Teach me heart anatomy from basics to clinical
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
I now have excellent material from Gray's Anatomy for Students, Goldman-Cecil Medicine, and the Textbook of Clinical Echocardiography. Let me compile the comprehensive answer.
Heart Anatomy: From Basics to Clinical
1. The Big Picture - What the Heart Is and Does
The heart is a hollow muscular pump located in the mediastinum, sitting obliquely between the lungs. It has two separate but connected pumps working in parallel:
- Right pump - receives deoxygenated blood from the body and sends it to the lungs (pulmonary circulation)
- Left pump - receives oxygenated blood from the lungs and sends it to the body (systemic circulation)
Each pump consists of an atrium (thin-walled receiver) and a ventricle (thick-walled pumper), separated by a valve.
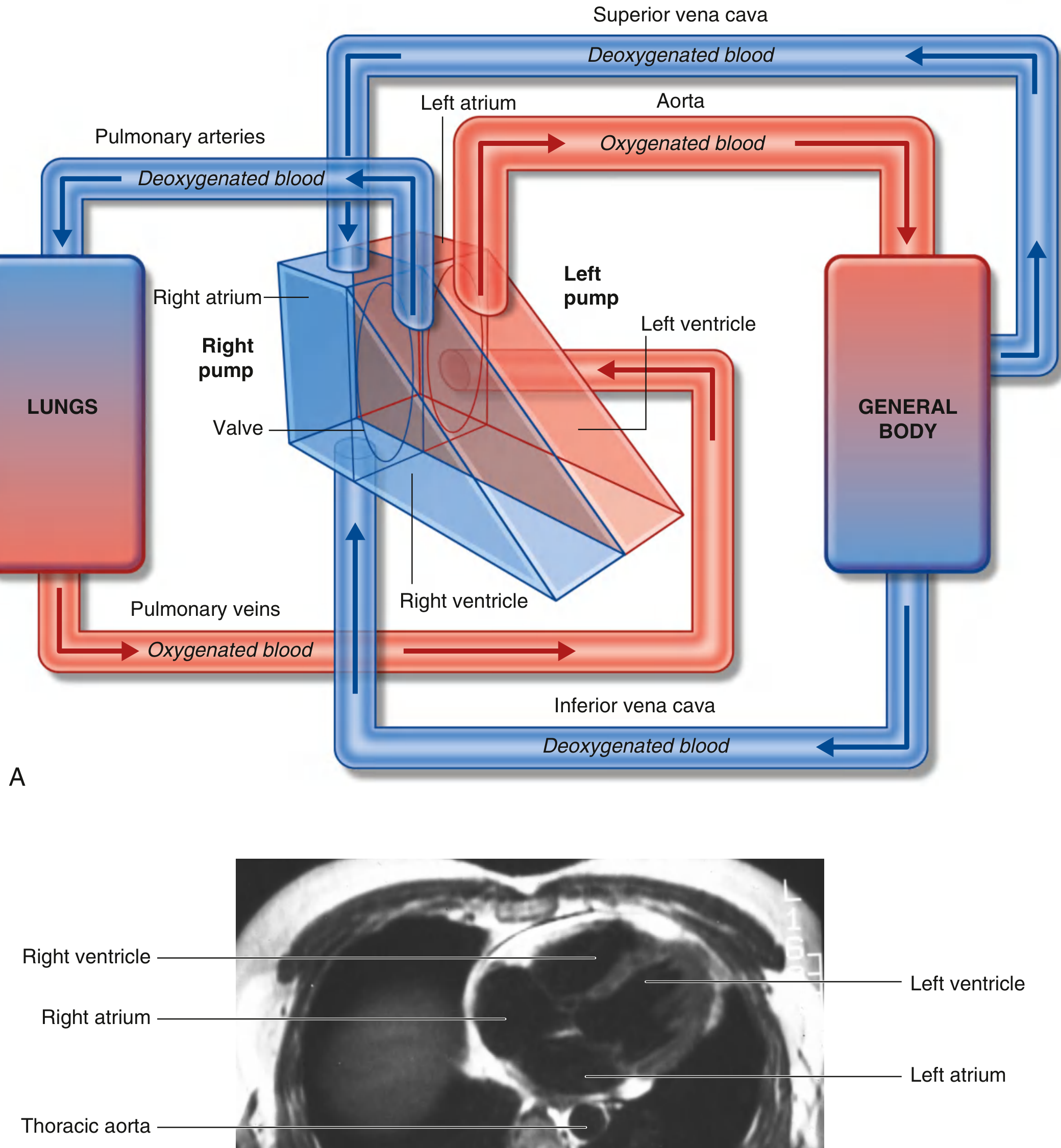
The right pump drives the pulmonary circuit (blue, deoxygenated); the left pump drives the systemic circuit (red, oxygenated). The MRI cross-section shows all four chambers and the thoracic aorta. - Gray's Anatomy for Students
Despite being a muscular pump, 60-70% of cardiac cells are fibroblasts, not cardiomyocytes. These fibroblasts produce collagen forming the extracellular matrix scaffold. In pathological states (hypertension, MI, heart failure), they generate excess matrix, causing fibrosis that impairs function. - Goldman-Cecil Medicine
2. Surface Anatomy and Borders
The heart has four surfaces:
- Anterior (sternocostal): mainly right ventricle
- Diaphragmatic (inferior): left ventricle and part of right ventricle
- Left (pulmonary): left ventricle, forming the cardiac apex
