
Explain in detail
Document Header
Patient Identification
- Patient's Name: Amina Bibi
- Address: Not filled in
- Mode of Admission: OPD/Casualty/Clinic (not specified which)
- Date of Admission: Not filled in
Clinical Narrative (Main Body)
Patient Summary
"36 yrs old pt. K/C of CLL - on treatment from Oncologist and RA"
- 36 years old patient - a relatively young adult
- K/C = Known Case (a standard abbreviation meaning the patient has an already-established diagnosis)
- CLL = Chronic Lymphocytic Leukemia - a type of blood cancer (B-cell malignancy) in which abnormal lymphocytes accumulate in the blood, bone marrow, and lymph nodes. It is the most common adult leukemia. At 36, this is unusually young (CLL typically affects those >60 years).
- On treatment from Oncologist - she is already under active cancer care
- RA = Rheumatoid Arthritis - a chronic autoimmune inflammatory joint disease. Having both CLL and RA means this patient is doubly immunocompromised - both from the malignancy itself and potentially from the immunosuppressive drugs used to treat RA (steroids, methotrexate, biologics).
"Bed ridden for 8 years"
- The patient has been confined to bed for 8 years, indicating severe functional disability - likely from advanced RA causing joint destruction, or from the combination of both diseases.
Presenting Complaints (C/O = Complaints of)
"This time presented to us c̄ C/O..."
-
Cough with sputum - 1 month
- Productive cough lasting one month suggests a lower respiratory tract infection (LRTI), possibly pneumonia or bronchitis
- In an immunocompromised patient with CLL, this raises concern for opportunistic infections (bacterial pneumonia, fungal, or even Pneumocystis jirovecii pneumonia/PJP)
-
Fever with chills
- Systemic signs of infection - fever + rigors/chills suggest sepsis or bacteremia in this immunocompromised host
-
Oral thrush and vomiting - 20 days
- Oral thrush = oropharyngeal candidiasis - white plaques on the oral mucosa caused by Candida albicans
- In an immunocompromised patient, this is a classic opportunistic infection, directly reflecting T-cell or overall immune failure
- Vomiting accompanying thrush suggests it may have extended into esophageal candidiasis (causing dysphagia/odynophagia and nausea/vomiting)
-
Constipation - 3 days
- Recent onset constipation, likely related to reduced oral intake, dehydration from vomiting, or medication effects
Abbreviated Complaints List
"A/C: vomiting, cough"
Examination Findings
Vitals (Left Column)
- BP - Blood pressure (value not written)
- Pulse - Heart rate (value not written)
- Temp - Temperature (value not written)
- SpO2 - Oxygen saturation (value not written)
S/E (Systemic Examination)
S1 + S2 + 0
- S1 and S2 = normal heart sounds (lub-dub) present
- +0 = no added sounds (no murmurs, gallops, or rubs)
- Cardiovascular system is essentially normal on auscultation
