Describe facial nerve under the head. ... endings of its nuclei and extracranial course, its sensations. And applied.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed to write a comprehensive answer. Here it is:
Facial Nerve (CN VII) - Complete Account
1. Overview and Fiber Types
The facial nerve (7th cranial nerve) innervates structures derived from Reichert's cartilage (2nd pharyngeal arch). Its trunk carries five distinct fiber types:
| Fiber Type | Function | Target |
|---|---|---|
| Special Visceral Efferent (SVE) | Motor to muscles of facial expression, stapedius, stylohyoid, posterior belly of digastric | Branchiomotor |
| General Visceral Efferent (GVE) | Parasympathetic secretomotor | Lacrimal, nasal seromucinous, submandibular, sublingual glands |
| Special Visceral Afferent (SVA) | Taste | Anterior 2/3 of tongue, tonsillar fossa, posterior palate |
| General Somatic Afferent (GSA) | Cutaneous sensation | External auditory canal (EAC), concha, skin near mastoid |
| General Visceral Afferent (GVA) | Visceral sensation | Mucosa of nose, pharynx, palate |
The sensory and parasympathetic fibers travel together as the nervus intermedius (nerve of Wrisberg), which lies between the motor root of CN VII and CN VIII as they exit the brainstem.
- Shambaugh Surgery of the Ear, p. 68
- Localization in Clinical Neurology, 8e, p. 775
2. Nuclei and Their Endings
Three nuclei give rise to the fibers of CN VII:
A. Motor Nucleus (SVE)
- Located in the ventrolateral caudal pontine tegmentum, dorsal to the superior olive, medial to the spinal trigeminal nucleus, anterolateral to the abducens nucleus.
- Organized into four subnuclei:
- Dorsomedial group - auricular and occipital muscles
- Intermediate group - frontalis and corrugator
- Ventromedial group - platysma
- Lateral group - buccinator and buccolabial muscles
- (Orbicularis oculi neurons lie in a cap at the dorsolateral margin)
- Intrapontine roots travel rostrally and dorsally to the level of the abducens nucleus, then sweep around the dorsal surface of the abducens nucleus - this loop creates the facial colliculus, which bulges into the floor of the 4th ventricle (the "internal genu").
- The fascicles then course ventrolaterally and caudally to emerge on the lateral aspect of the lower pons (pontomedullary sulcus).
Supranuclear (UMN) control: Corticobulbar fibers from the lower 1/3 of the precentral gyrus descend via corona radiata, genu of internal capsule, and medial cerebral peduncle. Most cross to the contralateral facial nucleus. Critically:
- The upper face (frontalis, orbicularis oculi) receives bilateral input - from both the ipsilateral AND contralateral cortex.
- The lower face receives predominantly crossed input only.
B. Superior Salivatory Nucleus (GVE - parasympathetic)
- Located dorsal to the motor nucleus in the pontine tegmentum.
- Preganglionic fibers travel in the nervus intermedius, then split into two pathways:
- Greater petrosal nerve → pterygopalatine ganglion → lacrimal, nasal, and palatal glands
- Chorda tympani → submandibular ganglion → submandibular and sublingual glands
- An associated lacrimal nucleus controls reflex lacrimation specifically.
C. Nucleus of the Tractus Solitarius (SVA - taste)
- Located in the medulla oblongata.
- Receives gustatory afferents from the anterior 2/3 of the tongue via the chorda tympani; also from the tonsillar fossa and posterior palate.
Note on somatic afferent endings: GSA fibers have their cell bodies in the geniculate ganglion and central processes end in the nucleus of the spinal tract of CN V (trigeminal). Some proprioceptive afferents from facial muscles end in the mesencephalic trigeminal nucleus.
- Localization in Clinical Neurology, 8e, p. 775-777
- Shambaugh Surgery of the Ear, p. 68
3. Course of the Facial Nerve
Intracranial Segments (Five segments total)
1. Intracranial (cisternal) segment - 24 mm
- From the lateral aspect of the lower pons (pontomedullary sulcus) to the porus of the internal auditory canal (IAC).
- Travels through the cerebellopontine angle (CPA) alongside CN VIII and the internal auditory artery.
- The nervus intermedius lies between the motor root and CN VIII.
2. Intracanalicular (meatal) segment
- Traverses the IAC.
- CN VII occupies the anterosuperior quadrant at the fundus, above the cochlear nerve (superior and inferior vestibular nerves are posteriorly placed).
