Clavicle fractures surgical treatment
Reading File
Finding Sources
Searching PubMed
"clavicle fracture" AND "surgical fixation"
Reading File
Searching PubMed
"clavicle fracture" AND surgery
Finding Sources
Searching Images
clavicle fracture plate fixation surgical treatment
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed for a comprehensive answer. Here is the complete synthesis:
Clavicle Fractures: Surgical Treatment
Source: Rockwood and Green's Fractures in Adults, 10th ed. 2025; Miller's Review of Orthopaedics, 9th ed.
Anatomy & Deforming Forces
The clavicle serves as the only bony strut connecting the axial skeleton to the upper limb. With a displaced midshaft fracture, characteristic deformity results from:
- Sternocleidomastoid pulls the proximal fragment superiorly and posteriorly
- Pectoralis major, deltoid, and gravity pull the distal fragment anteriorly, medially, and inferiorly
- The scapula protracts as a result, shortening the shoulder girdle
Classification
| Region | Frequency | Key Subtypes |
|---|---|---|
| Midshaft (Group I) | 80–85% of clavicle fractures | Transverse, oblique, comminuted, segmental |
| Lateral (Group II / Neer) | ~15% | Neer I (stable), Neer IIA/B (unstable — CC ligaments disrupted), Neer III (AC joint involvement) |
| Medial (Group III) | ~5% | Often physeal in young patients; CT essential |
Surgical Indications
Absolute Indications
- Open fracture
- Vascular injury requiring repair
- Progressive neurologic deficit (brachial plexus tethering)
- Scapulothoracic dissociation
Relative Indications — Midshaft
| Category | Factors |
|---|---|
| Fracture-specific | Displacement >2 cm, shortening >2 cm, increasing comminution, segmental fracture, obvious clinical deformity, scapular malposition/winging |
| Associated injuries | Multiple ipsilateral rib fractures, "floating shoulder" (displaced glenoid neck + clavicle fracture), ipsilateral upper extremity fractures |
| Patient factors | Polytrauma requiring early UE weight-bearing; elite athlete or high-demand professional; high overhead functional requirements; female sex + unfavorable fracture pattern |
Most clavicle fractures can and should be treated nonoperatively. Operative repair is reserved for medically well, physically active patients who stand to benefit most from rapid restoration of anatomy. — Rockwood and Green's, p. 1209
Timing of Surgery
- Ideally within 2–3 weeks of injury for easiest reduction
- Delayed fixation (>3 weeks) risks brachial plexus tethering to the inferior clavicle surface — iatrogenic brachial plexus injury has been reported as a complication of delayed fixation
- For IM nailing specifically, closed reduction is often only possible within the first week
Surgical Options: Midshaft Fractures
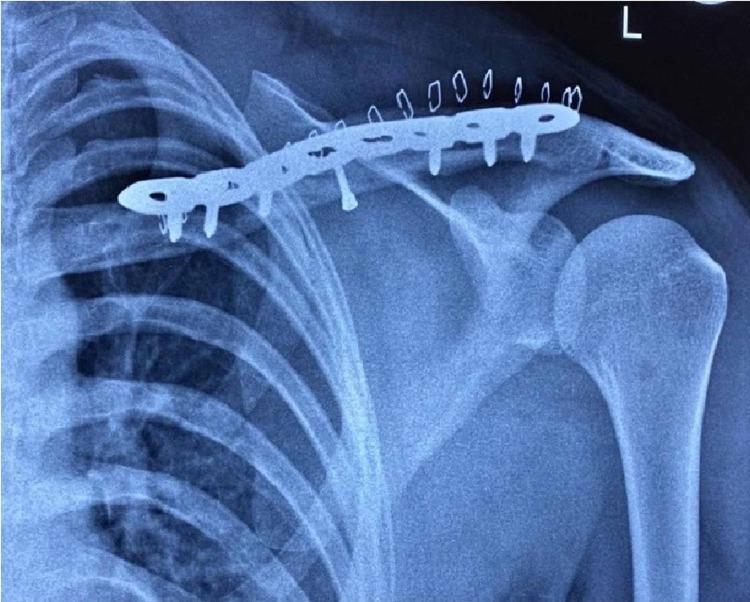
1. Plate Fixation (ORIF) — Gold Standard
Most popular and most studied technique for displaced midshaft fractures.