- Posterior (base): mainly left atrium
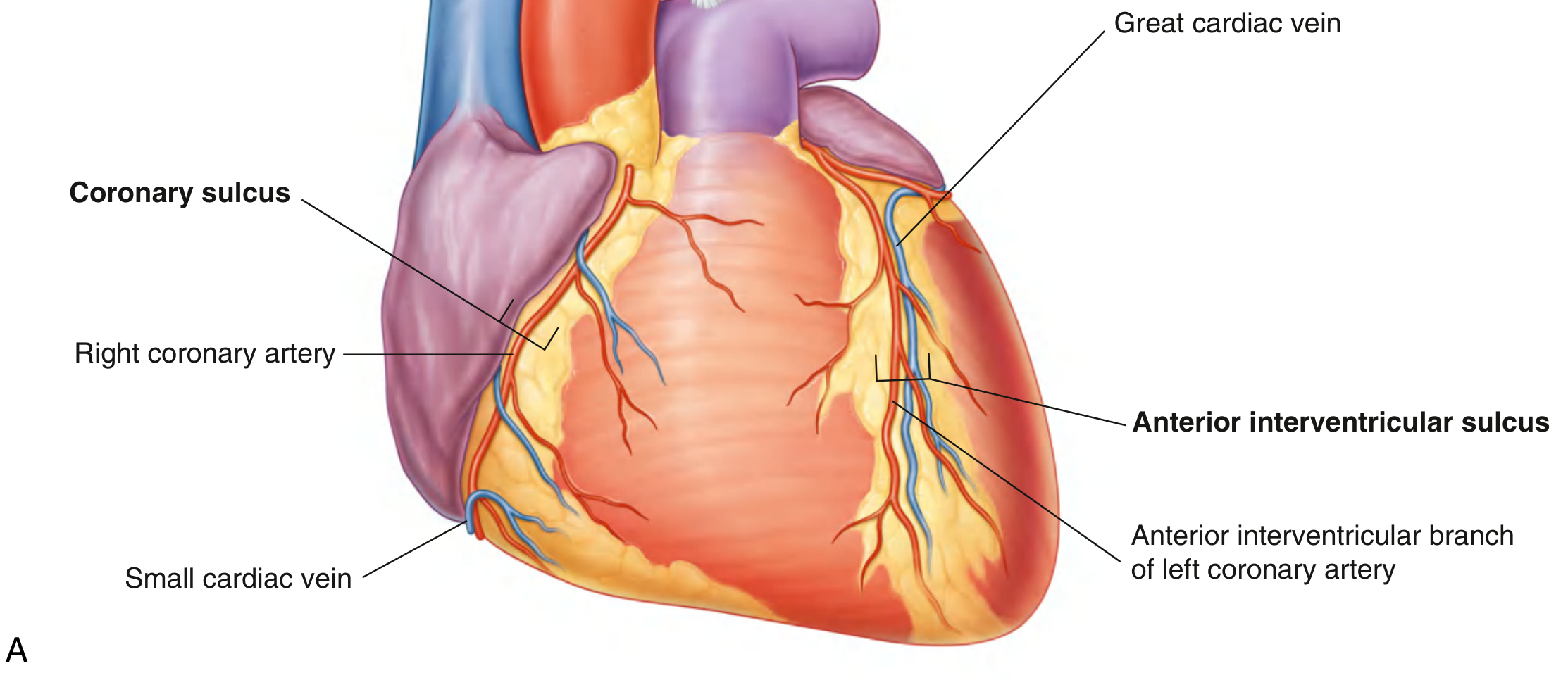
External Landmarks - the Sulci
The sulci are grooves on the surface that mark internal divisions:
| Sulcus | Location | Contains |
|---|---|---|
| Coronary (atrioventricular) sulcus | Encircles heart between atria and ventricles | Right coronary artery, coronary sinus |
| Anterior interventricular | Anterior surface | LAD artery + great cardiac vein |
| Posterior interventricular | Diaphragmatic surface | Posterior interventricular artery + middle cardiac vein |
3. The Four Chambers
Right Atrium
The right atrium forms the right border of the heart and receives blood from three vessels:
- Superior vena cava (SVC)
- Inferior vena cava (IVC)
- Coronary sinus (returns blood from the heart wall itself)
Key internal features:
- Crista terminalis - vertical muscular ridge separating smooth (sinus venosus-derived) from trabeculated (pectinate muscle-bearing) parts
- Fossa ovalis - depression in the interatrial septum; the remnant of the foramen ovale (fetal structure)
- Tricuspid valve orifice - leads to the right ventricle
Clinical note: The SA node sits at the superior end of the crista terminalis, at the SVC-right atrium junction.
Right Ventricle
The right ventricle pumps blood into the pulmonary trunk. Because pulmonary resistance is much lower than systemic resistance, its wall is significantly thinner than the left ventricle.
Internal features:
- Trabeculae carneae - muscular ridges lining the walls
- Papillary muscles (anterior, posterior, septal) - connected to the tricuspid valve leaflets by chordae tendineae
- Septomarginal trabecula (moderator band) - carries the right bundle branch of the conduction system