15/15 GCS
- GCS = Glasgow Coma Scale - a neurological scoring system (3-15)
- 15/15 = fully alert and oriented, no neurological impairment
Pain epigastrium
- Epigastric pain = tenderness/pain in the upper-middle abdomen (stomach area)
- This is consistent with nausea/vomiting, possibly from esophageal candidiasis extending into the stomach, or from gastritis
Congested chest, crepts
- Congested chest = dull/reduced breath sounds, indicating fluid or consolidation
- Crepts = Crepitations (Crackles) - abnormal lung sounds heard on auscultation, indicating fluid, consolidation, or fibrosis in the lung parenchyma
- Together, these findings are consistent with pneumonia or lower respiratory tract infection (LRTI), which aligns with her 1-month history of productive cough
Management Plan (Right Column)
Plan:
-
O2 Support - Supplemental oxygen, likely due to low SpO2 from pneumonia
-
I/O Record - Intake/Output chart - to monitor fluid balance (important given vomiting and risk of dehydration)
-
NG + Catheter - Nasogastric tube (for feeding/medication delivery, given vomiting) + urinary catheter (for accurate urine output monitoring - essential in potentially septic, bedridden patient)
-
Temp record - Temperature monitoring chart (to track fever trend)
-
BLTIA - Likely Blood, Liver, TFTs, Investigations, ABG or a standard abbreviation for a blood workup panel used locally
-
Blood + Urine C/S - Culture and Sensitivity of blood and urine - to identify the infecting organism and determine which antibiotics it is sensitive to (critical in an immunocompromised septic patient)
-
Urine R/E - Urine Routine Examination - dipstick/microscopy to look for infection, blood, protein in urine
-
2 O RCC - 2 units of Red Cell Concentrate (Packed Red Blood Cells) - the patient likely has significant anemia (common in CLL due to bone marrow infiltration and hemolytic anemia), requiring a blood transfusion
Clinical Summary and Significance
| Problem | Significance |
|---|---|
| CLL | Causes hypogammaglobulinemia and impaired B-cell immunity - high infection risk |
| RA (on immunosuppressants) | Further suppresses immunity |
| Bedridden x 8 years | Increased risk of aspiration, pressure sores, DVT, muscle wasting |
| Oral thrush + vomiting | Likely esophageal candidiasis from severe immunosuppression |
| Productive cough + crepts + fever | Probable pneumonia - could be bacterial, fungal (Aspergillus), or PJP |
| Epigastric pain | Possible esophageal/gastric involvement of candida |
| Anemia (2 units RCC ordered) | Expected in CLL - bone marrow infiltration |
- Antifungal therapy (IV fluconazole or amphotericin B for systemic candidiasis)
- Antibiotics (broad-spectrum for pneumonia/sepsis)
- Blood transfusion
- Nutritional support via NG tube
- Close monitoring in a high-dependency or ICU setting

Explain it.
Document Overview