Plate Position Options
| Approach | Advantages | Disadvantages |
|---|---|---|
| Anterosuperior | Familiar, easy radiographic monitoring, easily extensile | Superior→inferior drill trajectory risks lung/vessels; narrow superoinferior dimension (screws typically 14–18 mm) |
| Anteroinferior | Safer screw trajectory, longer screws in AP dimension, less hardware prominence, lower removal rate (5% vs 11%, p=0.008) | Less familiar, obscures fracture site on X-ray |
Plate selection:
- Precontoured anatomic plates are preferred — fit the S-shape of the clavicle, reduce need for intraoperative bending, lower subsequent hardware removal rates
- Modern plates combine locking and dynamic compression holes (variable-angle locking options available)
- 3.5-mm plates are standard; 2.7-mm dual mini-plating is an emerging option with similar union rates and lower implant-related irritation in meta-analysis
- Locking screws are useful in osteoporotic bone or to reduce periosteal blood supply compromise
- Cerclage wires in isolation are inadequate and should be avoided
Technique key steps:
- Beach-chair/semisitting position, small pad behind shoulder to elevate it
- Oblique or vertical incision centered over fracture
- Preserve supraclavicular nerve branches (peri-incisional numbness is a common postop complaint)
- Reduce with small-fragment forceps; lag screw for anterosuperior wedge fragment if present
- Apply precontoured plate with ≥3 bicortical screws on each side of fracture
- Close platysma and skin in separate layers
Postoperative protocol:
- Sling for comfort, pendulum exercises immediately
- Wound check at 10–14 days
- Full ROM (no strengthening) until 6 weeks
- Radiographs at 6 weeks; if healing evident, progressive strengthening begins
- Return to contact sport/heavy labor typically at 3–4 months
2. Intramedullary (IM) Pinning
Advantages:
- Smaller, more cosmetic incisions
- Less soft tissue stripping and periosteal devascularization
- Potential for easier hardware removal
Disadvantages:
- Poor rotational and axial control with unlocked/smooth pins — unsuitable for unstable or comminuted fractures
- High hardware migration and prominence rates with older devices
- Must be performed early (within ~1 week) for closed reduction
- Higher hardware removal rates than plate fixation
Device selection: Locked IM devices have significantly lower removal rates than unlocked pins. Avoid smooth pins in comminuted fractures.
Pitfalls:
- Ensure IM canal is large enough for planned device
- Avoid using IM device as a joystick (iatrogenic comminution)
- Do not pass instruments extraosseously posterior/inferior (neurovascular risk)
- Preserve supraclavicular nerve branches
3. External Fixation
- Technically feasible; avoids retained hardware
- Useful for severely compromised soft tissue envelope
- Limited acceptance due to pin prominence and practical difficulties; rarely used in routine practice
Surgical Options: Lateral (Distal) Clavicle Fractures
Neer IIA and IIB fractures are unstable because the CC ligaments remain attached to the distal fragment/coracoid, pulling it inferiorly while the proximal fragment displaces superiorly.
Available techniques:
- Precontoured locking plate (most popular currently)
- Hook plate — "hook" inserts into subacromial space posteriorly; provides stable fixation but requires planned removal (risk of subacromial impingement if left in)
- Coracoclavicular (CC) fixation — suture-button device, suture anchor, or cortical screw through the CC interval
- Tension band wiring
- Transacromial K-wire fixation
- Arthroscopically assisted techniques
Technical challenge: The distal fragment is often small and cancellous with inferior bone quality. A backup plan must be available intraoperatively — if distal locking screws provide insufficient purchase, convert to hook plate or augment with CC suture-button.
Lateral plate key steps:
- Beach-chair position; fluoroscopy is mandatory to confirm screws do not violate the AC joint
- Expose fracture, reduce distal fragment (elevate to meet proximal), provisional K-wire or lag screw
- Apply anatomic precontoured lateral plate with multiple 2.7-mm locking/variable-angle screws distally
- Assess stability; convert to hook plate or add CC fixation if inadequate
- Final fluoroscopic check before closure
Medial Clavicle Fractures
- Rare; often physeal fractures in adolescents/young adults
- Posterior displacement is an emergency — CT first to evaluate mediastinal impingement; may require cardiothoracic surgery backup
- Anterior: can often manage with closed reduction; unstable cases may need ORIF with mini-fragment LCP or CC reconstruction plate spanning sternum
Complications
| Complication | Notes |
|---|---|
| Hardware prominence/irritation | Most common reason for hardware removal; lower with anteroinferior plating |
| Hardware removal | ~5–11% depending on plate position; more frequent with superior plating and unlocked IM pins |
| Nonunion | <1% with operative treatment vs. 5–10% with nonoperative in high-risk displaced fractures |
| Malunion | Residual shortening >2 cm associated with weakness and TOS; corrective osteotomy is effective |
| Thoracic outlet syndrome (TOS) | Most common "neurovascular injury" after displaced clavicle fractures; results from change in thoracic outlet geometry; treat with corrective osteotomy (not first rib resection alone) |
| Brachial plexus injury | Can occur acutely (stretch) or iatrogenically during delayed fixation (tethering) |
| Infection | Superficial wound infection ~1–2%; deep infection requires hardware removal if union achieved |
| Pneumothorax | Rare from drill plunge with superior plate |
| Re-fracture after hardware removal | Patients should avoid high-risk activities after removal until full remodeling |
Outcomes Summary
- Plate fixation produces higher union rates, faster return to function, and lower nonunion rates than nonoperative treatment in displaced fractures — supported by multiple RCTs and systematic reviews
- Anteroinferior vs. anterosuperior plating: equivalent clinical outcomes; slight advantage for anteroinferior regarding hardware removal
- IM nailing with locked devices produces comparable results to plate fixation in appropriately selected (non-comminuted) fractures, with smaller scars
- For adolescents, operative treatment is not routinely superior; reserve for older, larger adolescents with severe displacement/shortening
Recent literature note:
- PMID 38281678 (Sys Rev, 2024): Displaced distal clavicle fractures may have inferior outcomes with nonoperative management
- PMID 40087117 (Sys Rev, 2025): Hook plates vs. locking plates for Neer IIB fractures — comparative systematic review (2025)
- PMID 40022180 (Sys Rev, 2025): Midshaft fractures with associated ipsilateral AC joint injuries — surgical management nuances
— Rockwood and Green's Fractures in Adults, 10th ed. 2025, Chapter 34; Miller's Review of Orthopaedics, 9th ed.
