Visual functions. Age dynamics of their development. Research method
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Here is a comprehensive overview of visual functions, their age-related development, and clinical research methods.
Visual Functions: Age Dynamics and Research Methods
1. The Major Visual Functions
The visual system encompasses several distinct functions that must be assessed individually:
| Function | What it measures |
|---|---|
| Visual acuity (VA) | Spatial resolution — the minimum angle of separation between two resolvable points |
| Contrast sensitivity | Ability to distinguish an object against its background at varying contrast levels |
| Color vision | Discrimination along red–green and blue–yellow axes via three cone populations |
| Visual field | The full extent of spatial vision, tested centrally and peripherally |
| Pupillary reflexes | Integrity of afferent (retinal/optic nerve) and efferent (oculomotor) pathways |
| Stereopsis & binocularity | Depth perception from binocular convergence |
2. Age Dynamics — Development from Birth to Adulthood
Visual functions develop progressively through distinct critical and sensitive periods.
Infancy (0–12 months)
- Newborns have very limited spatial resolution. Vision is estimated at approximately 20/400–20/200 at birth.
- By 3–6 months, an infant should fix and follow a face, toy, or bright light with both eyes individually.
- During this phase, the visual cortex is highly plastic. Ocular dominance columns in layer IVC of primary visual cortex are still forming, receiving segregated input from the two lateral geniculate nucleus layers.
- Hubel and Wiesel's landmark experiments demonstrated that monocular deprivation during the first weeks of postnatal life causes irreversible loss of cortical responsiveness to the deprived eye — the cortical connections underlying visual perception are established within a critical period of early development. Deprivation in adults had no such effect.
Preschool (1–5 years)
- A child aged 6 months to 3 years should fix and follow; formal chart testing is not yet reliable.
- By 36 months, visual acuity testing becomes possible using the "Tumbling E" game, HOTV matching letters, or Allen picture cards. Normal expectation: 20/40 or better, with no more than one line difference between eyes.
- This period encompasses the sensitive period for amblyopia (lazy eye) — reduced central vision from deprivation, strabismus, or unbalanced refractive error without anatomical cause. Most children with amblyopia have no visual complaints, making screening essential.
School age (5–12 years)
- By age 5, children should achieve 20/30 or better; by age 6+ with Snellen, the standard is 20/20.
- Myopia typically emerges in grades 3–4 (~age 9–10), driven by globe elongation. Children with a family history of high myopia (> –6 to –7 D) may be myopic from birth.
- Hyperopia generally requires correction only above +4.00 D, or when strabismus or accommodative difficulty is present.
- The American Academy of Ophthalmology recommends screening at: newborn–3 months, 3–6 months, 6–12 months, 3 years, 5 years, then every 1–2 years after age 5.
Adolescence and young adulthood
- Refractive errors stabilize after adolescence in the absence of disease.
- Normal corrected VA in young adults is frequently better than 6/6 (20/20).
- Contrast sensitivity peaks in young adulthood.
Middle age and beyond
- Presbyopia develops with loss of lens accommodation, requiring reading glasses in emmetropes (or bifocals in those already corrected for distance).
- Contrast sensitivity, color discrimination (particularly blue–yellow axis), and scotopic sensitivity progressively decline.
- The visual field threshold ("hill of vision") decreases with age; automated perimetry compares results against age-matched normative databases.