- At the lateral end, the nervus intermedius joins the main trunk.
3. Labyrinthine segment - 4 mm (shortest)
- From the beginning of the fallopian (facial) canal to the geniculate ganglion.
- Runs between the cochlea and vestibule through the narrowest portion of the bony canal.
- The subarachnoid space of CN VII usually ends here.
4. Tympanic (horizontal) segment - ~13 mm
- From the geniculate ganglion (1st genu, where it turns posteriorly) through the medial wall of the tympanic cavity.
- Runs superior to the cochleariform process and oval window.
- At the 2nd genu (just inferior to the lateral semicircular canal), the nerve turns inferiorly.
- This segment is most prone to dehiscence (bony gaps in the fallopian canal): ~66% of dehiscences occur here over the oval window, bilateral in ~75% of cases.
5. Mastoid (vertical) segment - ~20 mm
- From the 2nd genu to the stylomastoid foramen.
Intratemporal Branches
Three branches arise within the temporal bone:
-
Greater petrosal nerve - arises from the anterior aspect of the geniculate ganglion; carries preganglionic parasympathetic fibers for lacrimation and nasal glands. Emerges through the facial hiatus onto the floor of the middle cranial fossa, runs under the gasserian ganglion, enters the vidian canal → pterygopalatine ganglion.
-
Nerve to stapedius - arises from the mastoid segment near the pyramidal eminence; supplies the stapedius muscle (dampens loud sounds).
-
Chorda tympani - arises ~4 mm proximal to the stylomastoid foramen; carries taste fibers from the anterior 2/3 of tongue and preganglionic parasympathetics to the submandibular and sublingual glands. It ascends in the temporal bone, enters the tympanic cavity via the iter chordae posterius, crosses lateral to the long process of the incus and medial to the malleus (handle), and exits via the iter chordae anterius (canal of Huguier) through the petrotympanic (glaserian) fissure.
4. Extracranial Course
After exiting through the stylomastoid foramen, the facial nerve is now a purely motor nerve. It gives off:
- Posterior auricular nerve - supplies the occipital belly of occipitofrontalis and the auricular muscles
- Branch to posterior belly of digastric and stylohyoid
The main trunk then swings anteriorly and enters the parotid gland on its posteromedial surface, passing forwards and downwards behind the mandibular ramus. The trunk length from the stylomastoid foramen to the first intraparotid division ranges 8-22 mm.
Within the parotid, it divides into:
- Upper temporofacial trunk
- Lower cervicofacial trunk
These further branch and anastomose to form the parotid plexus (pes anserinus), giving five terminal groups that emerge from the anterosuperior and inferior borders of the gland:
| Branch | Supply |
|---|---|
| Temporal | Frontalis, orbicularis oculi, corrugator supercilii |
| Zygomatic | Orbicularis oculi (lower portion), zygomaticus |
| Buccal | Buccinator, muscles of the upper lip and nose |
| Marginal mandibular | Muscles of the lower lip and chin |
| Cervical | Platysma |
The facial nerve also has extensive anastomotic connections with all three divisions of the trigeminal nerve, with CN VIII, CN IX, CN X, and with the cervical plexus - clinically important for perineural spread of malignancy.
