can u generate pyq question from neet pg and final year mbbs on topic SLE
Reading File
Finding Sources
Searching the Web
NEET PG previous year questions SLE systemic lupus erythematosus mcq
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
I now have comprehensive, authoritative data from multiple medical textbooks. Let me compile the PYQ-style questions.
Here are 30 high-yield PYQ-style MCQs on SLE (NEET PG & Final Year MBBS level), organized by topic, with answers and explanations sourced from Harrison's, Goldman-Cecil, Firestein & Kelley's Rheumatology, and Fitzpatrick's Dermatology.
SLE - Previous Year Pattern MCQs
NEET PG & Final MBBS | 30 Questions with Explanations
SECTION 1: EPIDEMIOLOGY & BASICS
Q1. SLE predominantly affects which group?
- A) Men aged 40-60 years
- B) Women of childbearing age
- C) Children under 10 years
- D) Elderly men
✅ Answer: B
Explanation: ~90% of SLE patients are women, most of childbearing age. The disease is 9 times more prevalent in women than men. Black women have the highest prevalence. (Harrison's 22E)
Q2. Which racial/ethnic group has the highest prevalence of SLE among women?
- A) Asian/Pacific Islander
- B) White women
- C) Hispanic women
- D) Black women
✅ Answer: D
Explanation: Black women have the highest prevalence of SLE, followed by Hispanic, White, and Asian/Pacific Islander women. (Harrison's 22E)
Q3. SLE is caused by which basic immunological mechanism?
- A) T-cell mediated cytotoxicity
- B) IgE mediated hypersensitivity
- C) Overactive innate and adaptive immunity causing tissue damage via autoantibodies and immune complexes
- D) NK cell dysfunction
✅ Answer: C
Explanation: SLE involves overactive innate and adaptive immune systems causing tissue damage through autoantibodies and immune complexes (Type III hypersensitivity predominantly). (Harrison's 22E)
SECTION 2: DIAGNOSIS & CLASSIFICATION CRITERIA
Q4. According to the 2019 EULAR/ACR classification criteria for SLE, which of the following is MANDATORY as an entry criterion?
- A) Anti-dsDNA positivity
- B) Malar rash
- C) ANA titer ≥ 1:80
- D) Proteinuria > 0.5 g/24h
✅ Answer: C
Explanation: ANA titer of ≥1:80 on Hep-2 cells is the mandatory entry criterion. If ANA is absent, the patient cannot be classified as SLE under EULAR/ACR 2019. (Goldman-Cecil; Rheumatology 2022)
Q5. As per 2019 EULAR/ACR criteria, what minimum total score is required to classify a patient as SLE (after positive ANA)?
- A) 6
- B) 8
- C) 10
- D) 12
✅ Answer: C
Explanation: A patient requires at least 10 points to meet the EULAR/ACR 2019 classification criteria, after the mandatory positive ANA. (Harrison's 22E; Goldman-Cecil)
Q6. Which single finding alone can give 10 points in the EULAR/ACR 2019 SLE criteria?
- A) Seizure
- B) Acute cutaneous lupus
- C) Renal biopsy showing Class III/IV lupus nephritis
- D) Anti-dsDNA positivity
✅ Answer: C
Explanation: No single clinical or laboratory value leads to 10 points EXCEPT renal biopsy revealing class III or IV lupus nephritis. (Harrison's 22E)
Q7. In the SLICC 2012 criteria for SLE, a positive diagnosis requires:
- A) 4 or more criteria (at least 1 clinical + 1 immunologic) OR biopsy-proven lupus nephritis with positive ANA or anti-dsDNA
- B) 6 or more clinical criteria only
- C) ANA + anti-dsDNA positivity
- D) 4 immunologic criteria
✅ Answer: A
Explanation: SLICC criteria: ≥4 items (at least 1 clinical and 1 immunologic) OR biopsy-proven lupus nephritis with positive ANA or anti-dsDNA. (Harriet Lane Handbook; Harrison's 22E)
Q8. The butterfly (malar) rash in SLE characteristically spares which area?
