What is congenital trigger digits hand deformity
Reading File
Finding Sources
Searching the Web
congenital trigger digits hand deformity pathophysiology treatment
Searching PubMed
congenital trigger digit thumb finger
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a thorough answer. Here is the full, synthesized response:
Congenital / Pediatric Trigger Digits (Trigger Thumb & Trigger Finger)
Terminology and Classification
The term "congenital trigger digit" is now considered outdated. Current nomenclature uses pediatric trigger thumb and pediatric trigger finger, and these are no longer classified under congenital hand anomalies in the OMT (Oberg-Manske-Tonkin) classification, because evidence suggests they are likely acquired postnatally rather than truly congenital. Several large newborn screening studies found no cases at birth, despite the known incidence that would be expected if the condition were present from birth.
Trigger thumb is approximately 10 times more common than trigger finger in children.
Epidemiology
- Incidence: ~3 per 1,000 children diagnosed by age 1 year
- Males and females affected equally
- 25% of cases are bilateral
- More prevalent in Asian and Hispanic populations
- Possible genetic predisposition: autosomal dominant inheritance with variable penetrance has been reported; higher concordance in monozygotic twins
- Associated conditions (especially with trigger finger): trisomy 13, juvenile rheumatoid arthritis, mucopolysaccharidosis
Pathophysiology
Trigger Thumb
The core mechanism is a size mismatch between the flexor pollicis longus (FPL) tendon and its sheath, specifically at the level of the A1 pulley. This impairs normal tendon gliding.
Key features:
- Abnormal collagen degeneration and synovial proliferation cause the FPL tendon to thicken
- An intratendinous nodule called Notta's nodule forms proximal to the A1 pulley - it is palpable on clinical examination
- Biopsy consistently shows fibroblasts and mature collagen without inflammatory or degenerative changes, arguing against infectious or inflammatory etiology
- The tendon thickening prevents smooth passage through the A1 pulley, causing the characteristic locking in flexion
Trigger Finger (Less Common in Children)
The pathophysiology is more variable and less clearly defined than in adults or trigger thumb:
-
Abnormalities may extend from the A1 pulley up to the A3 pulley (broader involvement than in adults)
-
Abnormal nodularities in both the flexor digitorum superficialis (FDS) and profundus (FDP) tendons
-
Abnormal decussation between FDS and FDP tendons
-
Campbell's Operative Orthopaedics, 15th Ed., 2026, block42
Clinical Presentation
Trigger Thumb:
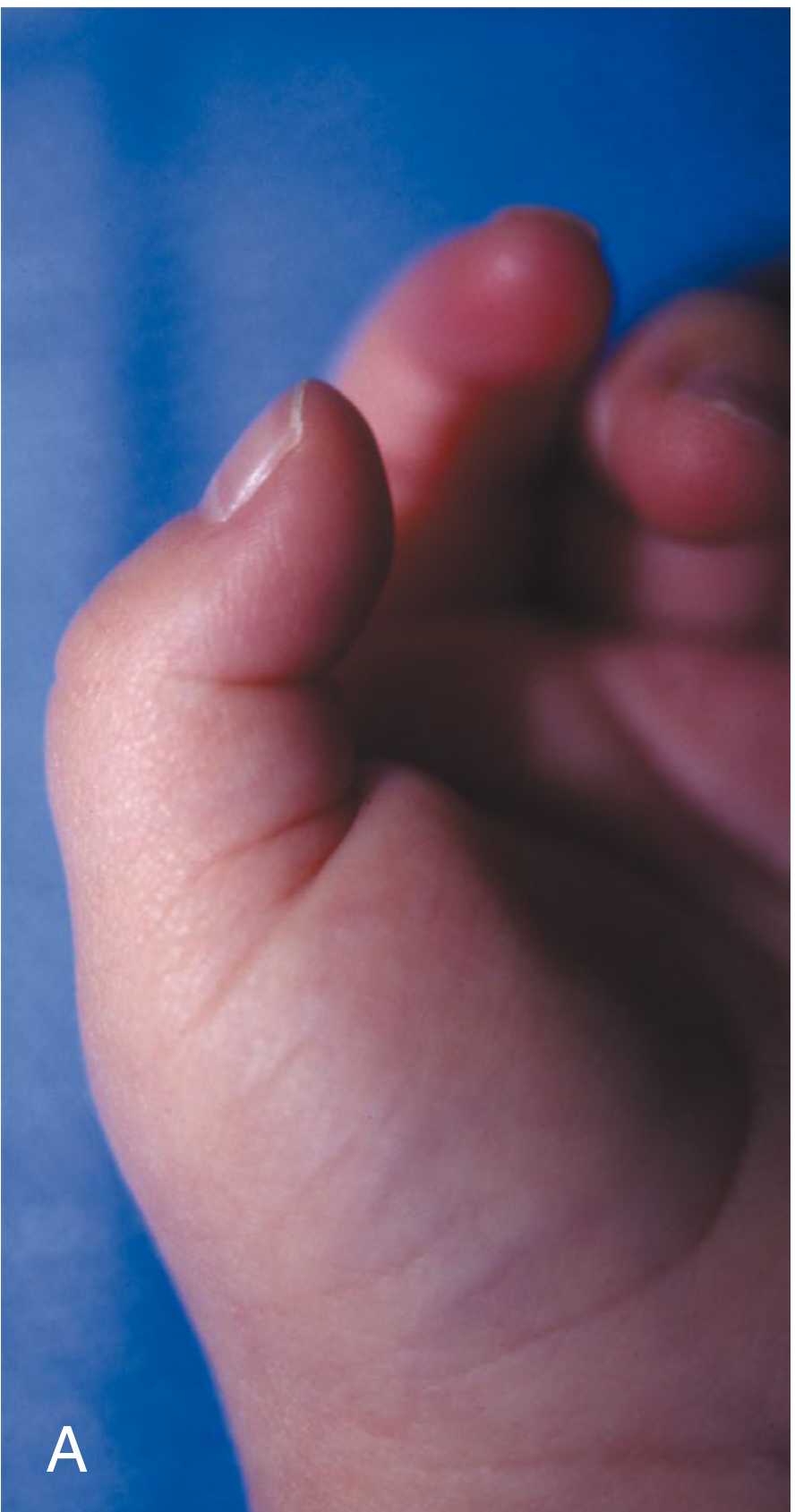
- Child presents in the first few years of life with a relatively fixed flexion posture of the interphalangeal (IP) joint of the thumb
- Even with passive force, full IP extension may be impossible
- The "snapping/clicking" sensation typical in adults is usually not the presenting complaint in children
- Notta's nodule may be palpable at the base of the thumb (volar side, proximal to the A1 pulley)
- Neurovascular status is typically preserved
Trigger Finger:
- Usually not noted until the patient is several years old
- Snapping sensation with active finger motion at the proximal interphalangeal (PIP) joint