Left Atrium
Located posteriorly, the left atrium receives oxygenated blood from four pulmonary veins (two from each lung). It forms the posterior surface (base) of the heart. The left auricle projects anteriorly.
Clinical note: The left atrium is the most posterior chamber. It lies directly anterior to the esophagus - left atrial enlargement (from mitral stenosis) can compress the esophagus and cause dysphagia.
Left Ventricle
The left ventricle is the primary pumping chamber, with walls typically 3x thicker than the right ventricle (8-12 mm vs 3-4 mm) because it pumps against systemic vascular resistance.
Internal features:
- Bicuspid (mitral) valve - between left atrium and left ventricle; 2 leaflets (anterior and posterior), with papillary muscles (anterior and posterior groups) attached via chordae tendineae
- Aortic vestibule - smooth-walled outflow tract leading to the aortic valve
- Interventricular septum - shared with the right ventricle; has a thin membranous part superiorly and a thick muscular part inferiorly
4. The Cardiac Valves
The heart has four valves, organized into two types:
Atrioventricular (AV) Valves
Prevent backflow from ventricles into atria during systole.
| Valve | Location | Leaflets | Papillary Muscles |
|---|---|---|---|
| Tricuspid | Right AV orifice | 3 (anterior, posterior, septal) | 3 groups |
| Mitral (bicuspid) | Left AV orifice | 2 (anterior, posterior) | 2 groups |
The papillary muscles contract during systole, pulling the chordae tendineae taut - this keeps the valve leaflets from prolapsing back into the atria during the high-pressure ventricular contraction.