- A) Cheeks
- B) Bridge of nose
- C) Nasolabial folds
- D) Lower eyelids
✅ Answer: C
Explanation: The malar rash affects cheeks, bridge of nose, and lower eyelids but characteristically SPARES the nasolabial folds - a classic NEET PG favourite. (EduRev SLE test; Fitzpatrick's Dermatology)
Q9. What is the highest weightage finding in EULAR/ACR 2019 SLE scoring (points = 10)?
- A) Acute cutaneous lupus (6 points)
- B) Anti-dsDNA antibody (6 points)
- C) Joint involvement (6 points)
- D) Renal biopsy Class III/IV lupus nephritis (10 points)
✅ Answer: D
Explanation: Class III/IV lupus nephritis on biopsy = 10 points, the highest single scoring item. (Goldman-Cecil Table 245)
SECTION 3: AUTOANTIBODIES (Most Heavily Tested Topic)
Q10. Which antibody is the MOST SENSITIVE test for SLE?
- A) Anti-dsDNA
- B) Anti-Smith (Anti-Sm)
- C) Anti-histone
- D) ANA (Antinuclear antibody)
✅ Answer: D
Explanation: ANA is the most sensitive test for SLE (~95-99% sensitivity) but low specificity. (Symptom to Diagnosis: Evidence Based Guide 4E)
Q11. Which antibody is the MOST SPECIFIC test for SLE?
- A) ANA
- B) Anti-dsDNA
- C) Anti-Smith (Anti-Sm)
- D) Anti-histone
✅ Answer: C
Explanation: Anti-Smith (Anti-Sm) is the most specific antibody for SLE. Anti-dsDNA is also highly specific (~95%) and additionally correlates with disease activity (especially nephritis). (Miller's Review of Orthopaedics; Rheumatology 2022)
Q12. Anti-dsDNA antibodies are particularly associated with which complication of SLE?
- A) Cutaneous vasculitis
- B) Lupus nephritis
- C) Serositis
- D) Seizures
✅ Answer: B
Explanation: Anti-dsDNA antibodies are deposited in the kidney, skin, choroid plexus, and joints. They are specifically associated with lupus nephritis and serve as a marker of disease activity. (Firestein & Kelley's Rheumatology; Rheumatology 2022)
Q13. Anti-Ro (SS-A) antibodies in SLE are associated with which condition in neonates?
- A) Neonatal thrombocytopenia
- B) Neonatal lupus with congenital heart block
- C) Neonatal renal failure
- D) Neonatal seizures
✅ Answer: B
Explanation: Anti-Ro/SS-A antibodies cross the placenta and are associated with neonatal lupus, specifically congenital complete heart block. Anti-Ro is also seen in subacute cutaneous lupus erythematosus (SCLE). (EduRev; Fitzpatrick's Dermatology)
Q14. Anti-RNP (anti-U1 RNP) antibodies in high titers are most characteristic of:
- A) SLE only
- B) Sjögren's syndrome
- C) Mixed Connective Tissue Disease (MCTD)
- D) Drug-induced lupus
✅ Answer: C
Explanation: High titer anti-RNP (anti-U1 RNP) is the hallmark of Mixed Connective Tissue Disease (MCTD/Sharp syndrome). (Miller's Review of Orthopaedics)
Q15. Which antibody pattern is as follows: Anti-Sm → SLE, Anti-RNP → MCTD, Anti-Scl-70 → Scleroderma, Anti-histone → Drug-induced lupus. Which matches Anti-Ro/Anti-La?