- A TMO Summary (top section, written in pencil/light pen)
- A Formal Referral Letter from Surgical Ward to Medicine/Cardiology (written over it in blue ink, with a structured patient condition box)
PART 1 - TMO Summary (Top Section, Light Handwriting)
"A 50 year old male patient, he is a case of FAI having two bullet wound one at the sternum (entry) having exit wound at scapula region and second bullet in the face which bled to medicule (medulla?) - currently he is vitally stable having GCS: 15/15"
Breaking this down:
| Bullet | Entry | Exit | Notes |
|---|---|---|---|
| 1st | Sternum (breastbone, front of chest) | Scapula region (shoulder blade, back) | A through-and-through chest wound - extremely dangerous, traversing the thoracic cavity |
| 2nd | Face | Unclear/retained | "Which bled to medulla" - possibly penetrating into the brainstem region or causing massive hemorrhage |
- The bullet traveled through the entire chest cavity
- At risk of injuring: heart, great vessels (aorta, pulmonary vessels), lungs, esophagus, trachea
- This is why a left thoracotomy (chest opening surgery) was performed (mentioned in the referral below)
- Vitally stable - hemodynamically holding at the time of writing
- GCS 15/15 - fully conscious and neurologically intact (Eye 4 + Verbal 5 + Motor 6), which is reassuring given a face/head bullet wound
PART 2 - Referral Letter (Blue Ink, Formal Section)
"Respected colleague, we have this 50 yrs old male patient named Shakis presented to us as a case of firearm injury. Left Thoracotomy done. The patient BP was 200/100 and after giving IV Lasix (40mg?) it is still 220/120. Kindly assess and help in further management."
Breaking this down:
- A thoracotomy is a surgical incision into the chest wall to access the thoracic cavity
- A left thoracotomy is performed to access the left lung, heart, descending aorta, or to control bleeding from left-sided chest trauma
- This confirms the patient underwent emergency chest surgery for the gunshot wound
- BP = 200/100 mmHg on arrival (Stage 2 severe hypertension / hypertensive urgency)
- Given IV Lasix (Furosemide) - a loop diuretic used to reduce fluid overload and lower BP
- Despite Lasix, BP remains 220/120 mmHg - this is now a hypertensive emergency, unresponsive to initial therapy
- This is why cardiology/medicine was urgently called - the surgical team cannot manage refractory hypertension alone; IV antihypertensives like labetalol, hydralazine, or nitroprusside are needed
PART 3 - Patient Condition Box (Structured Vitals)
| Parameter | Finding | Significance |
|---|---|---|
| Pulse | Partially legible | Heart rate monitoring |
| BP | Left side marker | Measuring BP on left arm (right may be unreliable post-chest trauma) |
| Temp | mute/m? (febrile?) | Temperature |
| RR | Abnormal (tachypneic?) | Respiratory rate - important post-thoracotomy |