- Scott-Brown's Otorhinolaryngology, Vol. 2, p. 1425-1426
- Gray's Anatomy for Students, p. 1052
5. Sensations Carried by CN VII
CN VII's sensory role is carried by the nervus intermedius via the geniculate ganglion:
| Sensation | Pathway | Origin |
|---|---|---|
| Taste (SVA) | Chorda tympani → nervus intermedius → nucleus tractus solitarius | Anterior 2/3 of tongue |
| Taste from palate | Greater petrosal nerve → geniculate ganglion → nucleus tractus solitarius | Soft palate, tonsillar fossa |
| Cutaneous sensation (GSA) | Nervus intermedius → nucleus of spinal tract of CN V | EAC, auricle, mastoid skin (Ramsay Hunt zone) |
| Visceral sensation (GVA) | Nervus intermedius | Mucosa of nose, pharynx, palate |
| Proprioception | Via mesencephalic trigeminal nucleus | Facial muscles (modified mechanoreceptors, not spindles) |
6. Applied Anatomy
A. UMN vs. LMN Facial Palsy (The Most Important Clinical Distinction)
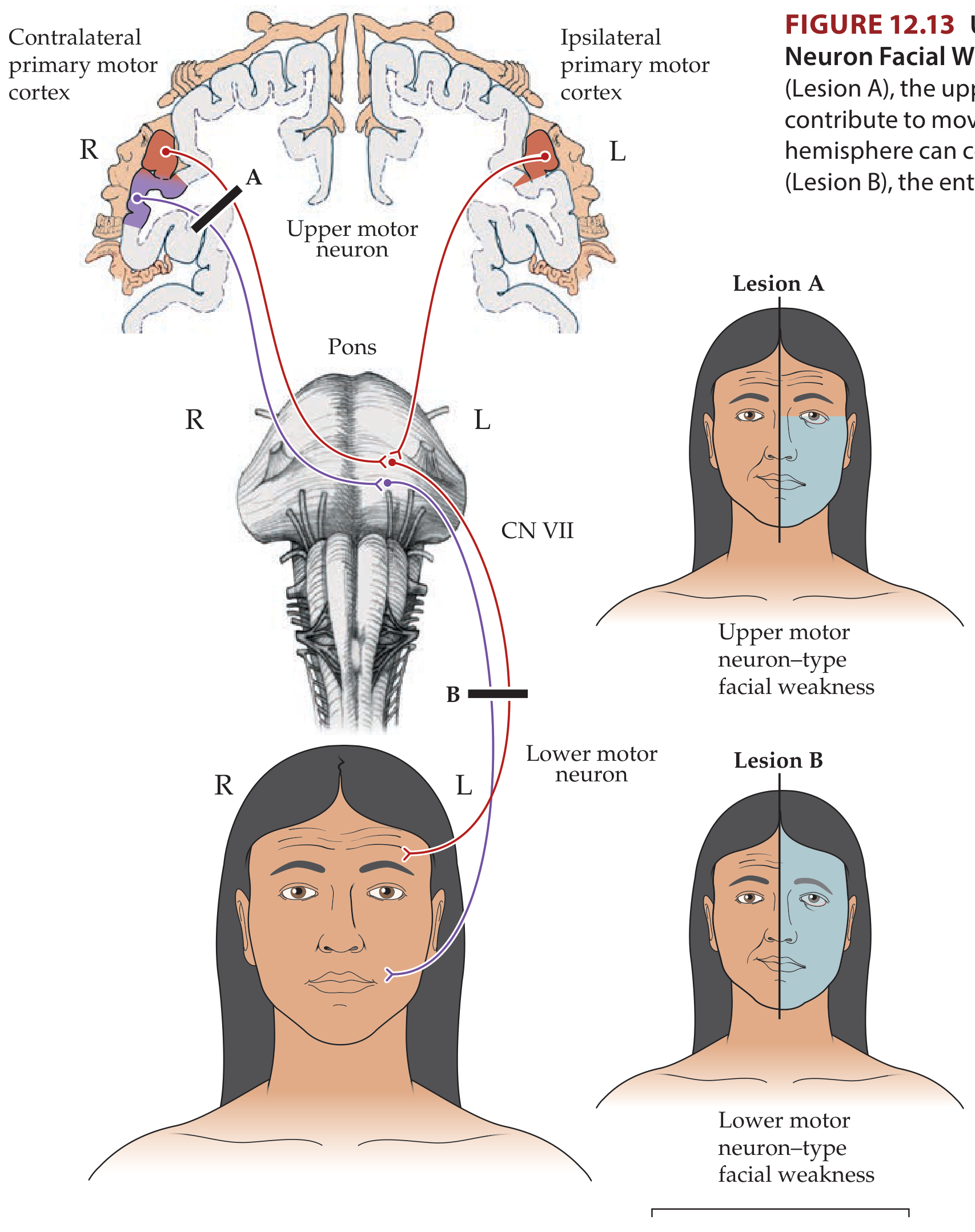
Neuroanatomy Through Clinical Cases, Figure 12.13
| Feature | UMN Lesion (Lesion A) | LMN Lesion (Lesion B) |
|---|---|---|
| Side affected | Contralateral lower face | Ipsilateral entire face |
| Forehead | Spared (bilateral cortical input) | Affected (no sparing) |
| Orbicularis oculi | Mildly affected (slight widened palpebral fissure) | Paralyzed - patient cannot close eye |
| Taste, lacrimation | Normal | Reduced if nerve involved proximal to chorda tympani/greater petrosal nerve |
| Hyperacusis | Absent | Present if stapedius branch involved |
| Associated features | Arm/leg weakness, aphasia, dysensory loss | Usually isolated |
Bell phenomenon - on attempting eye closure in LMN palsy, the eyeball deviates up and out (contraction of superior rectus, relaxation of inferior rectus) - a normal reflex made visible by orbicularis paralysis.