- A) SLE and Lupus nephritis
- B) Drug-induced lupus
- C) Sjögren's syndrome (and neonatal lupus)
- D) Antiphospholipid syndrome
✅ Answer: C
Explanation: Anti-Ro (SS-A) and Anti-La (SS-B) are classically associated with Sjögren's syndrome and subacute cutaneous lupus/neonatal lupus. (Miller's Review of Orthopaedics)
SECTION 4: DRUG-INDUCED LUPUS
Q16. Which antibody is characteristically found in drug-induced lupus erythematosus (DILE)?
- A) Anti-dsDNA
- B) Anti-Smith
- C) Anti-histone
- D) Anti-Ro
✅ Answer: C
Explanation: Anti-histone antibodies are seen in up to 95% of drug-induced lupus cases. However, they are not specific as they are also found in 50-80% of idiopathic SLE. (Fitzpatrick's Dermatology; Harrison's 22E)
Q17. All of the following drugs are classic causes of drug-induced lupus EXCEPT:
- A) Procainamide
- B) Hydralazine
- C) Isoniazid
- D) Hydroxychloroquine
✅ Answer: D
Explanation: Classic drug-induced lupus causes: Procainamide, Hydralazine, Isoniazid, Methyldopa, Minocycline. Hydroxychloroquine is actually USED TO TREAT SLE. (Fitzpatrick's Dermatology)
Q18. A patient develops fever, joint pains, and a skin rash after starting a cardiac arrhythmia drug. Labs show antihistone antibodies. The drug most likely responsible is:
- A) Digoxin
- B) Amiodarone
- C) Procainamide
- D) Verapamil
✅ Answer: C
Explanation: Procainamide (cardiac antiarrhythmic) is the most notorious cause of drug-induced lupus. Most patients develop antihistone antibodies, but only 10-20% develop symptomatic disease. (Henry's Clinical Lab Methods)
Q19. Drug-induced lupus differs from idiopathic SLE in that:
- A) Renal involvement is more common
- B) Anti-dsDNA is always present
- C) Symptoms resolve after stopping the drug
- D) It primarily affects young women
✅ Answer: C
Explanation: Key distinguishing feature: DILE resolves after discontinuation of the offending drug. Renal and CNS involvement are rare in DILE unlike in idiopathic SLE. (Fitzpatrick's Dermatology; NEET PG pattern question)
SECTION 5: LUPUS NEPHRITIS
Q20. What is the WHO/ISN-RPS classification of lupus nephritis on biopsy with diffuse proliferative glomerulonephritis (most severe form)?
- A) Class II
- B) Class III
- C) Class IV
- D) Class V
✅ Answer: C
Explanation: Class IV = Diffuse proliferative lupus nephritis (most severe, worst prognosis). Class III = Focal proliferative. Class V = Membranous. Class II = Mesangial. (Goldman-Cecil; Harrison's 22E)
Q21. Laboratory findings in active lupus nephritis include all EXCEPT:
- A) Proteinuria
- B) RBC casts
- C) Hypocomplementemia (low C3, C4)
- D) Elevated CRP (markedly)
✅ Answer: D
Explanation: Active lupus nephritis shows proteinuria, dysmorphic RBCs, RBC casts, positive serology (ANA, anti-dsDNA), and hypocomplementemia. CRP is typically NOT markedly elevated in SLE flares (unlike in bacterial infections) - this is a classic NEET PG point. (Washington Manual; Goldman-Cecil)
Q22. Which finding on renal biopsy gives the highest score (10 points) in EULAR/ACR 2019 criteria?
- A) Class I
- B) Class II or V lupus nephritis (8 points)
- C) Class III or IV lupus nephritis (10 points)
- D) Mesangial proliferation
✅ Answer: C
Explanation: Renal biopsy Class III or IV = 10 points; Class II or V = 8 points in EULAR/ACR 2019. (Goldman-Cecil Table 245)
SECTION 6: CLINICAL FEATURES
Q23. Which organ system is MOST commonly affected in SLE?