| Urine Output | "Nab/5 lboul (low?)" | Reduced urine output - concerning for renal hypoperfusion or post-Lasix diuresis |
| NG | Blank | Nasogastric tube (for feeding/decompression) |
| Drain | Blank | Chest drain likely in situ post-thoracotomy |
| Conscious Level | Thank you | Alert |
| Any Other | - | - |
Bottom Note
"Relieve the pain and treat the underlying cause"
- A clinical instruction to manage pain (likely significant post-thoracotomy and from bullet wounds) and address the root cause of the hypertensive crisis (could be pain-induced sympathetic surge, pre-existing hypertension, or a catecholamine response to trauma)
Full Clinical Picture Summary
| Element | Detail |
|---|---|
| Patient | 50M, named Shakis |
| Mechanism | Gunshot injury (firearm) - 2 bullets |
| Wounds | Chest (sternum in, scapula out) + face |
| Surgery done | Left thoracotomy (emergency chest surgery) |
| Key problem | Refractory hypertensive emergency - BP 220/120 despite IV Lasix |
| Neurology | GCS 15/15 - fully alert |
| Referral to | Medicine + Cardiology for BP management |
| Urgency | HIGH - uncontrolled hypertension post-trauma and post-surgery is life-threatening |
What are the position of appendix/ appendix clinical presentation
Positions of the Appendix
Anatomical Basis of Position Variation
The Six Positions (After Sir C. Wakeley)
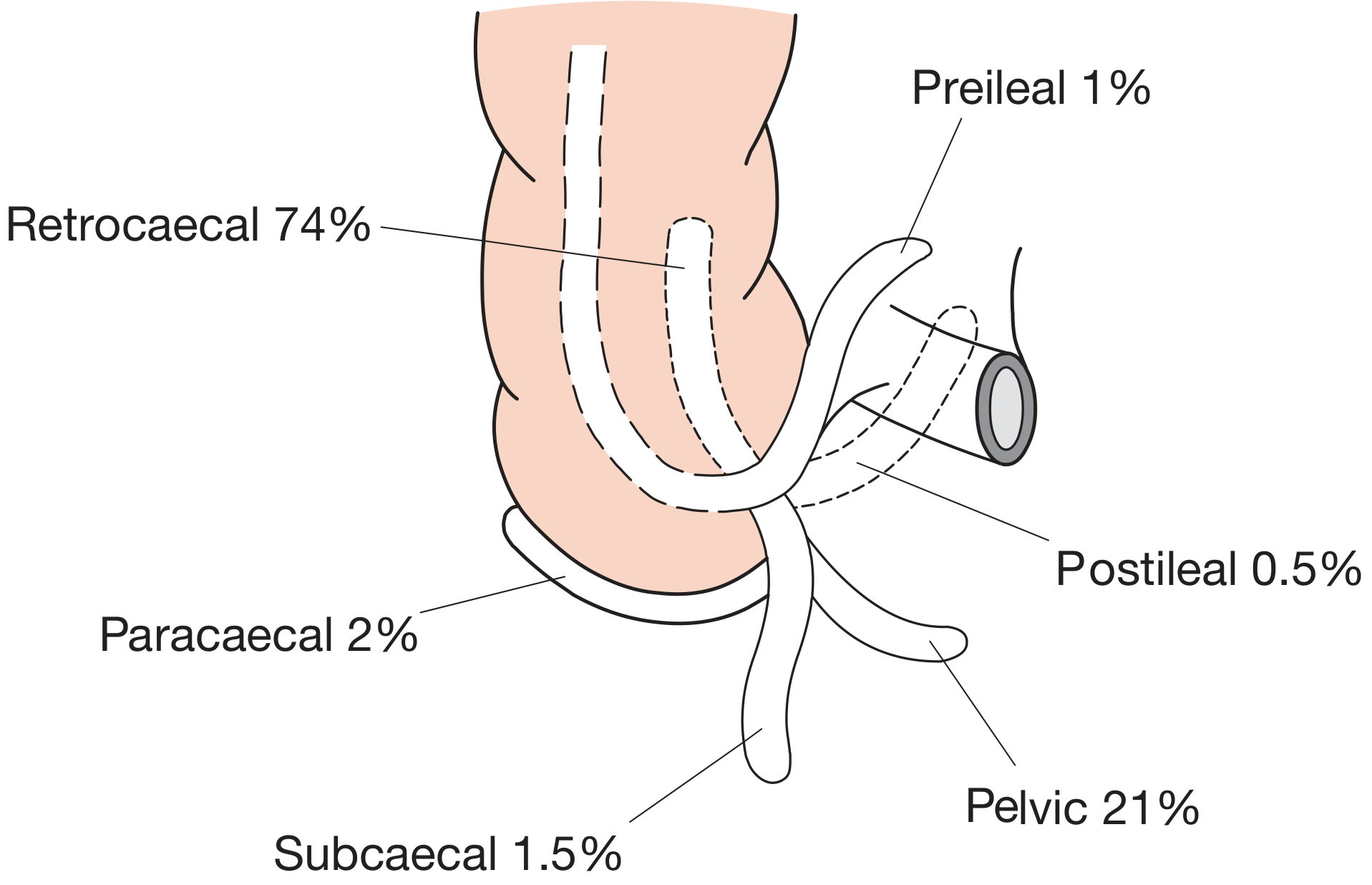
| Position | Frequency | Description |
|---|---|---|
| Retrocaecal | 74% | Behind the caecum; most common by far |
| Pelvic | 21% | Hangs down into the pelvis; second most common |
| Paracaecal | 2% | Alongside the caecum |
| Subcaecal | 1.5% | Below the caecum |
| Preileal | 1% | In front of the terminal ileum |
| Postileal | 0.5% | Behind the terminal ileum; rarest |
In rare cases of intestinal malrotation, the entire caecum fails to migrate to the right lower quadrant and the appendix may be found near the gallbladder or even in the left iliac fossa - causing profound diagnostic difficulty.
Clinical Presentation of Appendicitis
Symptoms (History)
Stage 1 - Visceral Pain (Early)
- Poorly localised, colicky periumbilical pain - this is midgut visceral discomfort from appendiceal obstruction/inflammation
- Pain starts central/periumbilical, similar to small bowel colic but less intense
- Associated with anorexia (constant and very useful sign - especially in children), nausea, and 1-2 episodes of vomiting that follow (not precede) the onset of pain
Stage 2 - Somatic Pain (Progression)
- As parietal peritoneum in the right iliac fossa (RIF) becomes irritated, pain shifts to the RIF and becomes constant, more intense, and localised
- Coughing or sudden movement worsens RIF pain
- This classic visceral-somatic sequence is present in only ~50% of patients
Signs (Examination)
General
- Low-grade pyrexia (37.2-37.7°C) - usually after the first 6 hours
- Mild tachycardia (80-90 bpm)
- In 20% of early cases, NO pyrexia or tachycardia