3. Research Methods — Clinical Assessment of Visual Functions
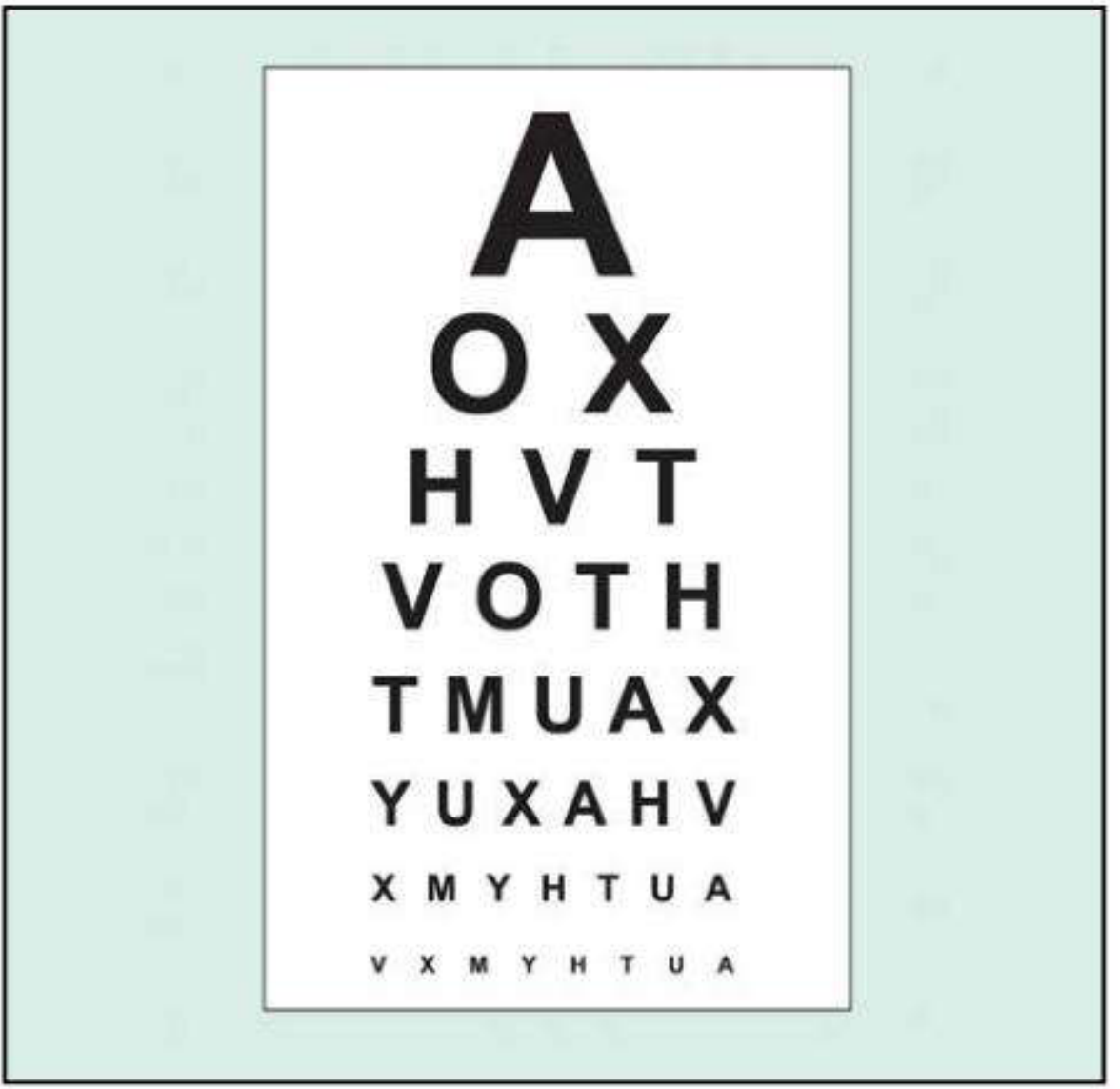
3.1 Visual Acuity
Snellen chart — the standard tool, used at 6 m (20 ft). The patient reads progressively smaller optotypes; normal is 6/6 (20/20). The worst eye is tested first with the fellow eye occluded.
- Rosenbaum card (portable near version) — held at 36 cm; requires reading glasses for presbyopic patients.
- Pinhole test — a ~1 mm aperture compensates for refractive error. If VA improves through the pinhole, a refractive cause is likely. Note: pinhole VA may be worse than spectacle correction in macular disease.
- Best-corrected VA (BCVA) — acuity measured with optimal refractive correction; the gold standard for most clinical decisions.
Scales for very poor VA (in ascending order):
- No light perception (NLP)
- Light perception (LP)
- Hand movements (HM)
- Counting fingers (CF) — recorded at the distance tested (e.g., CF at 1 m)
Age-specific testing methods:
| Age | Method |
|---|---|
| 0–3 months | Fix and follow (face, light, toy) |
| 3 months – 3 years | Fix and follow with each eye individually |
| 3–5 years | Tumbling E, HOTV letters, Allen picture cards (at 10 ft) |
| ≥5–6 years (literate) | Standard Snellen chart at 20 ft |
| Illiterate / cognitive disability | Tumbling E chart |
Legal blindness (IRS definition): best-corrected VA ≤ 6/60 (20/200) in the better eye, or binocular visual field ≤ 20°.
3.2 Contrast Sensitivity
Contrast sensitivity measures the ability to discriminate an object from its background — a different dimension to spatial resolution and not captured by Snellen alone.