B. Bell's Palsy
- The most common facial nerve disorder.
- All divisions of CN VII are affected (full LMN pattern).
- Acute onset over hours to days, then gradual recovery.
- Presumed viral/inflammatory etiology (herpes simplex virus most likely).
- Features: unilateral LMN facial weakness, retroauricular pain (GSA involvement), hyperacusis (stapedius), reduced taste (chorda tympani), dry eye (parasympathetic involvement).
- Treatment: 10-day course of oral corticosteroids started early improves complete recovery; role of antivirals remains uncertain.
- Eye care critical - artificial tears, taping eyelid closed at night to prevent corneal exposure.
C. Ramsay Hunt Syndrome (Herpes Zoster Oticus)
- Reactivation of VZV in the geniculate ganglion.
- Triad: LMN facial palsy + otalgia + vesicular eruption in the external auditory canal / pinna (Ramsay Hunt zone - the sensory territory of CN VII).
- Occasionally vesicles on the anterior 2/3 of the tongue (chorda tympani territory) or palate.
- Prognosis is worse than Bell's palsy; only ~50% recover fully without treatment.
- Treatment: combined aciclovir (antiviral) + corticosteroids; early treatment reduces long-term sequelae.
D. Pontine Syndromes (Nuclear/Fascicular Lesions)
Because the facial nerve fascicles loop around the abducens nucleus, pontine lesions typically involve both CN VI and CN VII together:
- Millard-Gubler syndrome (ventral pons): ipsilateral peripheral facial palsy + ipsilateral lateral rectus palsy + contralateral hemiplegia (corticospinal tract).
- Foville syndrome (pontine tegmentum): ipsilateral peripheral facial palsy + ipsilateral conjugate gaze palsy (PPRF) + contralateral hemiplegia.
- Eight-and-a-Half syndrome: ipsilateral peripheral facial palsy + one-and-a-half syndrome (INO + horizontal gaze palsy).
- Moebius syndrome: congenital agenesis of the facial nucleus and abducens nucleus together (bilaterally) - bilateral facial diplegia and failure of abduction.
E. Surgical Landmarks for Identifying CN VII
During parotidectomy or mastoid surgery:
- Tragal pointer - the main trunk lies ~1 cm medial and inferior to the medial aspect of the tragus.
- Tympanomastoid suture - trunk can be found 6-8 mm below the inferior "drop off" of this suture.
- Posterior belly of digastric - the nerve lies just superior and superficial at this level.
- Facial recess - triangular area bounded by: facial nerve (posterior), chorda tympani (anterior), and incudal fossa (superior) - used in intact canal wall mastoidectomy.
F. Parotidectomy Risk
The intimate relationship of CN VII with the parotid gland makes parotid surgery one of the highest-risk procedures for facial nerve injury. All 5 terminal branches must be individually preserved. Intraoperative nerve monitoring is standard practice. Accidental division of a single branch in a plexiform pattern nerve often causes minimal deficit due to cross-innervation, but injury to the main trunk is catastrophic.
G. Chorda Tympani Injury in Middle Ear Surgery
During myringoplasty, stapedectomy, or ossiculoplasty, the chorda tympani can be stretched or cut - resulting in:
- Loss of taste on the ipsilateral anterior 2/3 of tongue
- Dry mouth (reduced submandibular/sublingual secretion)
- Some patients also report unpleasant metallic tastes
H. Greater Petrosal Nerve - "Crocodile Tears" (Gustatory Lacrimation)
After proximal CN VII injuries (proximal to the geniculate ganglion), misdirected regeneration of parasympathetic fibers originally destined for the salivary glands can reinnervate the lacrimal gland. The result: the patient sheds tears while eating (Frey's syndrome / crocodile tears).
Sources:
- Shambaugh Surgery of the Ear (facial nerve anatomy, pp. 68-69)
- Localization in Clinical Neurology, 8e (nuclei, supranuclear control, pontine syndromes, pp. 775-783)
- Neuroanatomy Through Clinical Cases, 3rd ed. (UMN/LMN distinction, Bell's palsy, pp. 543-544, 269-270)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 2 (extracranial course, surgical landmarks, pp. 1425-1426)
- Gray's Anatomy for Students (extracranial course, parotid relationships, p. 1052)
- Cummings Otolaryngology Head and Neck Surgery (intratemporal segments and branches)
A short note on financial constructors. No pharyngeal constructors.
