activity then worsens again
- Mechanism: Degenerative changes at the calcaneal enthesis due to repetitive traction via the windlass mechanism; aging reduces collagen and water content in the plantar fascia
- Risk factors relevant to this patient: Obesity, pes planus (flat foot), pes cavus, tight heel cord (Achilles), decreased knee extension
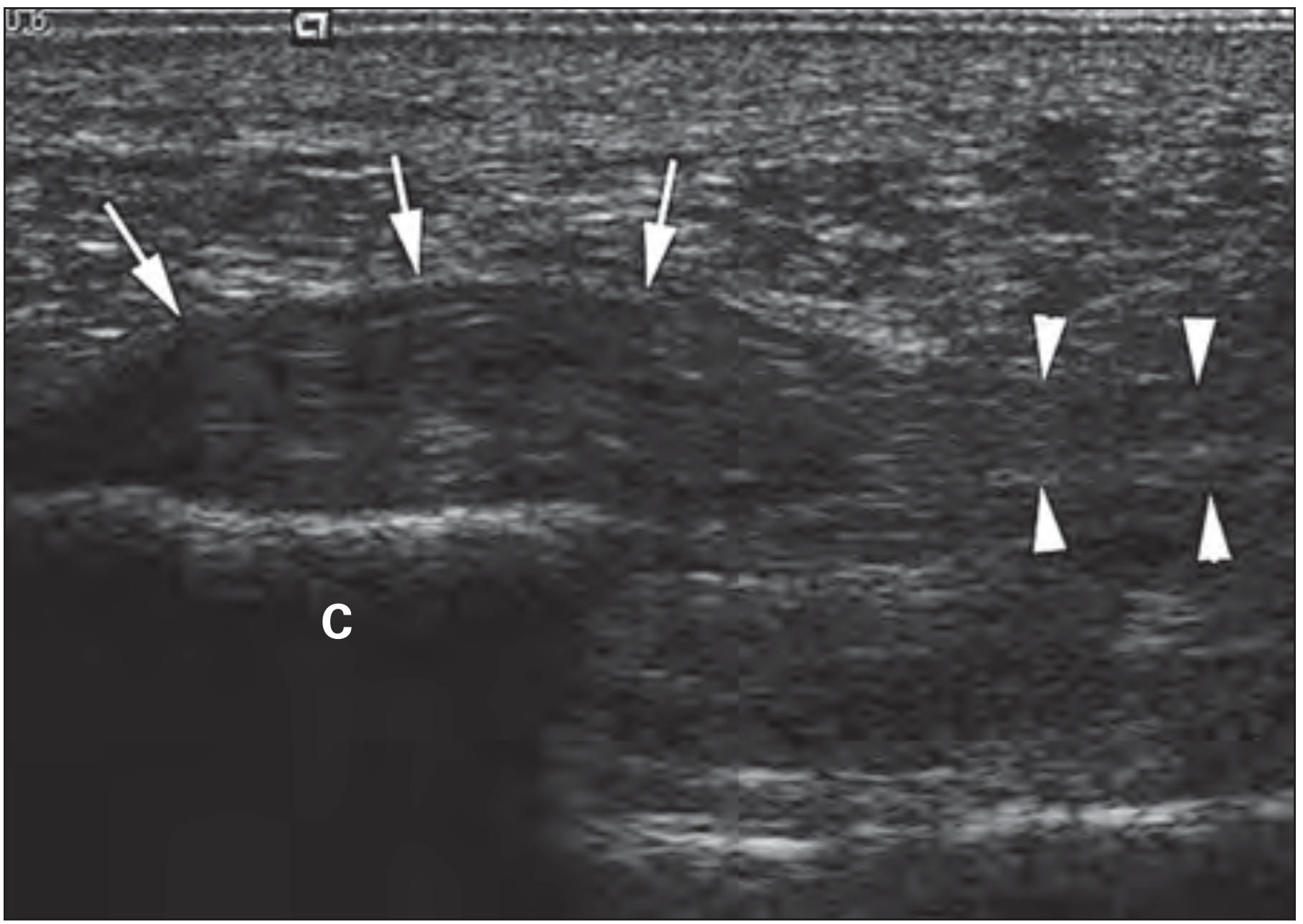
- Diagnosis: Clinical; ultrasound confirms fascial thickening at the enthesis (see image below)
- Course: Majority resolve within 18 months; self-limiting in many cases
2. Heel Pad Atrophy
- The heel fat pad normally cushions impact; with aging, collagen and water content decline, reducing its shock-absorbing capacity
- Particularly relevant at 45 years old, as perimenopause accelerates connective tissue changes
- Pain: Diffuse plantar heel, worsens with walking on hard surfaces
- Exam: Heel pad feels thin and less spongy; may look flattened
- Distinguishing from plantar fasciitis: No localized tenderness at the medial calcaneal tubercle; pain is more diffuse and not specifically worse in the morning
3. Calcaneal Stress Fracture
- Relevant in perimenopausal women due to declining estrogen - increases bone turnover risk
- Pain: Diffuse heel pain, worsens with weight-bearing activity; may be subacute/progressive
- Classic exam sign: Positive "squeeze test" - pain elicited by mediolateral compression of the calcaneus
- Imaging: X-ray often negative early; MRI or CT-SPECT are most sensitive
- Important to rule out when there is bone-quality concern (low bone density, prolonged steroid use, early menopause)
4. Entrapment of the First Branch of the Lateral Plantar Nerve (Baxter's Nerve Entrapment)
- Often underdiagnosed, sometimes called "Baxter's nerve" entrapment
- The nerve is compressed between the abductor hallucis muscle and the medial plantar fascia
- Pain: Plantar heel, similar distribution to plantar fasciitis; may radiate along the medial arch
- Key distinguishing feature: Burning or tingling quality, tender along the medial heel; may persist after plantar fasciitis treatment
- A 2025 review in Neurol Sci (PMID 40418415) highlights this as a "hidden culprit" in chronic heel pain that is frequently missed
5. Tarsal Tunnel Syndrome
- Compression of the posterior tibial nerve (or its branches) in the tarsal tunnel behind and below the medial malleolus
- Pain/symptoms: Burning, tingling, or aching on the plantar surface and medial heel; may radiate into the toes
- Exam: Positive Tinel's sign at the tarsal tunnel; electromyography/nerve conduction studies confirm