- Pelli–Robson chart — viewed at 1 m; rows of equal-size letters with decreasing contrast (0.15 log-unit steps per group of three). The patient reads until the lowest-resolvable group is reached. Detects deficits in amblyopia, optic neuropathy, and cataract even when Snellen VA is preserved.
- Sinusoidal grating tests — the patient views gratings of decreasing contrast across spatial frequencies.
- SPARCS (Spaeth-Richman Contrast Sensitivity Test) — computer-based, usable in illiterate patients; tests both central and peripheral contrast sensitivity.
3.3 Color Vision
Color vision depends on three cone populations:
- Short-wave (blue/tritan) — peak 414–424 nm
- Medium-wave (green/deuteran) — peak 522–539 nm
- Long-wave (red/protan) — peak 549–570 nm
Congenital color deficiency (CVD): X-linked recessive; affects ~8% of Northern European men and 0.5% of women. Most are anomalous trichromats with red–green deficiency. Types include protanomaly (2% of men), deuteranomaly (6% of men), and tritanomaly (rare, blue–green).
Acquired defects: Macular disease → blue-yellow axis; optic nerve disease → red-green axis.
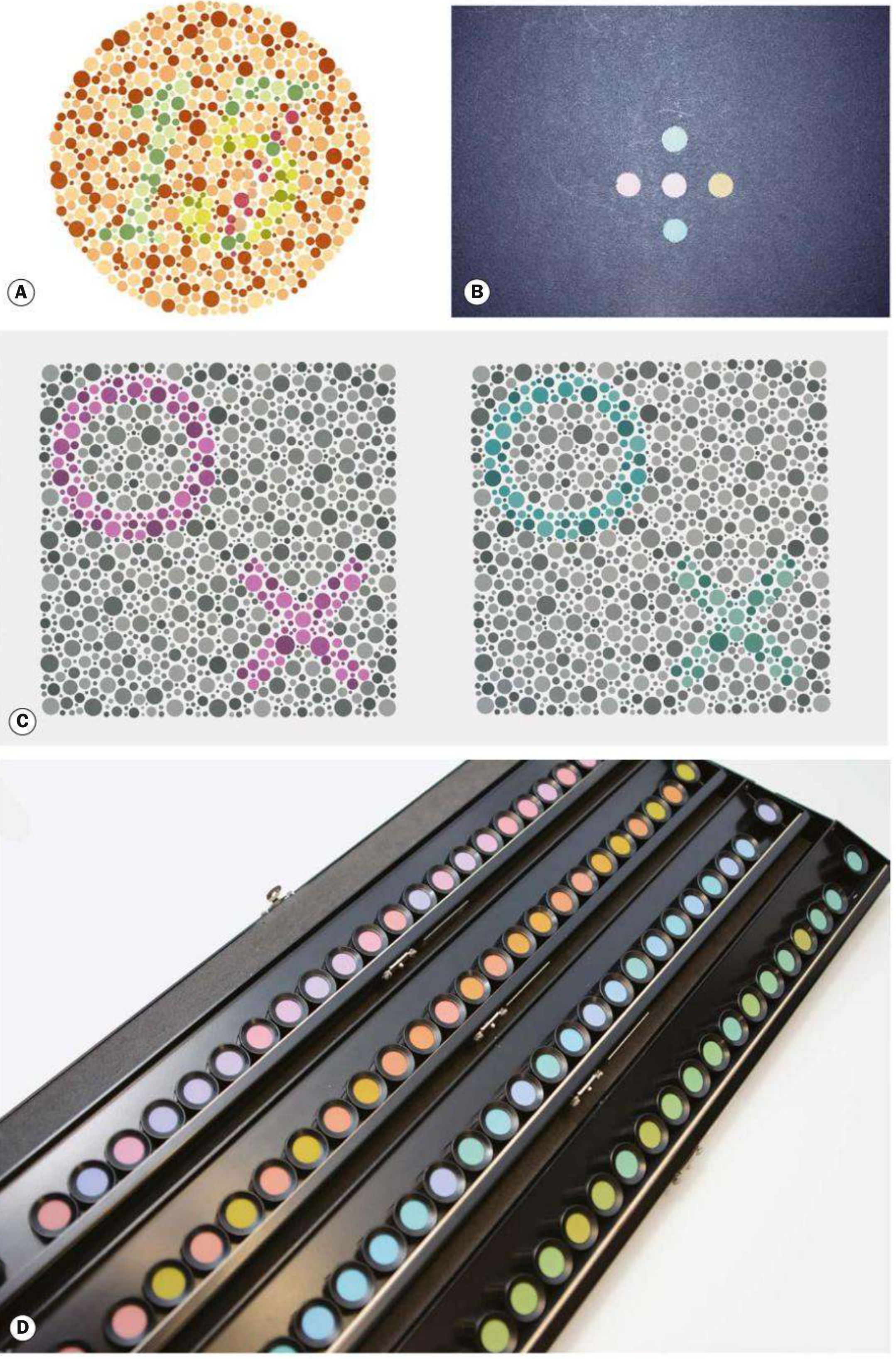
Testing instruments:
| Test | Use |
|---|---|
| Ishihara pseudoisochromatic plates (16 plates) | Screening for congenital protan/deuteran defects; also optic nerve function |
| Hardy–Rand–Rittler (HRR) | Detects protan, deuteran, and tritan defects |
| City University test | Arrangement test for acquired and congenital defects |
| Farnsworth–Munsell 100-hue test | Detailed classification; sensitive for subtle acquired defects; arranges 100 colored caps in hue order |
3.4 Visual Field
The visual field is the total area of space visible with a steady, forward gaze.