- A) Pulmonary
- B) Cardiovascular
- C) Renal
- D) CNS
✅ Answer: C
Explanation: Cutaneous, musculoskeletal, and renal systems are most involved in SLE, followed by pulmonary, hematologic, cardiovascular, serosal, and CNS. (Harrison's 22E)
Q24. Libman-Sacks endocarditis in SLE is characterized by:
- A) Vegetations on the mitral valve on the ventricular surface
- B) Vegetations on BOTH surfaces of the valve leaflets (especially mitral)
- C) Large destructive vegetations like in infective endocarditis
- D) Tricuspid valve involvement only
✅ Answer: B
Explanation: Libman-Sacks endocarditis (non-bacterial thrombotic endocarditis) in SLE involves both surfaces of valve leaflets, most commonly the mitral valve. The vegetations are small and sterile. (High-yield NEET PG fact)
Q25. A child presents with fever, photosensitivity, and a facial rash that spares the nasolabial fold. What is the diagnosis?
- A) Rosacea
- B) Dermatomyositis
- C) Systemic Lupus Erythematosus
- D) Erysipelas
✅ Answer: C
Explanation: Classic presentation of SLE: fever + photosensitivity + malar rash sparing nasolabial folds. (Oncourse AI NEET PG; Fitzpatrick's Dermatology)
SECTION 7: TREATMENT
Q26. Drug of choice for SLE in pregnancy is:
- A) Methotrexate
- B) Mycophenolate mofetil
- C) Hydroxychloroquine
- D) Cyclophosphamide
✅ Answer: C
Explanation: Hydroxychloroquine is the drug of choice for SLE in pregnancy. Steroids are deactivated by placental enzymes. Methotrexate and MMF are teratogenic. (PrepLadder NEET PG; Rheumatology 2022)
Q27. Hydroxychloroquine in SLE is useful for all EXCEPT:
- A) Skin disease
- B) Arthritis
- C) Serositis
- D) Severe lupus nephritis (Class IV)
✅ Answer: D
Explanation: Hydroxychloroquine controls lupus skin disease, arthritis, serositis, mild hematologic abnormalities, and reduces thrombosis risk. It is NOT used for severe lupus nephritis - which requires cyclophosphamide or mycophenolate mofetil. (Goldman-Cecil; Washington Manual)
Q28. Indication for cyclophosphamide in SLE is:
- A) Mild arthralgia
- B) Malar rash
- C) Severe lupus nephritis (Class III/IV)
- D) Drug-induced lupus
✅ Answer: C
Explanation: Cyclophosphamide is indicated for severe organ-threatening SLE, especially Class III/IV lupus nephritis. It is also used for CNS lupus. (Oncourse AI NEET PG; Washington Manual)
Q29. Which biological agent is approved specifically for SLE?
- A) Rituximab
- B) Belimumab
- C) Tocilizumab
- D) Abatacept
✅ Answer: B
Explanation: Belimumab (anti-BLyS/BAFF monoclonal antibody) is FDA-approved specifically for active SLE. Rituximab is used off-label for refractory SLE. (High-yield NEET PG pharmacology)
SECTION 8: ANTIPHOSPHOLIPID SYNDROME & MISCELLANEOUS
Q30. A patient with SLE has recurrent arterial/venous thrombosis, recurrent pregnancy loss, and thrombocytopenia. Anti-cardiolipin antibodies are positive. What is the diagnosis?