- More common in women, flat-footed individuals, and those with systemic conditions (rheumatoid arthritis, hypothyroidism)
6. Achilles Insertional Tendinopathy
- Posterior heel pain at the Achilles insertion onto the calcaneus
- Pain: Posterior heel, worse with activity (running, climbing stairs), tender at the tendon insertion
- Distinct from non-insertional tendinopathy (which is 2-6 cm above the insertion)
- More common in middle-aged individuals, often associated with tight gastrocnemius-soleus complex
7. Retrocalcaneal Bursitis / Achilles Bursitis
- Retrocalcaneal bursa: Deep to the Achilles tendon - more often associated with inflammatory disease (RA, seronegative arthropathies)
- Achilles (adventitious) bursa: Superficial to the tendon insertion - prone to mechanical irritation from footwear
- Pain: Posterior heel, pain/swelling at the back of the heel
- Diagnosis confirmed by MRI or ultrasound
8. Haglund Deformity ("Pump Bump")
- Bony prominence on the posterior-superior calcaneus, often aggravated by rigid footwear (e.g., high heels - relevant in women)
- Causes mechanical irritation of the retrocalcaneal bursa and Achilles tendon
- Exam: Prominent bony bump; pain reproduced by shoe pressure
- X-ray confirms the calcaneal deformity
9. Inflammatory Enthesitis / Seronegative Arthropathy
- Bilateral heel pain in particular should prompt consideration of seronegative spondyloarthropathies: psoriatic arthritis, ankylosing spondylitis, reactive arthritis (Reiter syndrome)
- Enthesitis at the calcaneal insertion of the plantar fascia or Achilles tendon is a hallmark
- Clues: Morning stiffness >45 minutes, associated back pain, skin lesions (psoriasis), bowel symptoms, uveitis, elevated ESR/CRP, HLA-B27 positivity
- Rheumatoid arthritis can also cause heel pain (usually via retrocalcaneal bursitis)
10. Plantar Fascia Rupture / Tear
- Acute partial or complete tear, often during push-off phase of gait or after corticosteroid injection
- Pain: Sudden-onset plantar heel pain; passive dorsiflexion of hallux is painful
- Swelling may be visible
- MRI confirms the tear
11. Posterior Tibial Tendon Dysfunction (PTTD)
- The posterior tibial tendon supports the medial arch; degeneration leads to progressive flatfoot
- Pain: Medial ankle and heel, worsens with activity
- Exam: Inability to perform single heel-rise; progressive pes planus deformity
- More common in women aged 40-60
12. Less Common / Red Flag Diagnoses to Exclude
| Condition | Clue |
|---|---|