- Temperature >38.5°C in children suggests another diagnosis (e.g. mesenteric adenitis)
Abdominal Signs
| Sign | Description | Significance |
|---|---|---|
| McBurney's Point tenderness | Maximum tenderness 2/3 of the way from umbilicus to right anterior superior iliac spine | Classic point of appendix base |
| Muscle guarding | Involuntary rigidity of right iliac fossa muscles | Peritoneal irritation |
| Rebound tenderness | Pain on sudden release of deep pressure | Parietal peritoneum involvement |
| Rovsing's sign | Deep palpation of LEFT iliac fossa causes pain in the RIGHT iliac fossa | Peritoneal irritation referred to RIF |
| Psoas sign | Patient lies with right hip flexed for relief; hip extension causes pain | Appendix lying on psoas muscle (common in retrocaecal position) |
| Obturator sign | Pain on flexion + internal rotation of right hip | Inflamed appendix in contact with obturator internus (pelvic position) |
| Pointing sign | Patient points to where pain began vs where it moved | Helps trace visceral-somatic shift |
How Position Alters Clinical Presentation
| Position | Atypical Feature |
|---|---|
| Retrocaecal | Pain is in the flank/back (not anterior RIF); psoas sign positive; tenderness may be in the loin; can mimic renal colic |
| Pelvic | Suprapubic pain and tenesmus (urge to defecate); NO anterior abdominal wall tenderness; tenderness only on rectal examination; can mimic PID, ovarian pathology, or bladder problems |
| Preileal/Postileal | Pain and tenderness near the umbilicus; can mimic Meckel's diverticulitis or small bowel obstruction |
| Left iliac fossa (malrotation) | Pain in the LEFT iliac fossa - easily mistaken for diverticulitis or left-sided pathology |
| Subcaecal | Tenderness lower than McBurney's point; can mimic bladder or pelvic pathology |
Special Populations - Atypical Presentations
- Infants (<36 months): Cannot give history; diagnosis delayed; perforation rate is very high
- Elderly: Localisation to RIF is unusual; may present late with abdominal distension, vomiting, and generalised tenderness from developed peritonitis
- Pregnant women: Uterus displaces the appendix upward and laterally, shifting pain away from RIF
- Immunosuppressed/Diabetics: Signs may be blunted or absent - high perforation risk
Risk Factors for Perforation
- Extremes of age (very young or old)
- Immunosuppression
- Diabetes mellitus
- Faecolith obstructing the lumen
- Pelvic appendix position (delayed diagnosis due to absence of anterior wall signs)
- Previous abdominal surgery (limits omentum's ability to wall off infection)
Bottom Line
- Bailey & Love's Short Practice of Surgery, 28th Edition, Chapter 76
With full details but in simple terms, also i can't understand the appendix position
The Appendix - Everything Explained Simply
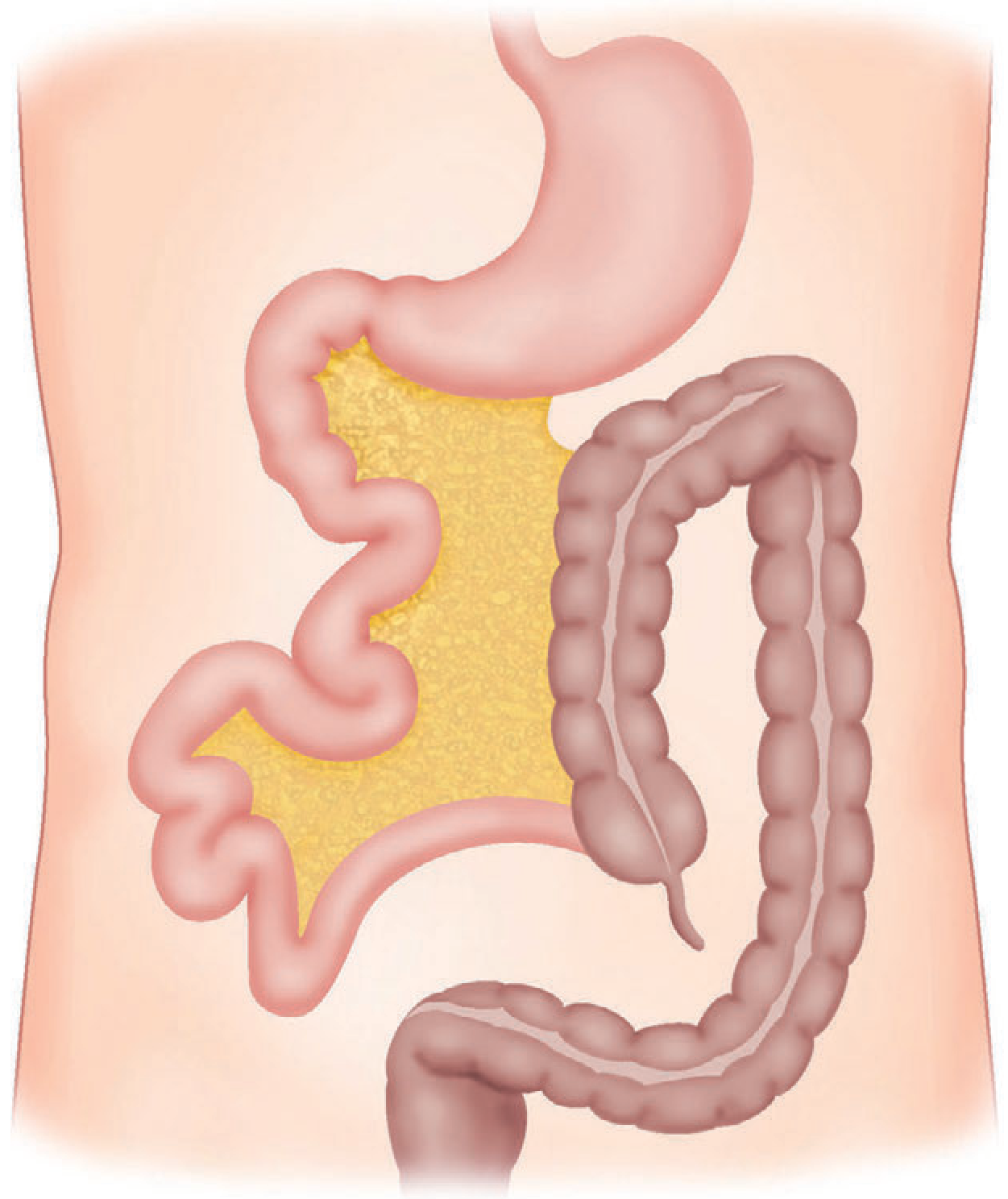
First - What IS the Appendix?