- May present as a fixed flexion deformity
Key Differential: Must be distinguished from clasped thumb deformity, which involves primarily metacarpophalangeal (MCP) flexion with an abnormal extensor mechanism (EPB/EPL), whereas trigger thumb involves IP joint flexion with a normal extensor but abnormal flexor tendon.
Natural History
Resolution can occur spontaneously:
- One third to two thirds of trigger thumbs resolve without surgery
- Hutchinson et al.: 32% spontaneous resolution at 5 years; Baek et al.: 76% over 5 years
- Spontaneous resolution is more likely if the initial contracture is < 30 degrees
- Fixed contractures are unlikely if the condition resolves or is surgically corrected before age 3
- For trigger finger: 63% spontaneously resolve at an average age of 60.1 months
Treatment
Conservative (Non-operative)
- Observation alone has limited effectiveness
- Extension splinting (at least 3 hours/day) significantly improves outcomes over observation alone: 67% resolution with splinting vs. 30% with observation alone (Shiozawa et al.)
- More effective in early, flexible deformities where IP joint is not yet fixed
- Corticosteroid injections are used in adults but are generally not recommended in children
Surgical
Pediatric Trigger Thumb - A1 Pulley Release (Technique 85.43):
- Tourniquet control; transverse incision at the volar crease of the MCP joint of the thumb
- Carefully protect the two digital nerves
- Identify the prominent flexor sheath just beneath subcutaneous fat
- Identify the proximal edge of the A1 pulley and completely incise it longitudinally under direct vision
- Shaving the nodule or excising a segment of the A1 pulley is generally unnecessary
- Close wound; soft dressing; no particular immobilization required
- Traditionally recommended around age 3 if spontaneous resolution has not occurred
- Han et al.: excellent results even at an average age of 7.5 years, with return of near-normal motion by 2.7 weeks postoperatively
Pediatric Trigger Finger - More Extensile Release (Technique 85.44):
-
Bruner incision centered over the MCP joint and A1 pulley
-
Must visualize the flexor tendon sheath and tendons from the A1 to A3 pulley
-
Carefully evaluate for tendon nodularities and abnormal FDS/FDP decussation
-
Low threshold to resect a slip of FDS to reduce tendon volume within the sheath
-
Using A1 pulley release + FDS slip resection: 91% success rate (Bae, 23 patients)
-
Release A3 pulley if triggering persists
-
Campbell's Operative Orthopaedics, 15th Ed., 2026
Summary Table
| Feature | Trigger Thumb | Trigger Finger |
|---|---|---|
| Relative frequency | Much more common | ~10x less common |
| Affected joint | IP joint | PIP joint |
| Key pathology | FPL tendon/A1 pulley mismatch + Notta's nodule | A1-A3 pulley + FDS/FDP nodularity |
| Typical age at diagnosis | First few years of life | Several years old |
| Spontaneous resolution | 32-76% | ~63% |
| Surgical approach | A1 pulley release only | A1 to A3 release ± FDS slip resection |
Recent literature (2026): A clinical management update on pediatric trigger thumb (Gordon D, Sherman PJ. Curr Opin Pediatr, April 2026 [PMID: 41670430]) was published - this represents the most recent evidence on the topic and may contain updated management recommendations beyond the textbook.