Tens nailing in clavicle fracture
Finding Sources
Searching PubMed
"TENS nail" AND clavicle
Finding Sources
Searching PubMed
"elastic stable intramedullary nail" AND clavicle
Reading File
Finding Sources
Reading File
Reading File
Searching Images
TENS TEN titanium elastic nail intramedullary clavicle fracture technique
Loading Image
Loading Image
Loading Image
I now have all the material needed for a comprehensive, well-illustrated answer.
TENS/TEN Nailing in Clavicle Fractures
TEN = Titanium Elastic Nail | also called ESIN = Elastic Stable Intramedullary Nailing
What Is a TEN?
The Titanium Elastic Nail is a smooth, flexible, small-diameter intramedullary implant made of titanium. It is pre-bent and inserted into the medullary canal of the clavicle, where its elasticity generates three-point bending forces that confer relative stability. It is the same implant used for pediatric long bone fractures (femur, tibia, forearm). It is cheap, widely available, and straightforward to remove.
Biomechanical Principle & Limitations
Because TENs are unlocked (no rotational or axial locking mechanism), they provide:
- ✅ Restoration of length and alignment in simple, stable fracture patterns
- ❌ Poor rotational control — the clavicle can rotate around the nail
- ❌ Poor axial control — the nail cannot prevent telescoping/shortening
- ❌ Unsuitable for comminuted or unstable fractures — loss of length and rotation are major risks
A biomechanical study (Golish et al.) comparing 3.5-mm compression plates to 3.8–4.5-mm IM pins showed plate constructs were superior in resisting displacement in all testing modes (maximal load, cyclical stress). — Rockwood and Green's, p. 1210
Patient Selection (Indications)
| Suitable | Not Suitable |
|---|---|
| Simple transverse or short oblique midshaft fracture | Comminuted fracture |
| Adequate medullary canal size | Narrow or tortuous canal |
| Patient willing to undergo elective hardware removal | Patient preference against second procedure |
| Younger patients / smaller frame | Large, high-demand patients |
| Early presentation (<1 week) — closed reduction possible | Delayed presentation (>1–2 weeks) — open reduction often required |
Surgical Technique
Preoperative Planning Checklist
- Radiolucent or shoulder table
- Semisitting position with small pad between scapulae (lets shoulder fall back, aiding reduction)
- C-arm placed contralaterally or cranially
- Confirm IM canal diameter pre-op on X-ray — select nail diameter accordingly
- If older than ~10–14 days: plan for open reduction
Positioning
- Semisitting / beach-chair on radiolucent table
- Head turned to contralateral side and taped
- Pad between scapulae
