Becks triad
Reading File
Finding Sources
Searching Images
Beck's triad cardiac tamponade
Reading File
Reading File
Beck's Triad
Beck's Triad is the classic clinical presentation of acute cardiac tamponade, first described by Claude Beck in 1935. It comprises three signs:
| Component | Mechanism |
|---|---|
| Hypotension (low blood pressure) | Pericardial fluid compresses the heart → decreased ventricular filling → reduced stroke volume → decreased cardiac output |
| Distended neck veins (elevated JVP/CVP) | Impaired right ventricular filling → venous back-pressure |
| Muffled/distant heart sounds | Fluid surrounding the heart dampens transmitted sounds |
Pathophysiology
Cardiac tamponade occurs when fluid accumulates in the pericardial sac faster than the pericardium can stretch. This raises intrapericardial pressure, compresses the cardiac chambers (especially the thin-walled right heart), and impairs diastolic filling. Stroke volume falls, and the heart compensates initially with tachycardia — but rapid decompensation follows.
The most important factor is the rate of accumulation, not just the volume. A rapidly accumulating 150 mL can cause tamponade, whereas a slowly accumulating 1000 mL may not.
Important Caveats
- Only ~33% of patients with cardiac tamponade present with the complete triad — so its absence does not rule out tamponade
- Almost 90% have at least one of the three signs
- The complete triad usually appears shortly before cardiac arrest (i.e., it's a very late finding)
- In hypovolemic patients, neck vein distension may be absent
- Muffled heart sounds are the least reliable sign
Beck's Two Triads (Historical Note)
Beck actually described two triads:
| Triad | Signs | Context |
|---|---|---|
| Acute triad (Beck's Triad) | ↑ CVP + ↓ arterial pressure + muffled heart sounds | Acute cardiac compression |
| Chronic triad | ↑ CVP + ascites + small quiet heart | Chronic pericardial effusion |
Causes of Cardiac Tamponade
- Malignancy (32%) — lung, breast, lymphoma
- Infection (24%) — TB, staph, HIV
- Idiopathic (16%)
- Iatrogenic (15%) — post-catheterization, post-cardiac surgery, anticoagulants
- Post-MI free wall rupture (7%)
- Uraemic pericarditis (4%)
Supporting Diagnostic Findings
| Test | Finding |
|---|---|
| ECG | Sinus tachycardia, electrical alternans (beat-to-beat QRS axis variation), low voltage |
| CXR | Globular "water bottle" cardiac silhouette (if >250 mL fluid) |
| Echo (POCUS) | Pericardial effusion + right-sided chamber collapse in diastole — diagnostic |
| Cardiac cath | Equalization of right and left ventricular diastolic pressures |
Pulsus paradoxus (>10 mmHg drop in systolic BP during inspiration) is an additional bedside sign.
Management
- IV fluids — increases right-sided filling pressure to temporarily overcome pericardial compression
- Pericardiocentesis — definitive treatment; needle drainage of pericardial fluid
- Surgical pericardiotomy — for recurrent or loculated effusions
Echocardiogram Images of Cardiac Tamponade
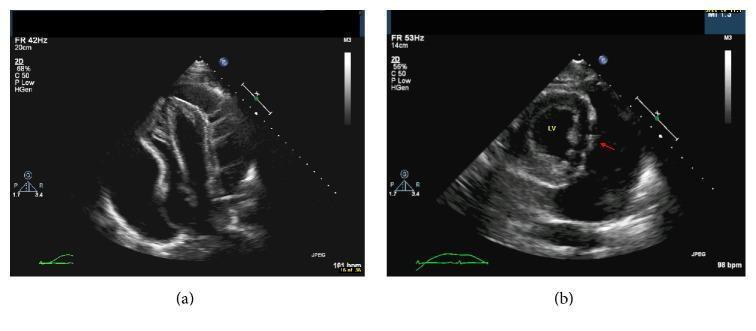
Apical 4-chamber echo: circumferential pericardial effusion (anechoic space) with collapse of the right atrium and right ventricle — hallmark of tamponade.
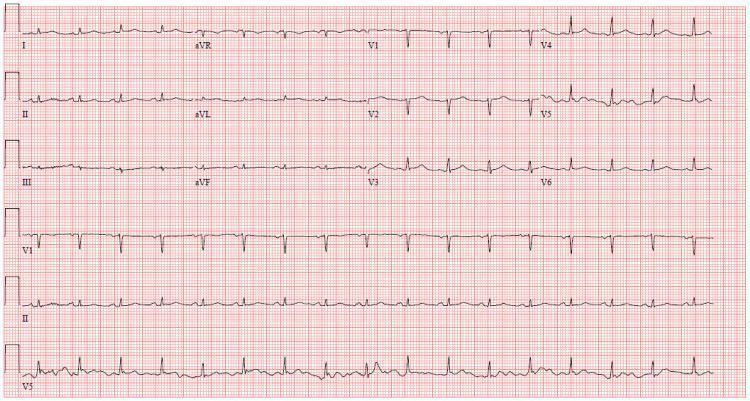
ECG: sinus tachycardia + electrical alternans (beat-to-beat QRS variation) — classic ECG pattern of cardiac tamponade.
Sources: Roberts & Hedges' Clinical Procedures in Emergency Medicine; Rosen's Emergency Medicine; The Washington Manual of Medical Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.