What is meant about streeters dysplasia hand deformity
Finding Sources
Searching the Web
Streeter dysplasia constriction band syndrome hand deformity pathophysiology classification treatment
Searching PubMed
constriction band syndrome amniotic band upper limb
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive, textbook-quality answer. Here is the full response:
Streeter's Dysplasia (Constriction Ring Syndrome / Amniotic Band Syndrome)
What Is It?
Streeter's dysplasia is a widely used eponym for what is now formally called constriction ring sequence (also known as constriction band syndrome or amniotic band syndrome). The name honors George L. Streeter, who in 1930 described "focal deficiencies in fetal tissues and their relation to intrauterine amputation." The condition occurs when deep cutaneous creases encircle a limb or digit, as if a string were tightly tied around the part.
It comprises approximately 2% of all congenital hand anomalies, with distal rings and those involving the central digits being most common. Its incidence is approximately 1 in 1,200 live births.
Etiology and Pathophysiology
The exact cause remains debated. Two main theories exist:
-
Exogenous (Amniotic Band) Theory - Fibrous bands form from rupture or delamination of the amnion in utero, creating free-floating strands that wrap around and constrict developing fetal parts. This is the most widely accepted theory.
-
Endogenous (Vascular Disruption) Theory - Failure of development of subcutaneous tissue (similar to how normal skin creases form), or hemorrhages in the distal rays causing adhesions. Some argue these defects arise from vascular disruption rather than external bands.
Key facts:
-
Not inherited - there is no evidence of hereditary predisposition; it is a sporadic occurrence
-
Deformations occur later than 5-7 weeks of gestation (when most hand anomalies occur); the youngest fetus described had this anomaly at 10 weeks gestation
-
The condition is classified under the deformation category in the current OMT (Oberg-Manske-Tonkin) classification, not under malformations
-
Campbell's Operative Orthopaedics, 15th Ed., 2026; The Developing Human - Clinically Oriented Embryology
Types / Classification (Patterson Classification, 1961)
There are four basic types of constriction ring formation - these may occur in any combination in a single child:
| Type | Description |
|---|---|
| Type I | Simple constriction ring - usually transverse, occasionally oblique, around the limb or digit; no distal deformity |
| Type II | Deep ring with distal deformity - associated with lymphedema distal to the ring, with or without hypoplasia |
| Type III | Acrosyndactyly (fenestrated syndactyly) - lateral fusion of adjacent digits at their distal ends with proximal fenestrations (sinuses/channels) between the intervening skin and soft tissue |
| Type IV | Intrauterine amputation - soft tissues more affected than bone; bone may protrude (like a guillotine amputation); no rudimentary parts distally; a distinctive osseous spike may grow at the amputation stump; proximal limb is normally developed |
Clinical Features
Appearance of rings:
- Grooves vary in depth and circumference - sometimes appear as misplaced normal skin creases
- Shallow rings: skin often normal, but subcutaneous tissue is deficient beneath
- Deeper rings: superficial blood vessels crossing the ring are absent (deep vessels intact)
- With deep, unrelenting rings: progressive necrosis, scarring, and vascular impairment can occur
Distal effects:
- Lymphedema distal to the crease is frequent
- Cyanosis and worsening constriction can occur before surgical intervention
- Digits distal to rings may be shortened or completely amputated
- Terminal simple syndactyly with small fenestrations is common
Asymmetric distribution - deformations are typically asymmetric; thumbs and great toes are rarely involved; longer (central) digits are affected more than shorter digits
Associated Anomalies
Reported in 80% of patients:
- Syndactyly, hypoplasia, brachydactyly
- Symphalangism, symbrachydactyly, camptodactyly
Reported in 40-50% of patients:
- Clubfoot (talipes equinovarus)
- Cleft lip and/or cleft palate
- Cranial defects
Ulnar nerve palsy has also been reported in association with congenital ring syndrome.