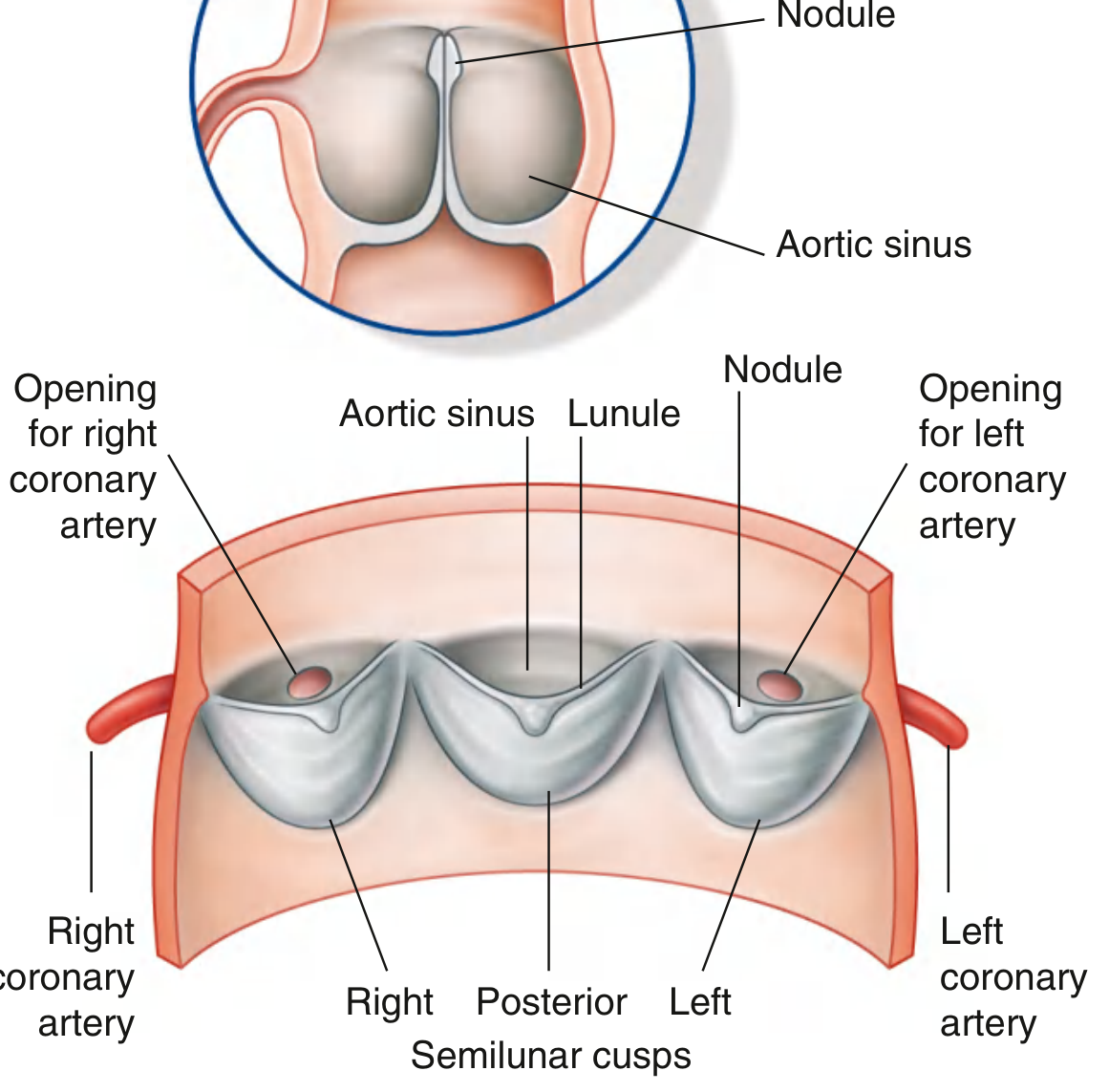
Semilunar Valves
Prevent backflow from arteries into ventricles during diastole.
| Valve | Location | Cusps |
|---|---|---|
| Pulmonary | Between RV and pulmonary trunk | 3 semilunar cusps |
| Aortic | Between LV and aorta | 3 semilunar cusps (right, left, posterior/non-coronary) |
The aortic valve has three pocket-like sinuses (sinuses of Valsalva) behind each cusp. The right and left coronary arteries originate from the right and left aortic sinuses respectively. As blood recoils after ventricular contraction, it fills these sinuses and is automatically forced into the coronary ostia.