- The root (where it attaches to the caecum) is ALWAYS in the same place - lower right abdomen
- The tip (free end) can point in different directions in different people - this is what changes
PART 1 - POSITIONS OF THE APPENDIX
1. RETROCAECAL - 74% (Most Common - 3 out of 4 people!)
[CAECUM - the bag]
|
| <-- Appendix is hiding HERE, behind the caecum, pointing up
|
ROOT (always fixed here)
- Because it is hiding behind the intestine, pressing on the front of the belly may NOT cause much pain
- Pain may be felt in the right flank (side) or even the back - like a backache
- Can be confused with kidney stone because it is so far back
- Psoas sign is positive - the appendix lies on the psoas muscle (the big hip-flexor muscle), so the patient bends their right hip inward for relief, and straightening the hip causes pain
2. PELVIC - 21% (Second Most Common - 1 in 5 people)
ROOT (fixed here, right lower belly)
|
|
↓
[TIP hangs down into PELVIS]
(Near bladder, uterus/ovaries, rectum)
- Because it is deep in the pelvis, pressing on the front belly wall causes little or no pain - very deceptive!
- Instead the patient gets:
- Suprapubic pain (pain just above the pubic bone)
- Tenesmus (feeling of wanting to pass stool urgently)
- Diarrhoea (because tip irritates the rectum)
- Strangury (painful urination, because tip irritates the bladder)
- Tenderness is only found on rectal examination (finger in rectum) - this is why doctors must always do a rectal exam in lower abdominal pain
- In women it is easily confused with ovarian cyst, PID (pelvic infection)
- Obturator sign is positive - flex the right hip and rotate it inward, causing pain because the inflamed tip touches the obturator muscle inside the pelvis
3. PARACAECAL - 2%
4. SUBCAECAL - 1.5%
5. PREILEAL - 1%
6. POSTILEAL - 0.5% (Rarest)
Quick Visual Summary of ALL Positions
PREILEAL (1%)
[in front of small intestine]
↑
|
RETROCAECAL ← [CAECUM] → PARACAECAL (2%)
(74%) (ROOT)
|
SUBCAECAL (1.5%)
|
↓
PELVIC (21%)
[deep in pelvis]
POSTILEAL (0.5%) = behind the small intestine (to the side)
SPECIAL RARE CASE - Malrotation (No fixed position!)
PART 2 - CLINICAL PRESENTATION OF APPENDICITIS
Step-by-Step Story of What Happens in the Body
The Cause - Why Does Appendicitis Start?
- A hard lump of faeces (faecolith - like a stone made of poo)
- Swollen lymph nodes (after a viral infection)
- A worm (roundworm or pinworm in some regions)
- A tumour (in elderly people)
- Mucus keeps building up inside - pressure increases
- Bacteria multiply rapidly
- Blood supply gets cut off - the wall starts dying (gangrene)
- Eventually the appendix bursts (perforates) - spillling infected material into the belly - this is the dangerous stage
The Classic Symptom Sequence - "Murphy's Triad"
1st - PAIN (comes first)
- Pain starts around the belly button (umbilicus) or upper central abdomen
- It is a dull, crampy, colicky pain - not very severe
- This happens because the appendix develops from the "midgut" during fetal life, so early pain is always felt in the center of the belly, regardless of where the appendix actually is
- This is very important - even if the appendix is in the pelvis or behind the caecum, the FIRST pain is ALWAYS central
- The pain moves (shifts) to the right iliac fossa (right lower abdomen - roughly where you put your right hand in your pocket)
- Now the pain is constant, sharp, localised - the lining of the abdomen (peritoneum) is getting irritated
- Any movement, coughing, or bumping makes it worse
- The patient walks bent forward, guarding the right side
Key teaching point: The shift of pain from umbilicus to right lower abdomen = classic sign of appendicitis (present in ~50% of patients)
2nd - VOMITING (comes after pain)
- Always comes AFTER the pain starts - this is important!