Prenatal Diagnosis
- Prenatal ultrasound can detect ABS - visualization of amniotic bands attaching to the fetus, restriction of motion, constriction rings on extremities, and digital amputation with syndactyly are diagnostic features
- 3D and 4D ultrasound improve sensitivity of prenatal diagnosis
- MRI can provide more detailed characterization
Treatment
Conservative (Observation)
- Shallow, incomplete creases with no distal lymphedema - surgical intervention usually unnecessary except for cosmetic reasons
- Creases should be observed as "baby fat" is lost (may improve in appearance naturally)
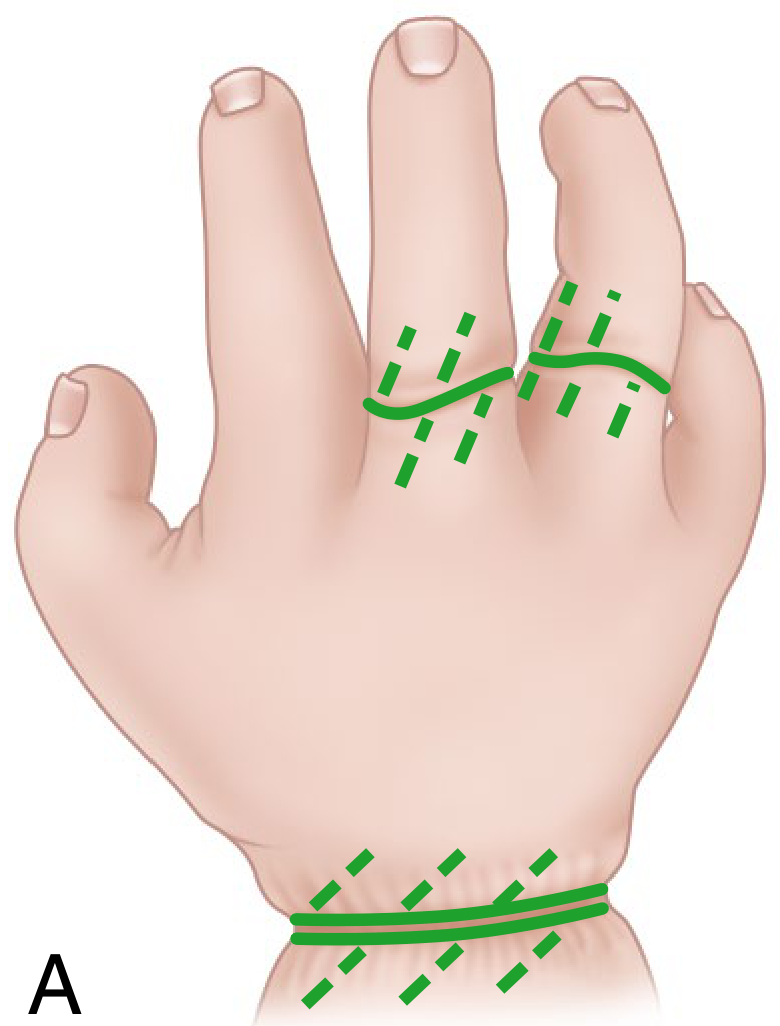
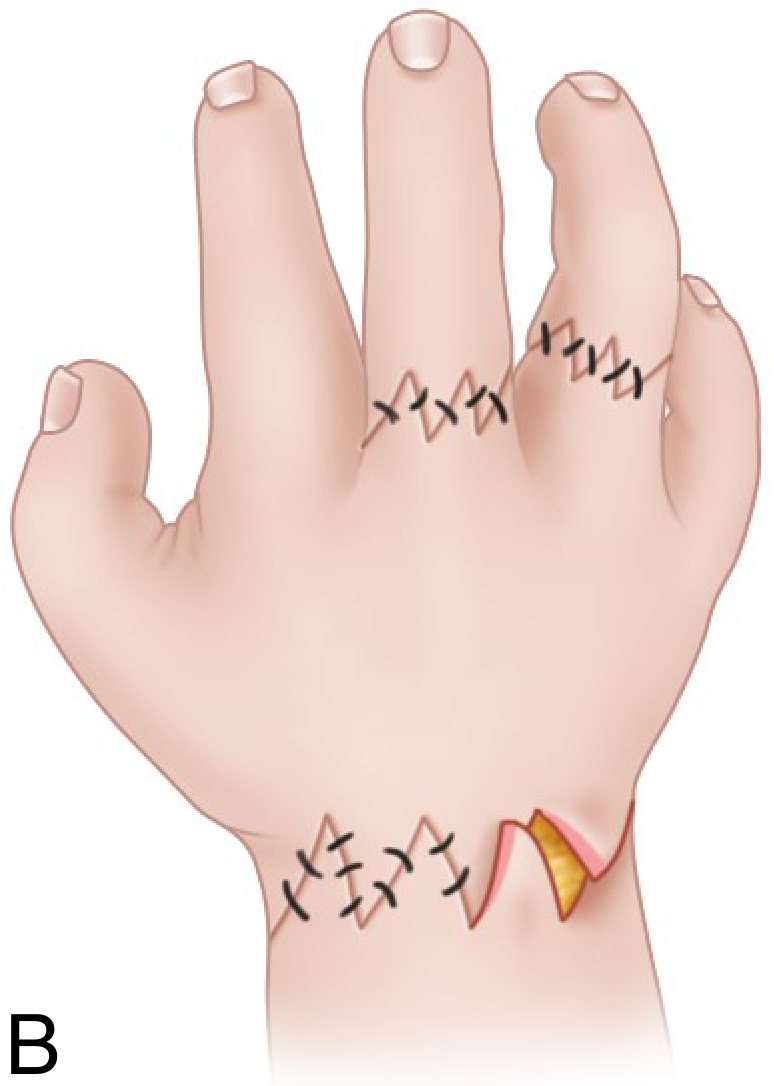
Surgical
For deep rings causing lymphedema or circulatory impairment:
- Excise down to normal tissue and close with multiple Z-plasty procedures
- If the ring completely encircles the part: staged excision is safer
- First operation: excise only one half (volar half) of the groove with Z-plasty closure
- Second operation: 2-3 months later to address the remaining half
- Splinting maintained for 2-3 weeks; sutures removed at 10-14 days
- Lymphedema and cyanosis typically improve gradually after release
- Simple excision with direct closure combined with limited Z-plasty is an alternative to traditional Z-plasty alone
For acrosyndactyly:
- Early syndactyly reconstruction is essential - all fingertips frequently are bound together, causing permanent deformity if not treated early
- Release of border digits (index and small finger) done within the first 6 months of life
- Release of central digits when the child is approximately 18 months old
- PIP joint stiffness is common after syndactyly release
For short digits:
- Lengthening by osteotomy and distraction
- Shortened thumb may require web space deepening or the Søiland method (adding a shortened index finger "on top" to lengthen the thumb)