- Arm may be free-draped if difficult reduction anticipated (significant shortening)
Insertion: Retrograde Technique (most common)

- Entry portal: Small incision (~1–2 cm) over the posterolateral clavicle, 2–3 cm medial to the AC joint
- Breach the posterior cortex with a drill or awl (entry must be confirmed fluoroscopically)
- Pass TEN retrograde through the lateral/distal fragment toward the fracture site
- Reduce the fracture — either percutaneously (preferred) using:
- Percutaneous reduction clamp on the medial fragment
- TEN as a joystick in the distal fragment (caution: risk of bending/breaking the nail)
- Or "inside-out" technique: pass nail out through fracture site, reduce, then drive into medial fragment
- Under fluoroscopic control, advance TEN across the fracture and seat it in the medial fragment
- Verify length, alignment, and rotation clinically and fluoroscopically
- Cut nail flush with the insertion site posterolaterally
- Close in layers (typically 2 layers)
Closed reduction is usually only achievable in the first 7–10 days post-injury. Beyond that, open reduction is required. — Rockwood and Green's, p. 1210
Antegrade Technique
- Entry at the anteromedial clavicle near the SC joint
- Less commonly used
- Advantage: may be technically easier in certain body habitus
Postoperative Protocol
- Simple sling for comfort postoperatively
- Wound check at 2 weeks
- Gentle ROM instituted early if reduction is stable
- Radiographs at 6 weeks — if healing satisfactory, progressive active exercises begin
- Hardware removal is planned once union is confirmed (typically 3–4 months); often done under local anesthetic given the subcutaneous position
Radiographic Appearances
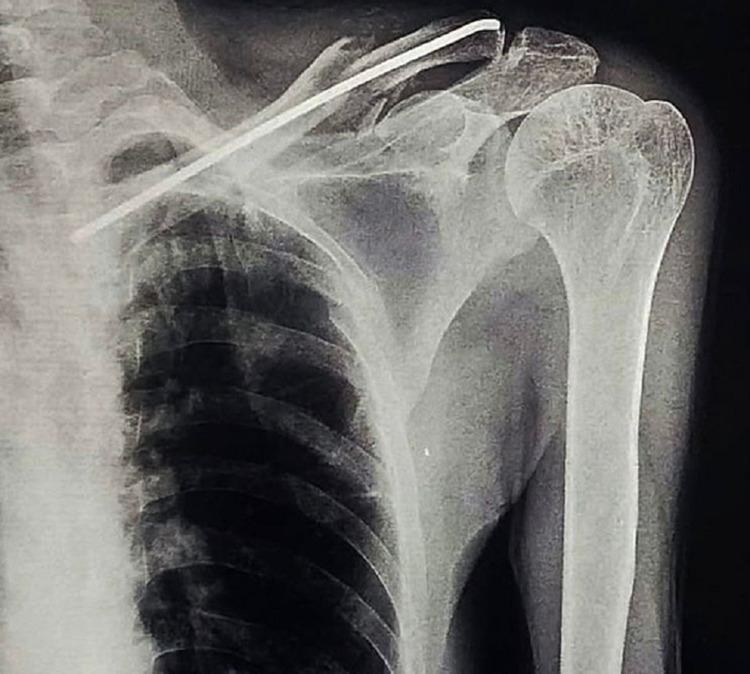

The series above illustrates the telescoping complication in a comminuted fracture — exactly why TENs should be reserved for simple fracture patterns.
Outcomes vs. Plate Fixation
| Parameter | TEN | Plate |
|---|---|---|
| Functional scores at 1 year | Excellent (Constant ~95–96) | Excellent (Constant ~95–96) |
| Early function (up to 6 months) | Slower recovery | Faster |
| Union rate | Similar | Similar |
| Operative time | Shorter | Longer |
| Blood loss | Less | More |
| Cosmesis | Better (smaller scar) | Worse |
| Hardware removal | Routine / expected (~20–100% depending on device) | Selective (~5–11%) |
| Comminuted fractures | Inferior — slower recovery, higher failure | Preferred |
Key RCT data (Van der Meijden et al., 120 patients): Both groups had excellent 1-year results; the plate group had less early disability (up to 6 months). TEN removal was recommended for all patients vs. only one request in the plate group.