| Calcaneal bone tumor (osteoid osteoma, intraosseous lipoma) | Night pain, pain not related to activity, X-ray/MRI findings |
| Deep soft-tissue abscess | Fever, diabetes, immunosuppression |
| Ledderhose's disease (plantar fibromatosis) | Palpable nodules in the plantar fascia |
| Gout/pseudogout | Acute inflammatory episodes, elevated uric acid |
| Referred pain (S1 radiculopathy) | Back pain, neurological deficits, positive straight-leg raise |
Age- and Sex-Specific Considerations at 45 Years Old
- Perimenopause effect on bone: Declining estrogen increases calcaneal stress fracture risk - always consider in unexplained worsening heel pain
- Footwear: Women's shoe choices (high heels, narrow toe-box) increase Haglund deformity, Achilles stress, and forefoot-to-heel load transfer
- Weight changes: Perimenopausal weight gain exacerbates plantar fasciitis and heel pad atrophy
- Inflammatory arthritis: Psoriatic arthritis and RA can present or worsen in the perimenopausal period
- Hypothyroidism: More prevalent in women 40-50; associated with tarsal tunnel syndrome and tendon degeneration
Diagnostic Approach Summary
| Step | Action |
|---|---|
| History | Location (plantar vs posterior), timing (morning stiffness, activity-related), bilateral vs unilateral, associated systemic symptoms |
| Exam | Localized tenderness mapping, heel squeeze test, Tinel's at tarsal tunnel, single heel-rise, neurological exam |
| X-ray | Rule out bony pathology (heel spur, calcaneal fracture, tumor); limited sensitivity |
| Ultrasound | First-line for plantar fasciitis, bursitis, tendinopathy |
| MRI | Stress fracture, PTTD, nerve entrapment, plantar fascia tear |
| Labs | ESR, CRP, RF, ANA, HLA-B27, uric acid if inflammatory or systemic cause suspected; TSH if neuropathic features |
Sources:
- Campbell's Operative Orthopaedics 15th Ed (2026), Chapter 88
- Rheumatology 2-Volume Set (Elsevier, 2022), Chapter 84
- Rosen's Emergency Medicine (9th Ed), Chapter 49
- Bailey & Love's Short Practice of Surgery (28th Ed), Chapter on Heel Pain
- Tedeschi R. "Baxter's nerve: the hidden culprit of chronic heel pain." Neurol Sci. 2025 Sep [PMID 40418415]
Aching pain on walking and tenderness on lateral aspect of dorsal surface of foot below lateral malleolus of 45 yrs old female
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Searching PubMed
"peroneal tendon" OR "sinus tarsi" lateral foot pain diagnosis
Reading File
Reading File
I have comprehensive data from multiple authoritative sources. Let me now compose the full answer.
