How to identify thrombus or scad in CAG
Reading File
Finding Sources
Finding Sources
Searching PubMed
thrombus SCAD coronary angiography differentiation
Reading File
Reading File
Finding Sources
Searching PubMed
spontaneous coronary artery dissection angiographic diagnosis
Reading File
Finding Sources
Loading Image
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
thrombus vs SCAD coronary angiography differentiation features identification
Excellent. I now have comprehensive information from both the textbooks and the web. Let me compile the full answer.
Identifying Thrombus vs. SCAD on Coronary Angiography (CAG)
These two entities can produce nearly identical clinical presentations (ACS, chest pain, troponin rise), but their management is fundamentally different - thrombus is treated with anticoagulation/PCI while SCAD is often managed conservatively. Accurate identification on CAG is therefore critical.
Part 1: Identifying Intracoronary Thrombus on CAG
Thrombus is visible by angiography in only about one-third of patients with ACS - coronary angioscopy detects it in the majority, so a negative CAG does not exclude thrombus (Goldman-Cecil Medicine).
Angiographic features of thrombus:
| Feature | Description |
|---|---|
| Intraluminal filling defect | A discrete lucency (dark area) within the contrast-filled lumen, surrounded by contrast on ≥3 sides |
| Haziness / cloudiness | A "hazy" or "blurred" appearance at the lesion site without a clear discrete defect |
| Irregular eccentric lesion | Asymmetric lesion with scalloped or overhanging edges and narrow neck - reflects plaque rupture + thrombus |
| Total occlusion | Abrupt cutoff, often with convex (meniscus-shaped) proximal edge |
| Contrast "staining" | Persistent contrast pooling at the lesion site after injection clears |
| Slow/absent flow | TIMI 0-2 flow distal to the occlusion |
| Haziness that clears with anticoagulation | Suggestive of fresh thrombus |
TIMI Thrombus Grading Scale:
| Grade | Description |
|---|---|
| 0 | No thrombus |
| 1 | Possible thrombus (hazy area, reduced density, irregular contour) |
| 2 | Small thrombus (<1/2 vessel diameter) |
| 3 | Moderate thrombus (0.5-2x vessel diameter) |
| 4 | Large thrombus (>2x vessel diameter) |
| 5 | Total thrombotic occlusion |
The culprit lesion of thrombus is often NOT severely stenotic - two-thirds of culprit lesions previously had <50% luminal narrowing on prior angiograms. (Goldman-Cecil Medicine, p.2709)
Part 2: Identifying SCAD on CAG
SCAD is caused by separation of the coronary artery wall layers creating a false lumen / intramural hematoma (IMH) that compresses the true lumen. It occurs most often in young women without traditional cardiovascular risk factors. The LAD is most commonly affected (52%), followed by Cx (38%) and RCA (23%). - Fuster and Hurst's The Heart, 15th Ed.