A recent meta-analysis of 895 patients showed better functional outcomes with IM nailing than plate fixation, but sensitivity analysis revealed this was solely attributable to locking IM nails — not standard smooth TENs. — Rockwood and Green's, p. 1211
Complications
| Complication | Details |
|---|---|
| Hardware migration | Most common and serious — smooth nail can migrate medially toward great vessels or laterally through AC joint |
| Telescoping / shortening | Nail fails to maintain length in comminuted patterns; medial end protrudes through entry site |
| Hardware prominence/irritation | Often requires removal |
| Nail breakage | Particularly if used as joystick; more common in larger/heavier patients |
| Rotation malunion | Difficult to control rotation without locking |
| Peri-incisional numbness | Supraclavicular nerve branches cut during entry |
| Failure in comminuted fractures | Significantly inferior outcomes; avoid unlocked TENs in this setting |
| Re-fracture after removal | Rare; patients should avoid high-risk activity post-removal |
Surgical Pitfalls & Prevention
| Pitfall | Prevention |
|---|---|
| Inability to pass TEN | Pre-op canal sizing; have drill/awl available |
| Iatrogenic comminution | Do not use TEN as lever; maintain reduction while advancing |
| Neurovascular injury | Do not pass instrument extraosseously posterior/inferior |
| Nail migration | Use locked devices when possible; cut nail flush with cortex |
| Malunion/shortening | Avoid in comminuted fractures; use locking IM nail if canal allows |
Locking IM Nails — The Next Step
Newer-generation locking IM clavicle nails (e.g., modified Hagi/Rockwood pin with threaded medial end + compression nut, or large-diameter lockable nails) address the core limitation of the TEN:
- Threaded/locked ends prevent migration and rotation
- Axial control allows use in more comminuted patterns
- Hardware removal rates are lower than smooth TENs (~22% vs. routine removal)
- One meta-analysis showed superior functional outcomes with locked IM nails vs. plates — not seen with unlocked TENs
Locking IM pins represent a promising alternative that may finally make nailing a serious competitor for plate fixation in clavicle fractures. — Rockwood and Green's, p. 1211
Summary: When to Choose TEN
✅ Use TEN when:
- Simple transverse/short oblique midshaft fracture
- Canal accommodating (confirm on pre-op imaging)
- Patient values cosmesis (smaller scar) and accepts planned hardware removal
- Early presentation allowing closed reduction
- Pediatric/adolescent patients
❌ Avoid TEN when:
- Comminuted, segmental, or butterfly fragment fractures
- Narrow or tortuous medullary canal
- Delayed presentation (>2 weeks) with difficult reduction anticipated
- Large, high-demand patient requiring rigid fixation
— Rockwood and Green's Fractures in Adults, 10th ed. 2025, Chapter 34
Tens nail in clavicle fracture
The previous response already covered this topic in full detail. Here is a structured summary of everything covered:
TEN (Titanium Elastic Nail) in Clavicle Fractures — Summary
What It Is
A smooth, flexible, small-diameter titanium intramedullary implant inserted into the clavicle's medullary canal. Same implant used for pediatric long bone fractures. Also called ESIN (Elastic Stable Intramedullary Nailing).
Key Biomechanical Facts
- Works by 3-point bending inside the canal
- Unlocked → poor rotational AND axial control
- Cannot prevent telescoping/shortening
- Biomechanically inferior to plate fixation in all loading modes (Golish et al.)
- Best suited only for simple, stable fracture patterns
Ideal Patient
| ✅ Choose TEN | ❌ Avoid TEN |
|---|---|
| Simple transverse / short oblique midshaft | Comminuted or segmental fracture |
| Adequate canal size (confirm pre-op) | Narrow/tortuous canal |
| Early presentation <1–2 weeks | Delayed >2 weeks (closed reduction fails) |
| Patient accepts planned hardware removal | Patient wants single surgery |
| Younger patient, cosmesis priority | Large, high-demand patient |
Technique (Retrograde — Most Common)
Setup: Semisitting/beach-chair, radiolucent table, pad between scapulae (lets shoulder fall back → aids reduction), C-arm contralateral or cranial
Steps:
- Small incision (~1–2 cm) posterolateral clavicle, 2–3 cm medial to AC joint
- Breach posterior cortex with drill or awl
- Pass TEN retrograde through distal fragment to fracture site
- Reduce fracture — percutaneously (preferred, especially within first week) or open
- Percutaneous clamp on medial fragment
- TEN as joystick in distal fragment (caution: bending/breaking risk)
- Or "inside-out": pass nail out at fracture site → reduce → drive into medial fragment
- Advance TEN across fracture, seat in medial fragment under fluoroscopy
- Verify length, alignment, rotation clinically + fluoroscopically
- Cut nail flush with posterolateral cortex
- Two-layer closure
Antegrade option: Entry at anteromedial clavicle near SC joint — less common
Postoperative Protocol
- Sling for comfort
- Wound check at 2 weeks
- Early ROM if stable
- X-ray at 6 weeks → progressive strengthening
- Planned hardware removal once united (~3–4 months), often under local anesthetic
Outcomes vs. Plate
| Parameter | TEN | Plate |
|---|---|---|
| 1-year function | Equivalent (Constant ~95–96) | Equivalent |
| Early recovery (0–6 months) | Slower | Faster |
| Union rate | Similar | Similar |
| Op time / blood loss | Less | More |
| Scar / cosmesis | Better | Worse |
| Hardware removal | Routine / near 100% | Selective (~5–11%) |
| Comminuted fractures | Inferior | Preferred |
Key finding: A meta-analysis of 895 patients showed better functional outcomes with IM nailing vs. plates — but sensitivity analysis showed this was solely due to locking IM nails, not smooth TENs. — Rockwood and Green's, 10th ed.