Clinical note - Valve Disease:
- Aortic stenosis (most common valve disease): atherosclerotic calcification of leaflets; causes exertional syncope, angina, and dyspnea (SAD triad)
- Mitral stenosis: most common cause is rheumatic fever; presents decades after acute rheumatic endocarditis; leads to left atrial enlargement and pulmonary hypertension
- Mitral regurgitation: papillary muscle rupture post-MI is a catastrophic complication
- Tricuspid/pulmonary valve disease: most commonly from infection; IV drug use and alcoholism are major risk factors for tricuspid endocarditis - Gray's Anatomy for Students
5. The Cardiac Skeleton
The cardiac skeleton is a collection of dense fibrous connective tissue forming four rings in a plane between the atria and ventricles. It serves three major functions:
- Structural support - anchors the valve leaflets and provides attachment points for atrial and ventricular muscle
- Electrical insulation - electrically separates atrial from ventricular myocardium; the only normal conduction pathway through this fibrous barrier is the AV bundle (Bundle of His)
- Mechanical - prevents excessive dilation of the valve orifices during contraction
6. Coronary Blood Supply
The coronary arteries arise from the aortic sinuses directly above the aortic valve and travel through the epicardium to supply the myocardium.
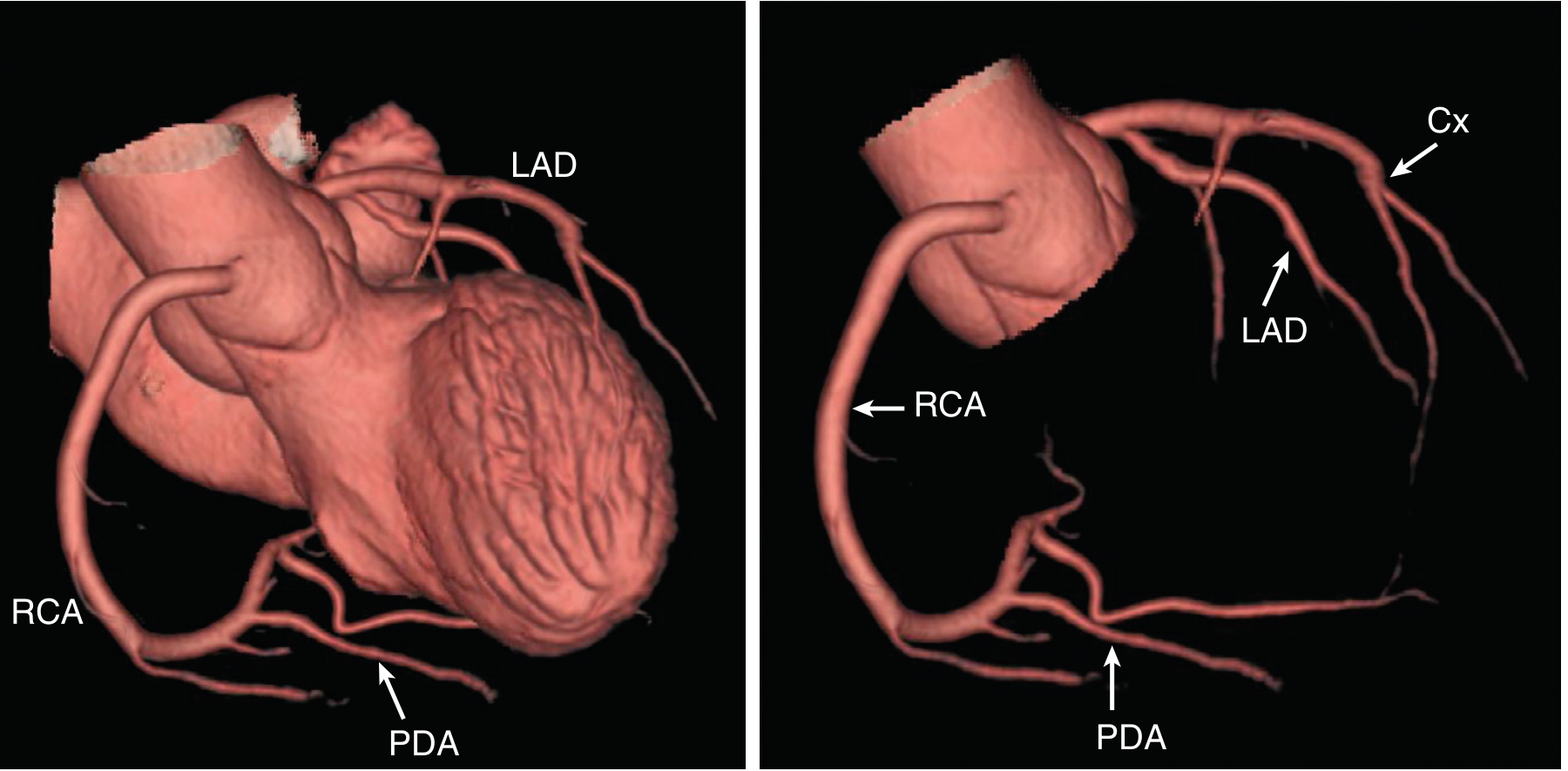
Left Coronary Artery (LCA)
Arises from the left coronary sinus of Valsalva and quickly divides into two main branches:
-
Left Anterior Descending (LAD) - runs down the anterior interventricular groove toward the apex
- Supplies: anterior interventricular septum (via septal perforators), anterior LV wall (via diagonal branches)
- "The widow maker" - proximal LAD occlusion causes a massive anterior MI
-
Circumflex (Cx) - continues laterally in the atrioventricular groove
- Supplies: lateral LV wall (via obtuse marginal branches)
- In ~20% of people (left-dominant), gives rise to the posterior descending artery (PDA)
Right Coronary Artery (RCA)
Arises from the right coronary sinus and follows the right atrioventricular groove.
- In ~80% of people (right-dominant circulation), gives rise to the posterior descending artery (PDA)
- The PDA supplies: inferior interventricular septum, inferior LV free wall
- RCA also supplies the SA node (in 60% of people) and AV node (in 80-90% of people)
Coronary Dominance
The term "dominance" refers to which artery gives rise to the PDA:
- Right dominant: 80% of people (RCA gives PDA)
- Left dominant: 20% of people (Circumflex gives PDA)
- Co-dominant: small percentage where both contribute
Clinical correlate - MI territories:
- LAD occlusion → anterior + anteroseptal STEMI (V1-V4)
- RCA occlusion → inferior STEMI (II, III, aVF) ± right ventricular MI ± AV block
- Circumflex occlusion → lateral/posterior MI (I, aVL, V5-V6; posterior leads V7-V9)
Coronary Flow Physiology
- Coronary arteries receive blood from the aorta during diastole (especially to the endocardium)