Differential Diagnosis: Lateral Dorsal Foot Pain Below the Lateral Malleolus in a 45-Year-Old Woman
The area below and anterior to the lateral malleolus corresponds to the region of the peroneal tendons, sinus tarsi, calcaneocuboid joint, lateral ankle ligaments, and base of the fifth metatarsal. Pain with walking and point tenderness in this zone has a well-defined differential.
Anatomical Landmarks of the Region
Lateral Malleolus
|
↓
Peroneal tendons (behind & below the malleolus → curving forward)
Sinus tarsi (depression anterior to the malleolus)
Calcaneocuboid joint
Base of 5th metatarsal
Lateral ligament complex (ATFL, CFL, PTFL)
Priority Differential Diagnoses
1. Peroneal Tendinopathy (Tendinosis / Tenosynovitis) - TOP SUSPECT
The most likely chronic cause of aching lateral foot/ankle pain just below and posterior to the lateral malleolus in a middle-aged woman.
- Anatomy: The peroneus brevis and longus tendons run posterior to the lateral malleolus, held by the superior peroneal retinaculum, then curve below it toward their insertions (brevis to base of 5th metatarsal; longus crosses under the cuboid)
- Pain location: Posterolateral to the lateral malleolus, along the tendon course; may extend toward the base of the 5th metatarsal
- Symptoms: Aching pain on walking and standing, tenderness along the tendon sheath, may have swelling; worsens with activity
- Associations: Chronic lateral ankle instability, hindfoot varus, prior ankle sprains; peroneal tendons are the most common cause of chronic pain following an ankle sprain - Miller's Review of Orthopaedics
- Types: Tendinosis (degenerative), tenosynovitis (inflammatory), longitudinal split tears (especially peroneus brevis)
- Diagnosis: Ultrasound (first-line); MRI for tears; dynamic sonography for subluxation
- A 2026 systematic review on peroneal tendoscopy confirms peroneal tendon disorders as a frequent cause of lateral ankle and foot pain (PMID 41536605)
2. Peroneal Tendon Subluxation / Dislocation
- Subluxation/dislocation of the peroneal tendons are "uncommon and often overlooked causes of lateral ankle pain" - Campbell's Operative Orthopaedics (2026). Only 60% are accurately diagnosed at the first clinical evaluation.
- Mechanism: Failure of the superior peroneal retinaculum allows the tendons to snap anteriorly over the lateral malleolus
- Symptoms: Aching lateral pain, snapping or popping sensation, tenderness just posterior to the lateral malleolus; may be provoked by resisted eversion
- Exam: Ask patient to actively dorsiflex and evert the foot - tendon may visibly or palpably sublux
- Chronic cases: May occur without a specific traumatic event; insidious onset in older patients
- Key distinguishing feature from tendinopathy: Snapping/clicking sensation; palpable tendon displacement
3. Sinus Tarsi Syndrome
- The sinus tarsi is the anatomical hollow anterior to the lateral malleolus, between the talus and calcaneus
- Pain location: Directly over the sinus tarsi (the soft-tissue depression anterior to the lateral malleolus) - this matches the described location closely
- Symptoms: Pain and tenderness over the sinus tarsi, subjective hindfoot instability, aching worsened by walking on uneven ground
- Cause: Injury to the interosseous talocalcaneal ligament or subtalar joint; often follows an ankle sprain; fat atrophy or scarring in the sinus tarsi
- Pathognomonic feature: Pain is characteristically relieved by local anesthetic injection into the sinus tarsi - Bailey & Love's Surgery (28th Ed.)