- A) Thrombotic thrombocytopenic purpura
- B) Antiphospholipid Antibody Syndrome (APS)
- C) Immune thrombocytopenic purpura
- D) DIC
✅ Answer: B
Explanation: APS (secondary to SLE) presents with thrombosis (arterial/venous), recurrent fetal loss, and thrombocytopenia, with positive antiphospholipid antibodies (anti-cardiolipin, anti-β2GPI, lupus anticoagulant). Hydroxychloroquine reduces thrombosis risk in SLE-APS patients. (Washington Manual; EULAR/ACR 2019 criteria)
Quick Revision - High-Yield Points for NEET PG
| Topic | Key Fact |
|---|---|
| Most sensitive test | ANA |
| Most specific test | Anti-Smith (Anti-Sm) |
| Disease activity marker | Anti-dsDNA, complement (C3/C4) |
| Drug-induced lupus antibody | Anti-histone |
| Classic drug-induced lupus drugs | Procainamide, Hydralazine, INH, Methyldopa, Minocycline |
| Malar rash | Spares nasolabial folds |
| Worst lupus nephritis class | Class IV (diffuse proliferative) |
| Tx in pregnancy | Hydroxychloroquine |
| Biological Tx | Belimumab |
| CRP in SLE flare | NOT elevated (vs bacterial infection) |
| Neonatal heart block | Anti-Ro/SS-A antibodies |
| MCTD antibody | Anti-U1 RNP |
Sources: Harrison's Principles of Internal Medicine 22E, Goldman-Cecil Medicine, Firestein & Kelley's Textbook of Rheumatology, Fitzpatrick's Dermatology, Washington Manual of Medical Therapeutics, Harriet Lane Handbook
pathogenesis of rhemutoid arthritis that is easy to remember and produce in exam
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
I have everything I need - the full pathogenesis, diagrams from Robbins & Kumar and Cellular & Molecular Immunology. Here's a complete, exam-ready breakdown:
Pathogenesis of Rheumatoid Arthritis
Easy to Remember & Write in Exams
The Master Diagram (from Robbins & Cellular/Molecular Immunology)
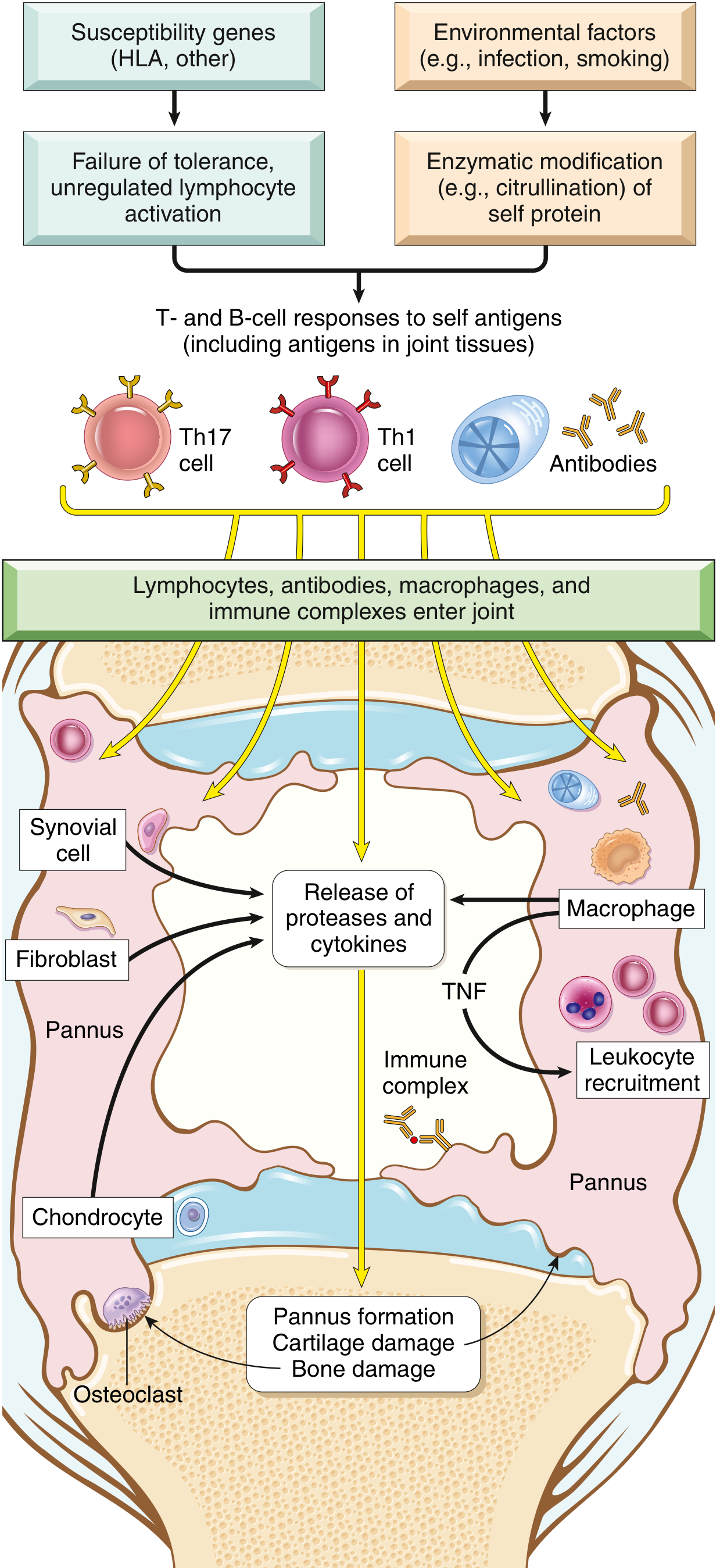
Think of it in 4 Simple Phases
PHASE 1 → PHASE 2 → PHASE 3 → PHASE 4
TRIGGER IMMUNE ENTER DESTROY
RESPONSE JOINT JOINT
PHASE 1 - The Trigger (What starts it?)
Two inputs combine:
A) Genetics (the soil)
- HLA-DR4 (shared epitope) - most important genetic risk
- Also PTPN22 gene polymorphism (tyrosine phosphatase)
- ~50% of RA risk is genetic
B) Environment (the spark)
- Smoking - most important environmental trigger
- Infections (especially periodontitis - Porphyromonas gingivalis)
- These cause CITRULLINATION of self proteins