The Saw Classification - 3 Angiographic Types:
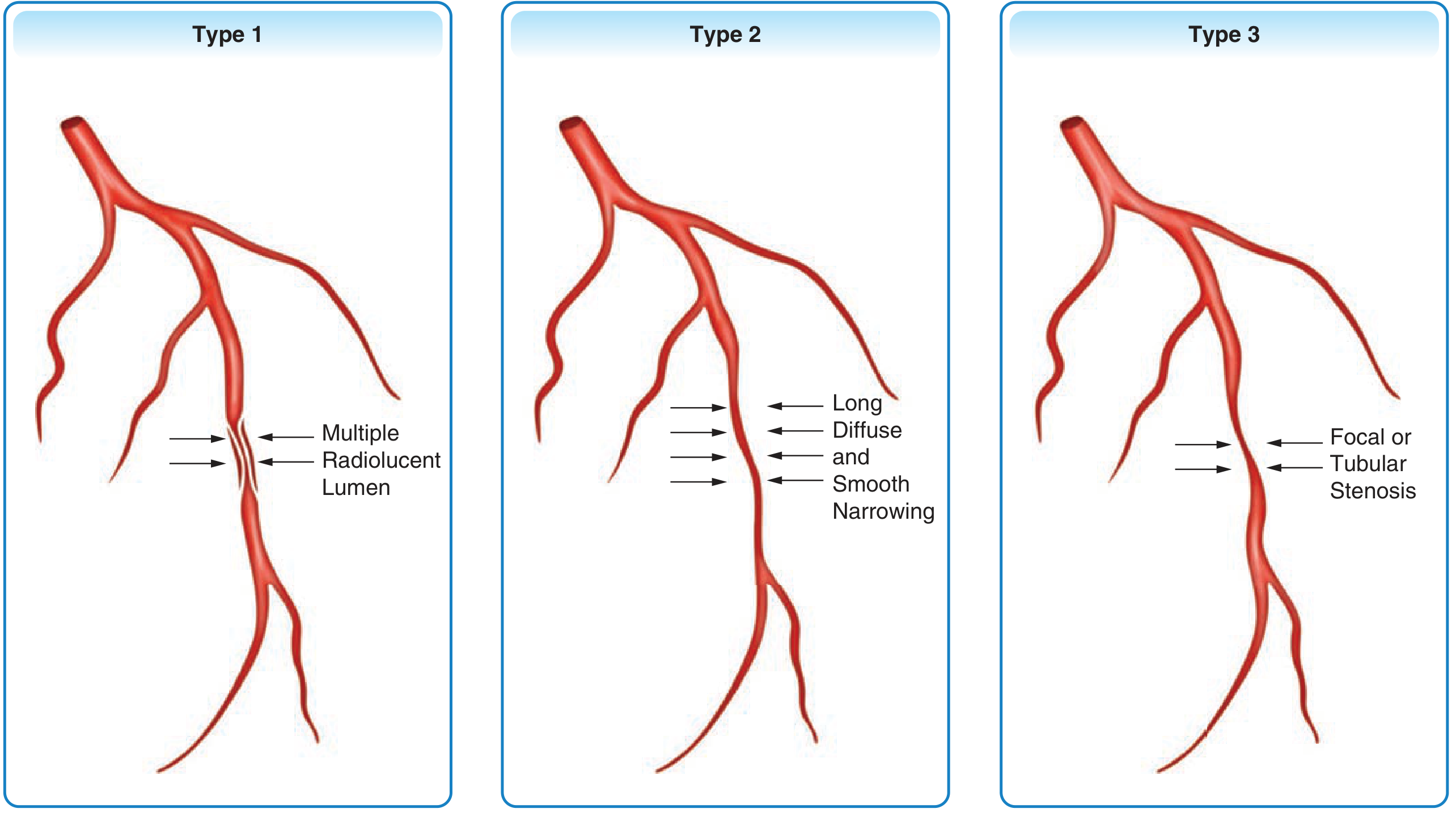
(Saw J, et al. J Am Coll Cardiol. 2017;70(9):1148-1158 - from Fuster and Hurst's The Heart, 15th Ed.)