- If vomiting comes before pain, think of another diagnosis (like gastroenteritis)
- Usually 1-2 episodes only, not severe
- Associated with nausea and total loss of appetite (anorexia) - the patient refuses food even if offered their favourite meal
3rd - FEVER (temperature rises)
- Low-grade fever: 37.2 - 37.7°C typically
- Pulse rate rises slightly (80-90 per minute)
- In the first 6 hours, fever may be ABSENT
- Very high temperature (above 38.5°C) in children suggests it is NOT appendicitis - more likely viral adenitis
Signs Doctors Look For
On Examination:
| Sign | How to Elicit | What it Means |
|---|---|---|
| McBurney's Point Tenderness | Press 2/3 of the way from belly button to right hip bone - maximum pain here | Appendix root is inflamed |
| Muscle Guarding | Belly muscles of right lower abdomen become rigid/hard involuntarily | Body protecting inflamed area |
| Rebound Tenderness | Press deeply then suddenly release - pain increases on release | Peritoneum (belly lining) is irritated |
| Rovsing's Sign | Press on the LEFT lower abdomen - patient feels pain on the RIGHT | Referred peritoneal irritation to RIF |
| Psoas Sign | Extend/straighten right hip - causes pain | Appendix lying on psoas muscle (retrocaecal) |
| Obturator Sign | Flex right hip + rotate inward - causes pain | Appendix touching obturator muscle (pelvic) |
| Sherren's Triangle Hyperaesthesia | Skin over right lower abdomen becomes extra sensitive to touch | Early peritoneal sign |
How the POSITION Changes the Presentation
| Position | Where Patient Feels Pain | Confusion With | Special Sign |
|---|---|---|---|
| Retrocaecal (74%) | Right flank / back / loin | Kidney stone, renal colic | Psoas sign positive |
| Pelvic (21%) | Suprapubic / lower pelvis | Bladder infection, PID, ovarian cyst | Obturator sign positive; rectal tenderness |
| Paracaecal (2%) | Right iliac fossa (typical) | Normal appendicitis | Classic signs |
| Subcaecal (1.5%) | Low right abdomen | Bladder pathology | Below McBurney's point |
| Preileal (1%) | Near umbilicus | Meckel's diverticulum | Periumbilical tenderness |
| Postileal (0.5%) | Near umbilicus/central | Small bowel pathology | Most atypical |
| Malrotation (rare) | LEFT iliac fossa | Left-sided pathology (diverticulitis) | Completely wrong side! |
Special Groups - How Presentation Differs
Children
- Higher fever, more vomiting, often diarrhoea
- Cannot communicate pain well - examine using child's own hand
- Short omentum cannot wall off infection easily
- Perforation happens early - diagnose and operate fast
Elderly
- Weak abdominal muscles - very little guarding or rigidity
- Atherosclerosis of the appendix artery - gangrene happens faster
- Presents looking like intestinal obstruction (distension, vomiting, constipation)
- High risk of perforation
Pregnant Women
- Growing uterus pushes the appendix upward
- Pain may be felt in the right upper abdomen, not lower - confuses with gallbladder problems
- Must always think of appendicitis in any pregnant woman with right-sided pain
What Happens If NOT Treated?
- Appendicular Lump - omentum and bowel loops wrap around the appendix, forming a protective mass in the right iliac fossa (palpable tender mass, appears 2-3 days in)
- Appendicular Abscess - the lump becomes full of pus
- Perforation - appendix bursts; patient briefly feels better (pain disappears as pressure releases) but then rapidly deteriorates
- Peritonitis - infection spreads throughout the entire belly - board-like rigidity, silent abdomen (no bowel sounds), rising pulse, falling blood pressure - this is life-threatening
The Golden Rule
"The initial pain is ALWAYS central (umbilical), because the appendix develops from the midgut. The SECOND pain shifts to wherever the appendix TIP is lying."
I want to understand ECG completely.
I want to understand ECG completely.
I want to understand ECG completely. So give me all basic and advance ecg knowledge with full detail it mbbs level, also explain with ecg paper with diagram then goes for abnormally and change in ecg patten with that abnormalities, then goes as for all condition from simpler to complex one with diagram.
I want to understand ECG completely. So give me all basic and advance ecg knowledge with full detail it mbbs level, also explain with ecg paper with diagram then goes for abnormally and change in ecg patten with that abnormalities, then goes as for all condition from simpler to complex one with diagram. Use otentic source and explain such a why that i become the expert of ecg interpretation.