- During systole, intramyocardial pressure compresses subendocardial vessels; epicardial vessels still receive flow during systole
- Coronary flow can increase up to 6x (via nitric oxide, adenosine, bradykinins, prostaglandins, CO₂) to match increased metabolic demand - Goldman-Cecil Medicine
7. Cardiac Conduction System
The conduction system initiates and coordinates the cardiac cycle, ensuring atria contract before ventricles, and ventricles contract apex-first (squeezing blood toward the outflow tracts).
Components (in order of activation)
SA Node → Atrial muscle → AV Node → Bundle of His →
Left + Right Bundle Branches → Purkinje Fibers → Ventricular muscle
1. Sinoatrial (SA) Node - the pacemaker
- Location: superior end of the crista terminalis, at the SVC-right atrium junction
- Fires at 60-100 bpm intrinsically
- Supplied by the SA nodal artery (from RCA in 60%, LCx in 40%)
2. Atrioventricular (AV) Node
- Location: triangle of Koch - near the coronary sinus opening, close to the tricuspid valve's septal cusp attachment, within the atrioventricular septum
- Introduces a critical conduction delay (~0.1 s) allowing ventricular filling before contraction
- Supplied by the AV nodal artery (from RCA in 80-90%)
3. Bundle of His (AV bundle)
- Direct continuation of the AV node
- Passes along the lower border of the membranous interventricular septum
- The only electrical bridge through the fibrous cardiac skeleton
4. Bundle Branches
- Right bundle branch: travels down the right side of the septum, enters the septomarginal trabecula (moderator band) to reach the anterior papillary muscle, then fans out as Purkinje fibers
- Left bundle branch: passes to the left side of the muscular septum, descends to the LV apex; usually divides into anterior and posterior fascicles
5. Purkinje Fibers (subendocardial plexus)
- Spread throughout both ventricles
- Activate papillary muscles and apex first, then the base - this apical-to-basal contraction wrings blood upward into the outflow tracts
Clinical note - Conduction Disease:
- Coronary artery disease is the most common cause of conduction system disruption
- RCA occlusion (inferior MI) → AV node ischemia → 1st/2nd/3rd degree AV block
- LAD occlusion → bundle branch ischemia → LBBB or RBBB
- RBBB is often benign; new LBBB post-MI suggests extensive anterior infarction
8. The Pericardium
The heart is enclosed in the pericardium, which has two layers:
- Fibrous pericardium - tough outer layer anchoring the heart to surrounding structures
- Serous pericardium - double-layered membrane:
- Parietal layer (lines fibrous pericardium)
- Visceral layer (epicardium, adheres to the heart surface)
- Pericardial cavity between these two layers normally contains 15-50 mL of lubricating fluid
Clinical note - Pericardial disease:
- Cardiac tamponade: fluid accumulation in pericardial cavity compresses the heart, reducing filling. Presents with Beck's triad: hypotension, distended neck veins, muffled heart sounds. Pulsus paradoxus >10 mmHg is characteristic.