Emergency surgery - indicated immediately in the neonatal period if the constriction ring is jeopardizing digital circulation (can be done under local anesthesia in the NICU)
Summary
| Feature | Detail |
|---|---|
| Eponym origin | G.L. Streeter, 1930 |
| Current name | Constriction ring sequence |
| Incidence | ~1 in 1,200 live births |
| Inheritance | Sporadic; non-hereditary |
| Timing of onset | After 10 weeks gestation |
| Four types | Simple ring, ring + distal deformity, acrosyndactyly, intrauterine amputation |
| Key associated anomaly | Clubfoot (40-50%), syndactyly/hypoplasia (80%) |
| Main surgical treatment | Staged Z-plasty ring excision; early acrosyndactyly release |
- Campbell's Operative Orthopaedics, 15th Ed., 2026; Miller's Review of Orthopaedics, 9th Ed.; The Developing Human - Clinically Oriented Embryology
What is cleft hand deformity ?
Finding Sources
Searching the Web
cleft hand deformity ectrodactyly classification pathophysiology surgical treatment
Searching PubMed
cleft hand ectrodactyly congenital
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have comprehensive information from Campbell's Operative Orthopaedics (2026) and supporting sources to compose a thorough answer.
Cleft Hand Deformity (Ectrodactyly / Central Longitudinal Deficiency)
Definition and Names
Cleft hand is a congenital longitudinal deficiency of the central rays of the hand, characterized by the absence or severe suppression of bone and soft tissues of the second, third (long), and/or fourth rays (index, middle, ring fingers). This produces a cleft - a gap or split - in the center of the hand.
Common names include:
- Ectrodactyly (Greek: "ektroma" = abortion + "daktylos" = finger)
- Split-hand malformation
- Lobster claw hand
- Crab claw hand
- Central longitudinal deficiency (ICD-10: Q68.1)
It is exceedingly rare, with an incidence of approximately 1 per 90,000 live births (some sources cite 1 in 20,000).