- Diagnosis: Clinical + MRI (replacement of normal fat signal in sinus tarsi); diagnostic injection
4. Lateral Ankle Ligament Sprain / Chronic Lateral Instability
- Prior or ongoing injury to the lateral ligament complex (anterior talofibular ligament - ATFL, calcaneofibular ligament - CFL)
- In a 45-year-old woman, chronic/recurrent sprains may present with persistent aching below the lateral malleolus
- Symptoms: Recurrent giving way, pain on activity, tenderness over the ATFL (just anterior-inferior to the lateral malleolus)
- Exam: Anterior drawer test positive (ATFL), talar tilt test (CFL); stress X-rays
- Chronic instability leads to secondary peroneal tendinopathy, sinus tarsi syndrome, and osteochondral lesions
5. Fracture of the Anterior Process of the Calcaneus
- A frequently missed injury - the anterior process of the calcaneus is located just below and anterior to the lateral malleolus
- Mechanism: Inversion injury (plantarflexion + inversion); may be missed on standard X-rays
- Pain: Persistent lateral foot pain below/anterior to the lateral malleolus, worsened by walking
- Exam: Tenderness at the anterior process (more anterior than typical ankle sprain tenderness)
- Imaging: Oblique X-ray; CT most sensitive; may present as a chronic non-union if initial injury missed
- Campbell's includes this as a specific entity to recognize (Fig. 94.41 - fracture of anterior process of calcaneus)
6. Base of Fifth Metatarsal Pathology
The base of the 5th metatarsal is the insertion of the peroneus brevis tendon and lies on the lateral border of the foot just distal to the calcaneocuboid joint.
| Type | Details |
|---|---|
| Avulsion fracture (Zone 1) | Peroneus brevis pulls off the styloid process; common in ankle inversion injuries; point tender at the base |
| Jones fracture (Zone 2) | Stress fracture at the metaphyseal-diaphyseal junction; aching lateral foot pain with activity; risk increases with osteopenia in perimenopausal women |
| Stress fracture (Zone 3) | Diaphyseal; gradual onset, worst during and after running/walking; may have no obvious trauma |
7. Calcaneocuboid Syndrome / Cuboid Syndrome
- Pain and tenderness at the calcaneocuboid joint, which lies on the lateral border of the foot below and distal to the lateral malleolus
- Cuboid syndrome: Painful subluxation of the cuboid, seen in athletes and active women; patient may have a palpable "click" as the foot is brought from plantarflexion-inversion to dorsiflexion-eversion - Miller's Review of Orthopaedics
- Calcaneocuboid arthritis: Degenerative joint pain at this articulation, common in middle age
- Tenderness: Over the calcaneocuboid joint line (approximately 2-3 cm anterior to the lateral malleolus)
8. Osteochondral Lesion of the Talus (OLT)
- Cartilage and/or subchondral bone damage on the talar dome; lateral lesions present with lateral ankle/foot pain
- Symptoms: Deep aching pain, worsened by activity; may have mechanical symptoms (catching, locking)
- More common after ankle sprains; MRI is the gold standard for diagnosis
- Can co-exist with chronic lateral instability
9. Sural Nerve Neuritis / Entrapment
- The sural nerve runs lateral to the Achilles tendon, curves below the lateral malleolus, and continues along the lateral border of the foot to the 5th toe
- Symptoms: Burning, aching, or tingling lateral to the lateral malleolus and along the lateral foot border; Tinel's sign may be positive posterior to the lateral malleolus
- Causes: Direct trauma, tight footwear, ankle sprain, ganglion cyst
- More common in women; aggravated by walking
10. Tarsal Coalition (Less Common at 45 Years)
- Abnormal fusion (bony, cartilaginous, or fibrous) between tarsal bones - classically calcaneonavicular or talocalcaneal
- Usually symptomatic in adolescence, but can present or worsen in adulthood with increasing activity or weight gain
- Symptoms: Rigid flatfoot, pain with walking, restricted subtalar motion, lateral peroneal spasm