Complications
| Complication | Mechanism |
|---|---|
| Nail migration | Most dangerous — medially toward great vessels or through AC joint |
| Telescoping/shortening | Axial instability in comminuted patterns; medial end protrudes |
| Rotation malunion | No rotational control |
| Nail breakage | Excessive joysticking; large/heavy patients |
| Hardware prominence | Requires removal |
| Peri-incisional numbness | Supraclavicular nerve branches at entry site |
Surgical Pitfalls
| Pitfall | Prevention |
|---|---|
| Can't pass nail | Pre-op canal size check |
| Iatrogenic comminution | Don't use as lever; maintain reduction while advancing |
| Neurovascular injury | Never pass instrument extraosseously posterior/inferior |
| Migration | Cut flush; use locking device if possible |
| Shortening | Avoid in comminuted; switch to locking nail |
Locking IM Nails — Evolution Beyond TEN
Newer devices (Hagi pin, Rockwood pin — threaded medial end + compression nut; large-diameter lockable nails) solve TEN's core weakness:
- Prevent migration and rotation
- Maintain axial length → usable in more comminuted patterns
- Removal rates ~22% (vs. near 100% for smooth TENs)
- The only IM devices shown to outperform plates in meta-analysis
Source: Rockwood and Green's Fractures in Adults, 10th ed. 2025, Chapter 34
Tendons around ankle joints
Reading File
Finding Sources
Searching Images
tendons around ankle joint anatomy diagram
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the complete answer.
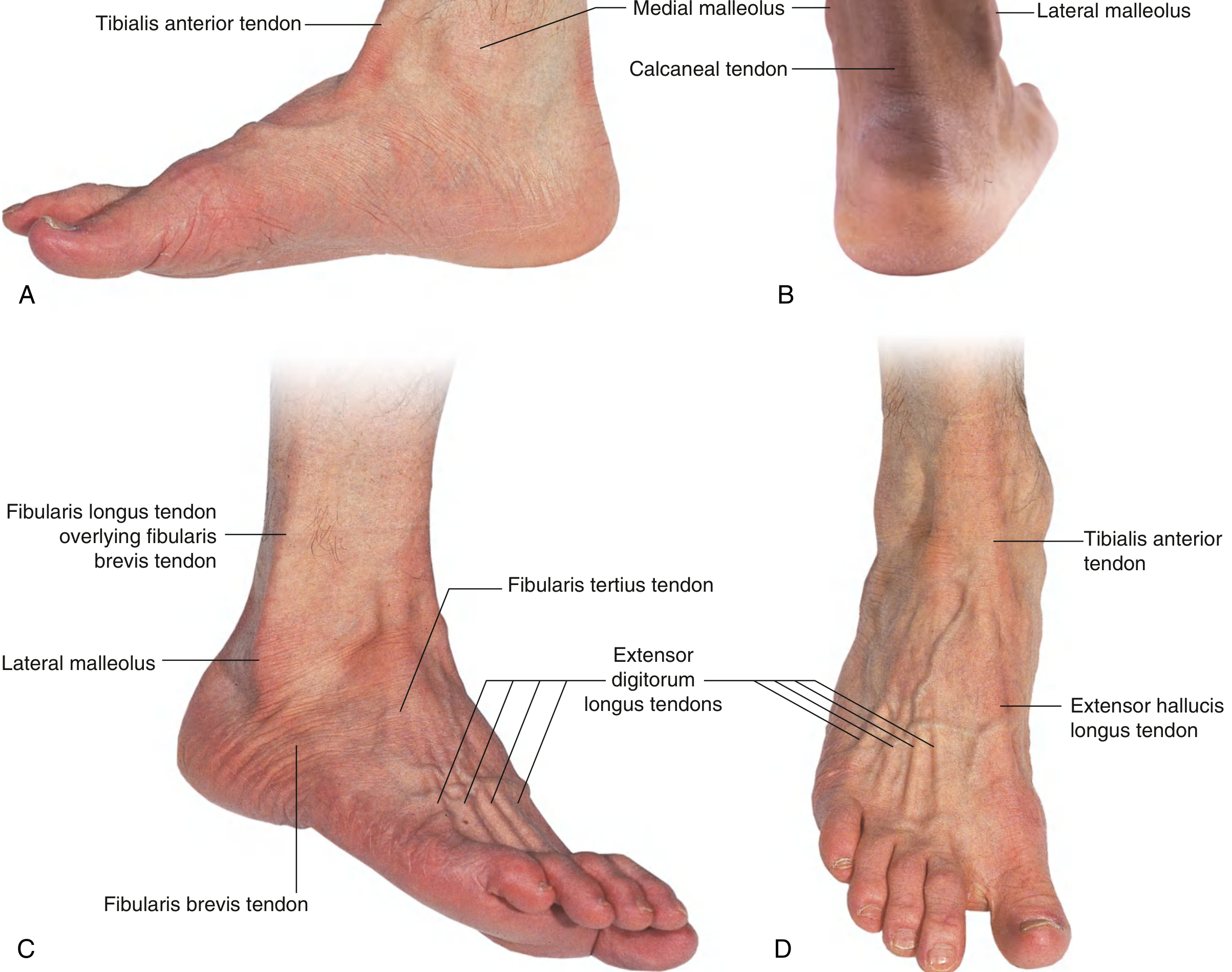
Tendons Around the Ankle Joint
Sources: Gray's Anatomy for Students; Imaging Anatomy (Thieme), Vol. 3; Rosen's Emergency Medicine; Gray's Atlas of Anatomy
Overview: Four Compartmental Groups
Tendons at the ankle are organized into four anatomic groups, each held in place by a retinaculum:
| Group | Retinaculum | Tendons |
|---|---|---|
| Medial (posterior to medial malleolus) | Flexor retinaculum | Tibialis posterior, Flexor digitorum longus, Flexor hallucis longus |
| Lateral (posterior to lateral malleolus) | Superior & inferior peroneal retinaculum | Peroneus (fibularis) longus, Peroneus (fibularis) brevis |
| Anterior (over dorsum) | Superior & inferior extensor retinaculum | Tibialis anterior, Extensor hallucis longus, Extensor digitorum longus, Fibularis (peroneus) tertius |