Clinical Appearance


Types: Typical vs. Atypical
| Feature | Typical Cleft Hand | Atypical Cleft Hand |
|---|---|---|
| Shape of cleft | V-shaped (narrow, pointed) | U-shaped (wide, shallow) |
| Digits absent | Long finger (3rd ray); occasionally index | Index, long, and ring (central 3 rays) |
| Remaining digits | Two digits on each side of cleft with syndactyly | Only thumb (radial) + little finger (ulnar) |
| First web space | Often narrow/deficient | Usually in the same plane |
| Laterality | Bilateral | Unilateral |
| Foot involvement | Bilateral foot deformities common | No associated foot deformity |
| Underlying entity | True central ray deficiency | Actually a form of symbrachydactyly |
| Inheritance | Autosomal dominant, incomplete penetrance | Sporadic |
Pathophysiology
The etiology of cleft hand is not fully established. Key concepts:
-
Apical Ectodermal Ridge (AER) defect - A wedge-shaped defect in the apical ectodermal ridge of the limb bud during the 5th-6th week of development prevents normal central digital ray formation. This distinguishes cleft hand from symbrachydactyly, which results from primary failure of the underlying bone (hence symbrachydactyly retains small terminal remnants, while pure cleft hand does not).
-
Centripetal suppression theory (Maisels) - Milder deformities have only a simple cleft without significant tissue loss; as severity increases, central ray is lost first, followed by loss of radial rays, and eventually all rays.
-
Association with central polydactyly - Cleft hand and central polydactyly can co-exist, emphasizing the developmental complexity. A rare ulnar-sided cleft hand has also been described (clefting between ring and small, or long and small fingers).
-
Genetics:
- Most typical cleft hands: autosomal dominant, incomplete penetrance
- Split-hand/split-foot (SHSF) syndrome: autosomal dominant, ~70% penetrance
- Many cases are sporadic
- Associated gene loci: 7q21 (DLX5/DLX6 region), 10q24, 2q31
Classification
Manske and Halikis Classification (most widely used clinically)
Based on first web space status (thumb-index web):
| Type | First Web Space | Description |
|---|---|---|
| I | Normal | Normal thumb web; cleft in central rays only |
| II | Narrowed | Mild narrowing of thumb-index web |
| IIIA | Syndactylized | Syndactyly of index and thumb with suppressed long finger |
| IIIB | Syndactylized | Thumb/index syndactyly with absent long finger |
| IV | Merged | Index suppressed; first web merged with cleft |
| V | Absent | Thumb absent; five-fingered hand appearance |
OMT Numerical Classification
- Group 0: All central bones present
- Group 1: One ray involved
- Group 2: Two rays involved
- Group 3: Three rays involved Each group is further divided into subgroups by degree of finger involvement.
Radiographic Features
- Transversely oriented bones (delta metacarpals) may be present within the cleft - these will progressively widen the cleft with growth if not removed
- Delta phalanx may be seen
- Two metacarpals supporting one digit, or a split metacarpal supporting two digits
- Metacarpal/phalangeal divergence angle between index and ring fingers should be measured for surgical planning
- Carpal coalition present in older children
Associated Anomalies
Reported in association with central hand deficiencies (Box 85.4):
Other limb/musculoskeletal:
- Cleft foot (split-foot)
- Clubfoot, calcaneovalgus, cavovarus foot
- Bilateral absence of the tibia
- Bilateral hip dislocation, short femur, hypoplastic patella
- Short humerus, absent ulna, radioulnar synostosis, elbow synostosis
Head/facial:
- Cleft lip/palate
- Deviated nasal septum
- Congenital ptosis, cataracts
Other systems:
- Congenital heart disease
- Imperforate anus
- Deafness
- Anonychia (absent nails)
- Genitourinary anomalies
- Hypoplasia or pseudoarthrosis of the clavicle, absent pectoralis major
Key syndromes:
- Split-Hand/Split-Foot (SHSF) syndrome - most common; autosomal dominant
- EEC syndrome - Ectrodactyly + Ectodermal Dysplasia + Cleft lip/palate
- Cornelia de Lange syndrome, Fanconi pancytopenia
Function
Despite the striking appearance, children with cleft hand often develop remarkable dexterity and adaptive function. The pincer grip between border digits can be highly effective, especially in typical bilateral cleft hand. Surgeons and families must appreciate that the appearance is far worse than the functional deficit.