Type 1 SCAD (29% of cases) - Pathognomonic, easiest to identify
- Multiple radiolucent lumens visible within the vessel
- Contrast staining of the artery wall (contrast enters the false lumen)
- Haziness or "hang-up" of contrast dye in the vessel wall
- Classic double-lumen appearance with an intimal flap
- Confirms SCAD without intracoronary imaging
Type 2 SCAD (60% of cases) - Most common, often missed
- Long, diffuse, smooth stenosis (typically >20 mm, often 20-60 mm)
- Smooth-walled narrowing without the irregular features of atherosclerosis
- Can be Type 2A: normal-caliber vessel proximal AND distal to the stenosis
- Type 2B: dissection extends to the distal tip of the vessel
- No visible intimal flap - the IMH compresses the lumen externally
- Easily mistaken for long atherosclerotic stenosis or vasospasm
Type 3 SCAD (11% of cases) - Mimics atherosclerosis, hardest to diagnose
- Focal or tubular stenosis (<20 mm)
- Looks identical to focal atherosclerotic plaque
- Requires intracoronary OCT/IVUS to confirm IMH or double-lumen
- Features that favor SCAD over atherosclerosis: absence of atherosclerosis elsewhere, younger patient, hazy stenosis, linear stenosis pattern
Type 4 SCAD (newer addition)
- Total occlusion of the vessel
- Must be differentiated from thromboembolic event
- Cannot be distinguished from thrombus by CAG alone - needs intracoronary imaging
Part 3: Key Differentiating Features - Thrombus vs. SCAD
| Feature | Thrombus | SCAD |
|---|---|---|
| Angiographic appearance | Intraluminal filling defect, discrete haziness, abrupt occlusion with meniscus sign | Radiolucent false lumen (Type 1), long smooth stenosis (Type 2), focal stenosis (Type 3) |
| Vessel wall | Normal wall outside the thrombus | Thickened wall due to IMH compressing lumen from outside |
| Lesion length | Usually short, focal | Typically long (mean 33mm in SCAD) |
| Edges | Irregular, scalloped, overhanging (plaque rupture) | Smooth, tapering edges (Type 2) |
| Contrast clearing | Filling defect persists within lumen | Contrast staining of wall (Type 1); lumen narrowing persists (Type 2/3) |
| Multiple lumens | No | Yes (Type 1 - pathognomonic for SCAD) |
| Location | Any, often at bifurcations/plaques | Mid-to-distal segments, LAD most common |
| Other coronary disease | Usually atherosclerosis elsewhere | Typically clean (no atherosclerosis) elsewhere |
| Patient profile | Older, ASCVD risk factors | Young woman, peripartum, FMD, connective tissue disorder |
| Flow disturbance | TIMI flow impaired by intraluminal clot | TIMI flow impaired by external compression of lumen |
Part 4: When CAG is Insufficient - Role of OCT/IVUS
CAG alone is a luminogram - it shows only the contrast-filled lumen and cannot image vessel walls. When SCAD type 2/3 vs. thrombus is ambiguous, OCT is the preferred adjunct (resolution 10-20 μm vs. 100-200 μm for IVUS):
- OCT findings in SCAD: Intramural hematoma, intimal disruption, false lumen with compressed true lumen, no intraluminal thrombus
- OCT findings in recanalized thrombus: Multiple intraluminal channels (recanalization channels) with preserved vessel walls, no IMH
- OCT findings in atherosclerosis: Fibrocalcific plaque, lipid core, no IMH
Important caveat: OCT/IVUS in SCAD carries a risk of iatrogenic catheter-induced dissection (~3.4% in reported series) and should be reserved for diagnostic uncertainty. Intracoronary imaging should be used cautiously, with the wire staying in the true lumen.
Clinical Clues That Should Raise Suspicion for SCAD (vs. Thrombus)
- Young woman (<50 years) presenting with ACS
- Peripartum period (antepartum or first 12 weeks postpartum)
- No conventional cardiovascular risk factors
- Known fibromuscular dysplasia (FMD)
- Connective tissue disorder (Marfan, Ehlers-Danlos)
- Long smooth lesion without atherosclerosis elsewhere
- Recent intense physical or emotional stress
- Hormone therapy (OCP, beta-hCG injections)
- Coronary tortuosity on CAG (78% vs 17% in controls)
Sources:
- Fuster and Hurst's The Heart, 15th Edition (Saw J classification; SCAD diagnosis chapter, p.648)
- Goldman-Cecil Medicine (CAG findings in NSTEACS, thrombus appearance, p.2709)
- OCT differentiating SCAD from recanalized thrombus (PMC, 2025) - PMID:38089767
- Recent reviews: García-Guimarães et al., Expert Rev Cardiovasc Ther 2024 (angiographic patterns in SCAD)
This is a shared conversation. Sign in to Orris to start your own chat.