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I have all the material needed. Here is the short note:
Pharyngeal Constrictors - A Short Note
Overview
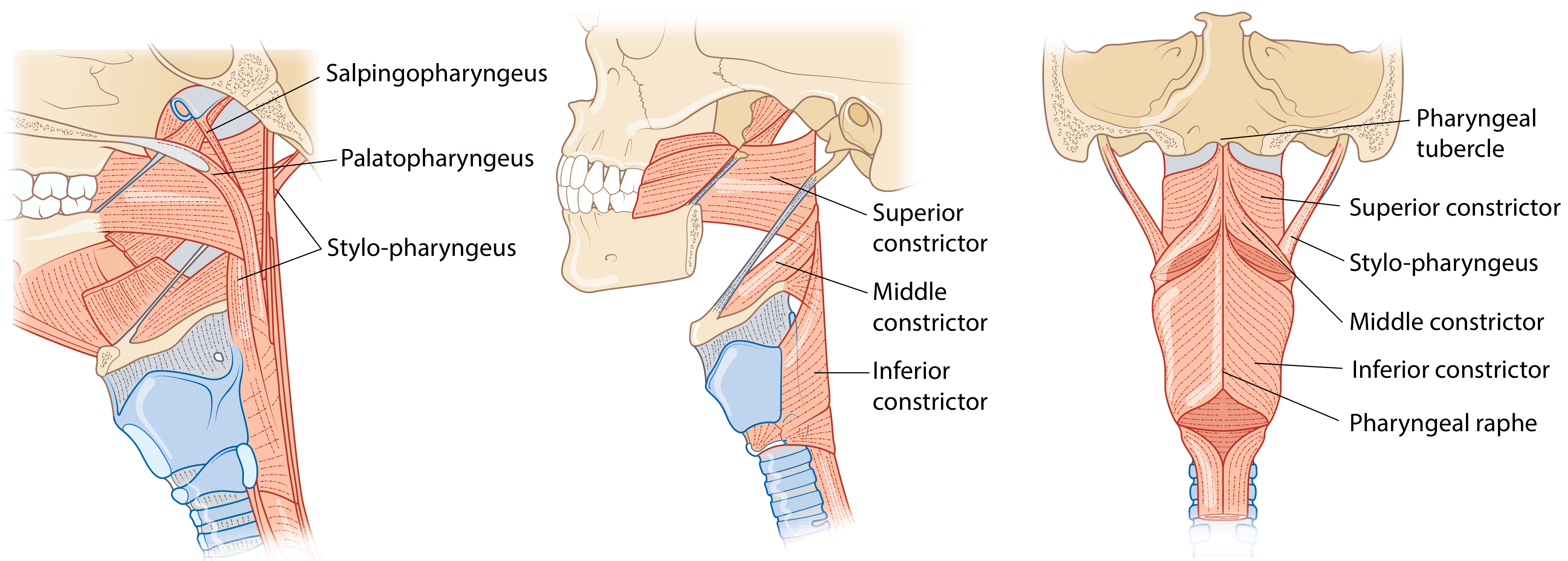
The pharyngeal constrictors are three overlapping flat muscles that form the outer (circular) muscular layer of the posterior and lateral pharyngeal walls. Their function is to sequentially narrow the pharyngeal cavity from top to bottom, propelling a food bolus into the esophagus. All three insert posteriorly into the median pharyngeal raphe (a fibrous band attached above to the pharyngeal tubercle of the basiocciput). All are innervated by the vagus nerve (CN X) via the pharyngeal plexus.
The Three Constrictors
1. Superior Constrictor
- Origin: Pterygomandibular raphe (a tendinous band between the pterygoid hamulus and mandible), adjacent mandible, medial pterygoid plate, and base of tongue.
- Insertion: Median pharyngeal raphe and pharyngeal tubercle of the basiocciput.
- Notes:
- The uppermost part of the posterior pharyngeal wall above the superior constrictor is not muscular - it is covered only by the pharyngobasilar fascia, which firmly anchors the wall to the skull base. This is a potential site of weakness.
- Passavant's ridge - a visible transverse ridge formed by contraction of the superior margin of the superior constrictor during swallowing, which meets the soft palate to close off the nasopharynx (velopharyngeal closure).
2. Middle Constrictor
- Origin: Greater and lesser horns of the hyoid bone and stylohyoid ligament.