| Posterior (midline) | None (paratenon only) | Achilles (calcaneal) tendon, Plantaris tendon |
1. Medial Tendons — Tarsal Tunnel (Posteromedial)
Held behind the medial malleolus by the flexor retinaculum (triangular fibrous band from medial malleolus → calcaneus → plantar aponeurosis).
The contents of the tarsal tunnel from anterior to posterior follow the mnemonic:
"Tom, Dick, And Very Nervous Harry" Tibialis posterior → Digitorum longus (FDL) → posterior tibial Artery + Veins → tibial Nerve → flexor Hallucis longus (FHL)
Tibialis Posterior (TP)
- Largest of the three medial tendons (~twice the diameter of FDL on cross-section)
- Origin: proximal 2/3 of tibia, fibula, and interosseous membrane
- Runs behind medial malleolus in a dedicated groove
- Primary insertion: navicular tuberosity; also sends slips to cuneiforms, 2nd–4th metatarsal bases, cuboid, and sustentaculum tali
- Function: plantar flexion + inversion; primary supporter of the medial longitudinal arch
- Pathology: most common medial ankle tendon to be injured; rupture → progressive flat foot (pes planus)
- May be associated with an accessory navicular bone (types 1, 2, 3)
Flexor Digitorum Longus (FDL)
- Runs posterior to TP behind the medial malleolus; crosses TP (the "chiasma crurale") at the distal leg
- Within the tarsal tunnel: lies inferior to TP
- On the sole: crosses over FHL (the "Knot of Henry") and receives the quadratus plantae
- Divides into 4 slips → inserts on distal phalanges of toes 2–5
- Function: flexion of toes 2–5; also plantar flexion and inversion
Flexor Hallucis Longus (FHL)
- Lies most posteriorly in the tarsal tunnel (just behind the neurovascular bundle)
- Passes in a groove on the posterior surface of the talus and under the sustentaculum tali
- Inserts on the distal phalanx of the great toe
- Function: flexion of great toe; plantar flexion (important push-off power)
- Classic association: ballet dancers (FHL tenosynovitis)
- Separated from the Achilles tendon only by its own tendon; important surgical landmark
2. Lateral Tendons — Peroneal (Fibular) Tendons
Held in the retromalleolar groove behind the lateral malleolus by the superior peroneal retinaculum (SPR) and further distally by the inferior peroneal retinaculum.