- Pericarditis: inflammation; presents as sharp, pleuritic, positional chest pain (worse supine, better leaning forward)
9. The Cardiac Walls (Histology)
The heart wall from outside to inside:
| Layer | Description |
|---|---|
| Epicardium | Visceral pericardium; contains fat, coronary vessels, nerves |
| Myocardium | Cardiac muscle (cardiomyocytes); the bulk of the wall |
| Endocardium | Inner lining of smooth endothelial cells; continuous with vessel intima |
Cardiomyocytes are:
- Branched, striated, uninucleate (mostly)
- Connected end-to-end by intercalated discs containing gap junctions (electrical coupling) and desmosomes (mechanical coupling)
- Gap junctions allow action potentials to spread rapidly - the myocardium functions as a functional syncytium
10. Congenital Defects - Clinical Anatomy Applied
These arise from defects in septal development:
| Defect | Anatomy | Shunt direction | Key consequence |
|---|---|---|---|
| ASD (atrial septal defect) | Failure of foramen ovale closure | Left → Right | RV volume overload; pulmonary HTN if chronic |
| VSD (ventricular septal defect) | Most common CHD; usually membranous septum | Left → Right | RV hypertrophy, pulmonary congestion |
| PDA | Patent ductus arteriosus | Left (aorta) → Right (pulmonary artery) | Pulmonary HTN; continuous "machinery" murmur |
| Tetralogy of Fallot | VSD + pulmonary stenosis + overriding aorta + RV hypertrophy | Right → Left (cyanotic) | Cyanosis, "tet spells"; boot-shaped heart on CXR |
Tetralogy of Fallot is the most common cyanotic congenital heart disorder diagnosed after birth. The right → left shunt means deoxygenated blood bypasses the lungs and enters the systemic circulation. - Gray's Anatomy for Students
Summary - The "Need to Know" Clinical Framework
| Structure | What it does | What goes wrong |
|---|---|---|
| LV wall (thick) | Systemic pump | Hypertrophy (HTN), dilates (DCM), scars (MI) |
| Mitral valve | LV inlet guard | Stenosis (rheumatic), regurgitation (MVP, papillary rupture) |
| Aortic valve | LV outlet guard | Stenosis (calcific), regurgitation (infective endocarditis) |
| LAD | Anterior LV blood supply | Occlusion = anterior STEMI |
| RCA | Inferior LV + conduction system | Occlusion = inferior STEMI + AV block |
| SA node | Pacemaker | Sick sinus syndrome |
| AV node | Conduction delay/gatekeeper | AV block; target of adenosine/verapamil for SVT |
| Interventricular septum | Separates pressures | VSD (congenital); rupture post-MI |
| Pericardium | Protective sac | Tamponade, pericarditis |
Sources: Gray's Anatomy for Students; Goldman-Cecil Medicine International Edition; Textbook of Clinical Echocardiography (Feigenbaum); Fuster and Hurst's The Heart, 15th Edition
This is a shared conversation. Sign in to Orris to start your own chat.