What is citrullination? Enzymatic conversion of arginine → citrulline in self proteins (fibrinogen, collagen type II, alpha-enolase, vinculin). This creates NEW antigens (neoantigens) that the immune system has no tolerance to.
Memory trick: "Smoke makes proteins dirty (citrullinated) → body attacks them"
PHASE 2 - The Immune Response (Who attacks?)
Citrullinated proteins (ACPA antigens)
↓
Presented by HLA-DR4 to CD4+ T cells
↓
┌──────────┬──────────┐
Th1 cells Th17 cells B cells
↓ ↓ ↓
IFN-γ IL-17 ACPA + RF
Key players:
- Th17 cells - primary driver, secrete IL-17 (recruits neutrophils)
- Th1 cells - secrete IFN-γ (activates macrophages)
- B cells produce two important antibodies:
| Antibody | Full Name | Notes |
|---|---|---|
| ACPA (Anti-CCP) | Anticitrullinated peptide antibody | Present in ~70% RA, specific for RA |
| RF | Rheumatoid Factor (IgM/IgA vs IgG Fc) | Present in ~80% RA, not specific |
ACPA can appear years before joint symptoms - earliest ACPAs are IgA type, suggesting disease starts at mucosal sites (lungs, gut)
PHASE 3 - Entering the Joint (The invasion)
Lymphocytes, antibodies, macrophages, and immune complexes flood the synovium
Inside the joint, macrophages release the big 3 cytokines:
| Cytokine | Main Effect |
|---|---|
| TNF-α | KEY mediator - recruits more cells, activates synoviocytes, most important for joint damage |
| IL-1 | Promotes protease release, bone erosion |
| IL-6 | Systemic inflammation (fever, acute phase proteins) |
IL-17 (from Th17) → recruits neutrophils + monocytes into joint fluid
PHASE 4 - Joint Destruction (The damage)
This is where the histology and pathology happen:
Synoviocyte hyperplasia
+
Dense infiltrate (CD4+ T cells, B cells, plasma cells, macrophages)
+
Increased vascularity (angiogenesis)
+
Neutrophils + fibrin deposits
↓
PANNUS forms
What is Pannus? (Most important morphology term)
A mass of edematous synovium + inflammatory cells + granulation tissue + fibroblasts that grows OVER and ERODES articular cartilage
Pannus destroys by:
- Proteases/collagenases (from synoviocytes + macrophages) → cartilage destruction
- RANKL (expressed on activated T cells) → stimulates osteoclasts → bone resorption → erosions
- Mechanical invasion of pannus into subchondral bone
End result of untreated disease:
Cartilage erosion → Joint space narrowing
Bone erosion → Periarticular erosions
Fibrous ankylosis → Bony ankylosis (ossification)
Complete Flow Chart (Write this in exam)