- Diagnosis: X-ray (oblique view for calcaneonavicular), CT for detail
11. Referred/Radicular Pain - L5 Radiculopathy
- L5 nerve root compression (disc prolapse) can refer pain to the lateral malleolus and dorsal foot/lateral foot
- Adams & Victor's Neurology (12th Ed.) specifically lists "lateral malleolus and great/second/third toe" in the L5 distribution: "L5-S1 disc... lateral thigh, anterolateral foreleg, dorsal foot, lateral malleolus"
- Clues: Associated low back pain, sciatic radiation, weakness of extensor hallucis longus (L5), sensory changes
- Exam: Straight-leg raise, neurological testing
Summary Table
| Diagnosis | Location of Tenderness | Key Features | Investigation |
|---|---|---|---|
| Peroneal tendinopathy | Posterior to lateral malleolus, along tendon | Aching, worsens with activity, no snapping | Ultrasound, MRI |
| Peroneal tendon subluxation | Posterior to lateral malleolus | Snapping/clicking, tendon visible subluxing | Dynamic US |
| Sinus tarsi syndrome | Anterior to lateral malleolus (soft depression) | Hindfoot instability, relieved by injection | MRI, diagnostic injection |
| Lateral ankle ligament sprain | Over ATFL (anteroinferior to malleolus) | Instability, prior sprains | Stress X-ray, MRI |
| Anterior process calcaneus fracture | Anterior/inferior to malleolus | Often missed, after inversion injury | CT, oblique X-ray |
| Base of 5th metatarsal fracture | Lateral border at base of 5th MT | Acute after inversion OR insidious stress fracture | X-ray |
| Cuboid/calcaneocuboid syndrome | 2-3 cm anterior to malleolus | Click on eversion, lateral column pain | X-ray, MRI |
| Osteochondral lesion of talus | Deep joint line | Catching, mechanical symptoms | MRI |
| Sural neuritis | Along lateral malleolus → lateral foot | Burning/tingling, Tinel's positive | Clinical, nerve conduction |
| L5 radiculopathy | Diffuse lateral/dorsal foot | Back pain, dermatomal, weakness of EHL | MRI spine, EMG |
Age/Sex Considerations for this Patient (45-Year-Old Woman)
- Perimenopausal osteopenia: Raises risk of stress fractures (5th metatarsal, anterior process calcaneus) - bone mineral density assessment may be relevant
- Chronic ankle instability: Often underreported in women; leads to secondary peroneal tendinopathy and sinus tarsi syndrome
- Footwear: High heels and narrow shoes strain the peroneal tendons and lateral foot structures
- Inflammatory arthritis: Psoriatic arthritis and seronegative spondyloarthropathy should be considered if bilateral, if there is morning stiffness >30 min, or if systemic symptoms are present
- Hypermobility: More prevalent in women; predisposes to peroneal tendon and lateral ligament instability
Recommended Initial Work-Up
| Step | Action |
|---|---|
| History | Onset (acute vs. chronic), prior ankle sprains, footwear, activity level, systemic symptoms |
| Exam | Map tenderness precisely (posterior, anterior, or inferior to malleolus), test subtalar motion, eversion/inversion, peroneal tendon resisted eversion test, Tinel's behind malleolus |
| X-ray (weight-bearing) | Oblique view for 5th metatarsal base, anterior process calcaneus; lateral for sinus tarsi |
| Ultrasound | First-line for peroneal tendon pathology (tendinosis, tears, subluxation) |
| MRI | Definitive for OLT, sinus tarsi syndrome, ligament tears, stress fractures |
| Diagnostic injection | Sinus tarsi injection with local anesthetic - diagnostic and therapeutic |
| Neurology referral / MRI spine | If radicular pattern suspected |
Sources:
- Campbell's Operative Orthopaedics 15th Ed (2026), Chapters 53 & 88 & 94
- Miller's Review of Orthopaedics 9th Ed - Section 12, Tendon Disorders
- Bailey & Love's Short Practice of Surgery 28th Ed, Chapter 41
- Adams & Victor's Principles of Neurology 12th Ed, Table 10-1
- Tham A et al. "Peroneal tendoscopy for peroneal tendon disorders." J Orthop. 2026 (PMID 41536605)
This is a shared conversation. Sign in to Orris to start your own chat.