Treatment
Non-operative
- No effective conservative management exists
- Prostheses have largely been abandoned - even severe bilateral deformities allow significant adaptive function, and prostheses are used only occasionally for cosmesis on request
Indications for Surgery
- Cleft closure (cosmesis and function)
- Syndactyly release (especially between digits of unequal length)
- Narrowed first web space - the most important functional indication
- Transverse/deforming bony elements - these will progressively widen the cleft during growth; must be removed
- Absent or hypoplastic thumb reconstruction
- Delta phalanx correction
Goals of Surgery
- Primary: Achieve good pinch and grasp
- Secondary: Acceptable cosmesis
- Surgery should maintain or improve function; never sacrifice function for appearance
Timing and Sequence
- Syndactyly release - border digits first (by 6 months of age), central digits by 18 months
- After 6-month recovery: cleft closure alone, or cleft closure combined with first web deepening
- For cleft closure with first web deepening: the index metacarpal can be transferred to the long metacarpal position
Key Surgical Techniques
- Snow-Littler procedure - classic technique for cleft closure with first web space deepening
- Miura and Komada technique - less technically demanding, comparable results, fewer complications; 20-year follow-up shows long-term functional success
- Ueba technique - for palmar cleft with absent long finger, especially when combined with narrow thumb web
- Upton-Taghinia technique - simple incision separating glabrous from dorsal skin; avoids complicated dorsal/volar flaps and risk of flap necrosis
- Bipedicle flap/tunneling - index finger tunneled under a bipedicle flap of cleft skin to widen the first web space; good blood supply, no scar within the new web space
- Bony removal - transverse bones blocking cleft closure removed sparingly (excess removal weakens palm and risks cleft recurrence)
For the Atypical Pattern (Symbrachydactyly type)
- Deepening of palm for grasp
- Osteotomies of metacarpals for better opposition
- Tendon transfers for hypoplastic digits
- Single-stage toe-to-hand transfer for the one-digit hand (occasionally)
Worse outcomes associated with:
- Preoperative first web space narrowing
- Postoperative index MCP joint abnormalities
Sources: Campbell's Operative Orthopaedics, 15th Ed. (2026); The Developing Human - Clinically Oriented Embryology; StatPearls - Cleft Hand (2023)
What is madelung deformity
Finding Sources
Searching the Web
Madelung deformity wrist pathophysiology classification surgical treatment
Searching PubMed
Madelung deformity wrist treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Finding Sources
I now have all the key information - the treatment algorithm is particularly valuable. I have comprehensive content from Campbell's Operative Orthopaedics (2026), Grainger & Allison's Diagnostic Radiology, and supporting sources. Here is the full answer:
Madelung Deformity
Definition and History