GENETICS (HLA-DR4, PTPN22)
+
ENVIRONMENT (smoking, infection)
↓
CITRULLINATION of self proteins
(fibrinogen, collagen II, enolase, vinculin)
↓
LOSS OF TOLERANCE
↓
T cell activation (Th1 + Th17) + B cell activation
↓
ACPA + RF production
↓
Lymphocytes + antibodies + macrophages → SYNOVIUM
↓
Cytokine storm: TNF-α, IL-1, IL-6, IL-17
↓
SYNOVIOCYTE HYPERPLASIA → PANNUS formation
↓
Proteases + RANKL → osteoclast activation
↓
CARTILAGE + BONE DESTRUCTION
↓
Joint deformity: ulnar deviation, swan-neck, boutonnière
Key Morphology Points (Histology of RA Synovium)
Five histological features (write all 5 in exams):
- Synoviocyte hyperplasia and proliferation
- Dense infiltrate of CD4+ T cells, B cells, plasma cells, macrophages
- Increased vascularity (angiogenesis)
- Neutrophils + fibrin deposits on synovial surface
- Osteoclastic activity → periarticular erosions + subchondral cysts
Rheumatoid Nodules
- Site: subcutaneous tissue over forearm, elbows, occiput, lumbosacral area
- Feel: small, firm, nontender oval masses
- Histology: necrotizing granulomas (resemble them)
Drugs Linked to Each Pathogenesis Step
| Target | Drug | Mechanism |
|---|---|---|
| TNF-α | Infliximab, Etanercept, Adalimumab | Anti-TNF (most widely used) |
| IL-6 receptor | Tocilizumab | Blocks IL-6R |
| IL-1 | Anakinra | IL-1 receptor antagonist |
| T cell activation | Abatacept | Blocks B7:CD28 costimulation (CTLA-4-Ig) |
| B cells | Rituximab | Anti-CD20 (B cell depletion) |
| JAK signaling | Tofacitinib | JAK inhibitor (small molecule) |
| Conventional | Methotrexate | DMARD (first-line) |
Quick Memory Pegs for Exam
| Fact | Memory |
|---|---|
| Most important cytokine | TNF ("The Number 1 Factor") |
| Most important environmental trigger | Smoking |
| Most important genetic risk | HLA-DR4 (shared epitope) |
| Key chemical modification | Citrullination (Arg → Citrulline) |
| Key destructive structure | PANNUS |
| Bone destruction mediator | RANKL → osteoclasts |
| ACPA positive in | ~70% RA |
| RF positive in | ~80% RA (not specific) |
| Earliest ACPA isotype | IgA (starts at mucosal site) |
| Disease starts in | Mucosal sites (lung, gut) - years before joint disease |
Sources: Robbins & Kumar Basic Pathology; Cellular and Molecular Immunology (Abbas); Firestein & Kelley's Textbook of Rheumatology; Rheumatology 2-Volume Set (Elsevier)
This is a shared conversation. Sign in to Orris to start your own chat.