- Insertion: Median pharyngeal raphe.
- Notes:
- Fan-shaped; its upper fibers overlap the superior constrictor externally, while its lower fibers are overlapped by the inferior constrictor.
- The thyrohyoid membrane fills the gap between the middle and inferior constrictors anterolaterally - the internal laryngeal nerve and superior laryngeal artery/vein pierce through this membrane to reach the larynx.
3. Inferior Constrictor
- Origin: Oblique line of the thyroid lamina (and a small part of the inferior thyroid horn) = thyropharyngeus part; lateral aspect of the cricoid cartilage = cricopharyngeus part.
- Insertion: Median pharyngeal raphe (thyropharyngeus portion). Cricopharyngeus does not fuse at the midline raphe.
- Notes:
- Thickest of all three constrictors.
- Divided into two functional parts:
| Part | Origin | Character |
|---|---|---|
| Thyropharyngeus | Oblique line of thyroid cartilage | Flat, oblique fibers; inserts into raphe |
| Cricopharyngeus | Cricoid cartilage | Thick, horizontal, circular - acts as UES |
Cricopharyngeus - The Upper Esophageal Sphincter (UES)
The cricopharyngeus is distinct from all other constrictors:
- Its fibers run horizontally and encircle the cricoid arch without fusing at the pharyngeal raphe - forming a true sphincter.
- It is tonically contracted at rest (keeping the esophagus closed and preventing air entry).
- It relaxes momentarily during swallowing, triggered by laryngeal elevation.
- The UES is composed of the cricopharyngeus primarily, along with the inferior pharyngeal constrictor above and the cervical esophagus below.
Killian's Triangle and Zenker's Diverticulum
Between the oblique fibers of the thyropharyngeus and the horizontal fibers of the cricopharyngeus lies an area of muscular weakness called Killian's dehiscence (triangle of Killian). This is a site of least resistance in the posterior pharyngeal wall.
- With age and repeated elevated intraluminal pressure during swallowing, the mucosa and submucosa can herniate posteriorly through this weak point - forming a Zenker's (pharyngo-esophageal) diverticulum.
- Symptoms: progressive dysphagia, regurgitation of undigested food, halitosis, aspiration risk.
- Note: Killian-Jamieson space is a separate, lateral dehiscence inferior to the cricopharyngeus, through which branches of the inferior thyroid artery pass; a Killian-Jamieson diverticulum (anterolateral) can also develop here.
Gaps Between the Constrictors
The constrictors do not form a complete muscular tube - several important structures pass through the gaps between them:
| Gap | Structures Passing Through |
|---|---|
| Above superior constrictor | Auditory tube (Eustachian tube), levator veli palatini |
| Between superior and middle | Stylopharyngeus muscle, glossopharyngeal nerve (CN IX), stylohyoid ligament |
| Between middle and inferior | Internal laryngeal nerve, superior laryngeal artery and vein (via thyrohyoid membrane) |
| Below inferior constrictor | Recurrent laryngeal nerve, inferior laryngeal artery |
Innervation and Blood Supply
- Motor: Vagus nerve (CN X) via the pharyngeal plexus (for all three constrictors). The external laryngeal nerve (branch of CN X) also gives motor branches to the inferior constrictor.
- Sensory: Glossopharyngeal nerve (CN IX) and vagus nerve via the pharyngeal plexus.
- Blood supply: Ascending pharyngeal artery, tonsillar and ascending palatine branches of the facial artery, and branches of the superior thyroid artery.
Applied Points
- Parotidectomy / deep neck surgery: The superior constrictor forms the deep medial wall of the parotid bed; deep lobe parotid tumors can displace it medially.
- Tonsillectomy: The tonsillar branch of the facial artery pierces the superior constrictor to enter the inferolateral tonsil - a major bleeding point.
- Endoscopy: The tonically contracted cricopharyngeus is the most common site of resistance when passing an endoscope into the esophagus; swallowing by the patient helps overcome this.
- Dysphagia: Failure of cricopharyngeal relaxation (achalasia of the UES) causes transfer dysphagia and can lead to Zenker's diverticulum.
- Radiotherapy: The constrictors lie in the radiation field for head and neck cancers - post-radiotherapy fibrosis causes severe dysphagia and aspiration.
Sources: K.J. Lee's Essential Otolaryngology; Scott-Brown's Otorhinolaryngology, Vol. 1; Cummings Otolaryngology Head and Neck Surgery
This is a shared conversation. Sign in to Orris to start your own chat.