Peroneus (Fibularis) Longus (PL)
- Origin: lateral condyle of tibia, proximal 2/3 of fibula, intermuscular septum
- In the retromalleolar groove: lies posterolateral to peroneus brevis (i.e., more superficial/posterior)
- Passes under the cuboid in a dedicated groove → runs obliquely medially → inserts on the lateral tubercle of 1st metatarsal and plantar surface of medial cuneiform
- Function: plantarflexion + eversion; supports the transverse arch and lateral longitudinal arch
- May contain an os peroneum (sesamoid bone) at the level of the cuboid
Peroneus (Fibularis) Brevis (PB)
- Origin: distal 2/3 of fibula; muscle belly is lower than peroneus longus
- In the groove: lies anteromedial to PL (deeper, closer to fibula)
- Inserts on the base of 5th metatarsal (styloid process)
- Function: plantarflexion + eversion; lateral ankle stabilizer
- Clinically: avulsion at base of 5th metatarsal is a common injury ("dancer's fracture")
Peroneal Tubercle (Calcaneus)
- The peroneal tubercle on the lateral calcaneus separates the two peroneal tendons distally:
- PB passes above the peroneal tubercle
- PL passes below the peroneal tubercle
Superior Peroneal Retinaculum (SPR)
- Inserts anteriorly on periosteum of lateral malleolus; covers tendons posterolaterally; attaches to lateral calcaneus
- A small fibrocartilaginous ridge at the anterior margin of the groove acts like a labrum to deepen the groove
- SPR rupture → peroneal tendon subluxation/dislocation (snapping over lateral malleolus)
Accessory: Peroneus Quartus
- Present in 12–22% of the population
- Most common accessory ankle muscle
- Origin: distal 1/3 fibula → variable insertion (retrotrochlear eminence of calcaneus most common)
- Can cause crowding in the retromalleolar groove → peroneal tenosynovitis
3. Anterior Tendons
Held over the dorsum of the ankle and foot by the superior extensor retinaculum (transverse band just above ankle) and inferior extensor retinaculum (Y-shaped band with roots in the tarsal sinus).
From medial → lateral on the dorsum:
| Order (medial → lateral) | Tendon | Insertion | Function |
|---|---|---|---|
| 1st (most medial) | Tibialis anterior | Medial cuneiform + base of 1st metatarsal | Dorsiflexion + inversion |
| 2nd | Extensor hallucis longus (EHL) | Distal phalanx of great toe | Extension of hallux + dorsiflexion |
| 3rd | Extensor digitorum longus (EDL) | Distal phalanges of toes 2–5 | Extension of toes + dorsiflexion |
| 4th (most lateral) | Fibularis (peroneus) tertius | Base of 5th metatarsal | Dorsiflexion + eversion |
The dorsalis pedis artery lies on the dorsum between EHL and the EDL tendon to the 2nd toe — the surface landmark for pulse palpation.
Tibialis anterior is the largest anterior tendon and is visible/palpable medial to the ankle anterior to the medial malleolus on resisted dorsiflexion.
4. Posterior Tendons — Midline
Achilles (Calcaneal) Tendon
- Largest and strongest tendon in the body
- Formed by fusion of the gastrocnemius (two heads) and soleus aponeuroses = triceps surae
- The junction of the two aponeuroses is called the "conjoint junction"
- Fibers undergo a 90° internal rotation from proximal to distal (medial → posterior; lateral → anterior); this torsion increases mechanical resistance
- Inserts on the posterior surface of the calcaneus, below the posterosuperior angle
- No synovial sheath — instead surrounded by a paratenon (connective tissue derived from crural fascia)
- Retrocalcaneal bursa lies between tendon and posterosuperior calcaneal angle (clinically important in Haglund's deformity)
- Kager's fat pad fills the triangular space anterior to the tendon
- Poorest vascularization at the midportion (2–6 cm above insertion) → typical site of rupture and tendinopathy
- Tests S1–S2 reflex when tapped
Plantaris Tendon
- Long, slender tendon running medial to the Achilles tendon
- Inserts on the medial aspect of the calcaneus
- Absent in ~7–10% of people
- Clinically: rupture mimics Achilles injury; also used as a graft
Clinical Mnemonics
Tarsal Tunnel (medial, anterior to posterior):
"Tom, Dick, And Very Nervous Harry"
- Tibialis posterior
- Digitorum longus (FDL)
- Artery (posterior tibial)
- Veins (posterior tibial)
- Nerve (tibial nerve)
- Hallucis longus (FHL)
Posteromedial ankle surgical approach:
"Tom, Dick, and very angry nervous Harry" (Miller's Orthopaedics)
Clinical Significance Summary
| Tendon | Key Pathology |
|---|---|
| Tibialis posterior | Rupture → acquired flat foot (PTTD); most common medial tendon injury |
| FHL | Tenosynovitis in ballet dancers; trigger toe |
| Peroneus brevis | Avulsion at 5th metatarsal base; longitudinal tears at lateral malleolus |
| Peroneus longus | Os peroneum fracture; tear at cuboid tunnel |
| Peroneal tendons (both) | Subluxation/dislocation with SPR rupture |
| Tibialis anterior | Rupture (often in elderly) → foot drop on dorsiflexion |
| Achilles | Tendinopathy (midportion most common), rupture (typically 2–6 cm above insertion) |
— Gray's Anatomy for Students; Imaging Anatomy (Thieme), Vol. 3 — Bones, Joints, Vessels & Nerves; Rosen's Emergency Medicine, 10th ed.; Miller's Review of Orthopaedics, 9th ed.
This is a shared conversation. Sign in to Orris to start your own chat.