Confrontation testing — bedside screening; examiner moves fingers from the periphery toward the center in all quadrants. Detects gross hemianopias and quadrantanopias but misses subtle defects.
Amsler grid — evaluates the central 20° around fixation; principally screens for and monitors macular disease and central scotomas. Patients at risk of macular neovascularization can use it at home.
Perimetry — the formal standard:
- Goldmann kinetic perimetry — manual; a stimulus of fixed size and intensity is moved from non-seeing periphery inward; contour lines (isopters) map the "hill of vision" across the full field.
- Automated static perimetry (e.g., Humphrey Field Analyzer) — stimuli presented at fixed locations; threshold luminance is determined by staircase algorithms. Compares results to age-matched normative data.
- Threshold strategies (e.g., SITA-Standard, SITA-Fast): accurate, used for glaucoma monitoring.
- Suprathreshold strategies: rapid screening — tests whether stimuli visible to a normal age-matched person can be detected.
- Common patterns: 24-2 (central 24°, standard glaucoma), 30-2, 10-2 (central 10°, advanced glaucoma), FF-120 (neurological defects).
Tangent screen (Bjerrum screen) — office-based; white stimulus on black background, useful for central field assessment at variable distances (a field that does not expand with increasing distance suggests non-organic "tubular" constriction).
3.5 Pupils
Pupillary responses assess the afferent pathway (retina → optic nerve → pretectal nucleus) and efferent pathway (oculomotor nerve → iris sphincter). Testing in dim light with distant fixation:
- Direct light reflex — illuminated eye constricts
- Consensual reflex — fellow eye constricts simultaneously
- Relative afferent pupillary defect (RAPD) — swinging flashlight test; dilation of the tested eye as light swings to it indicates unilateral optic neuropathy
- Near response — tested only when light response is abnormal; light-near dissociation occurs in neurosyphilis (Argyll Robertson pupil), dorsal midbrain lesions (Parinaud syndrome), and Adie's tonic pupil
3.6 Electrophysiological Methods
Used when subjective testing is unreliable (infants, non-cooperative patients) or to objectively localize dysfunction:
- Visual evoked potentials (VEP) — cortical response to visual stimuli; delays indicate optic nerve disease
- Electroretinography (ERG) — retinal function; pattern ERG isolates macular/ganglion cell function
- Preferential looking / Teller acuity cards — behavioral estimate of grating acuity in infants based on preference for patterned over blank stimuli
Summary: Age Norms for Visual Acuity
| Age | Expected acuity / behavior |
|---|---|
| Newborn | Fix and follow a face/light |
| 6 months – 3 years | Fix and follow each eye individually |
| 3 years | 20/40 or better; ≤1 line interocular difference |
| 5 years | 20/30 or better |
| ≥6 years | 20/20 (6/6) |
| Middle age | Presbyopia onset; distance VA maintained with correction |
| Elderly | Progressive decline in contrast sensitivity, color discrimination, field sensitivity |
Sources: Harrison's Principles of Internal Medicine 22e; Kanski's Clinical Ophthalmology 10th ed.; Tintinalli's Emergency Medicine; Textbook of Family Medicine 9e; Kandel's Principles of Neural Science 6th ed.; Bradley & Daroff's Neurology in Clinical Practice.
This is a shared conversation. Sign in to Orris to start your own chat.