Madelung deformity is an abnormality of the volar-ulnar part of the distal radial physis in which progressive ulnar and volar tilt develops at the distal radial articular surface, with dorsal subluxation of the distal ulna. The condition was first described by Malgaigne in 1855 and more fully characterized by Otto Madelung in 1878.
It is a rare congenital disorder accounting for approximately 2% of congenital hand anomalies, though it seldom becomes obvious until late childhood or adolescence.
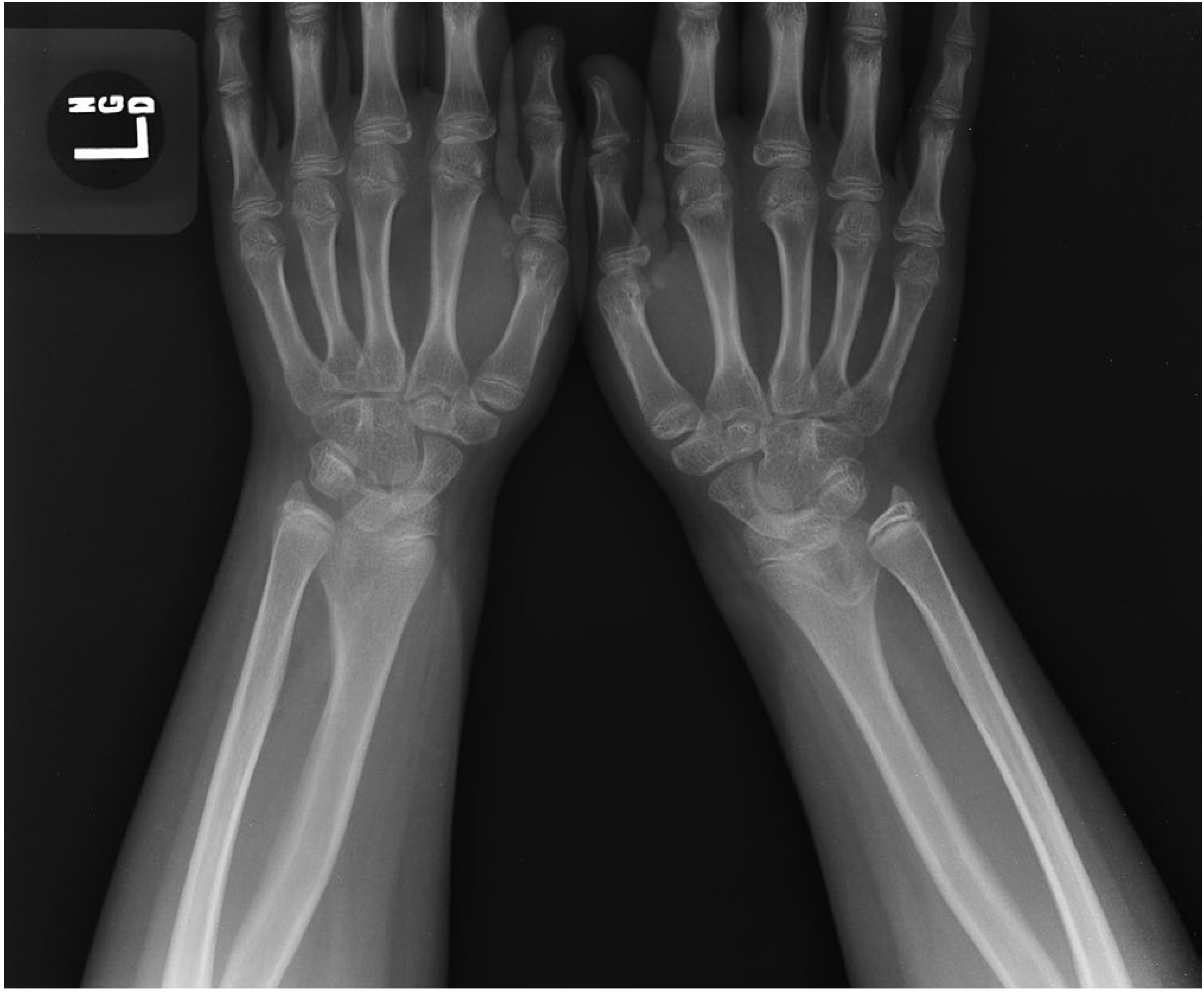
X-Ray Appearance
Pathophysiology
The Core Mechanism
Premature partial fusion (growth arrest) of the volar-ulnar aspect of the distal radial physis causes asymmetric radial growth. The dorsal-radial portion of the physis continues to grow normally, while the volar-ulnar portion cannot. This produces:
- Volar and ulnar bowing of the radius
- Increased radial inclination (ulnar tilt of the articular surface)
- Volar tilt of the lunate facet and scaphoid facet
- The ulna continues to grow straight - leading to dorsal prominence of the distal ulnar head
- Triangulation of the carpus - the lunate migrates proximally into the widened gap between radius and ulna
Role of the Vickers Ligament
In 83% of cases (Farr's study of 75 extremities), an anomalous volar ligament called the Vickers ligament is present. This ligament:
- Tethers the lunate to the distal radius proximal to the physis
- Acts as a physical tether that impedes growth of the volar-ulnar physis
- Is the primary deforming force in most cases
- A second anomalous radiotriquetral ligament has also recently been identified in many cases
Timing
Growth arrest occurs after 5-7 weeks of gestation (unlike most hand malformations). The deformity typically manifests clinically in late childhood or early adolescence.
Demographics and Associations
- Female predominance: affects girls 4 times more than boys
- Usually bilateral (bilateral deformities are often more severe at presentation)
- If bilateral deformity + short stature: suspect Leri-Weill dyschondrosteosis
- Family history often present
Etiology and Classification (Vender & Watson)
| Type | Cause |
|---|---|
| Posttraumatic | Damage to distal radial physis (Salter-Harris fracture, gymnast's wrist, repetitive stress) |
| Dysplastic | Dyschondrosteosis (Leri-Weill), diaphyseal aclasia |
| Genetic | Turner syndrome, SHOX mutations |
| Idiopathic | No identifiable cause |
Acquired (posttraumatic/infectious) deformities are distinguished by: unilaterality, less severe carpal deformity, absence of family history, and appropriate injury history.
Other conditions producing Madelung-like deformity:
- Mucopolysaccharidosis
- Turner syndrome
- Achondroplasia
- Multiple hereditary exostoses
- Multiple epiphyseal dysplasia
- Ollier disease (dyschondroplasia)
- Prior infection or juvenile chronic arthritis
Genetics: SHOX Gene
Leri-Weill dyschondrosteosis (the most common form of mesomelic dwarfism) is the classic genetic association:
- Mild short stature
- Shortness of the middle segments of upper and lower extremities (mesomelia)
- Madelung deformity
Caused by mutations in the SHOX homeobox gene (Short stature HOmeoboX gene), located at the pseudoautosomal region 1 (PAR1) of both the X and Y chromosomes. This is also why it is seen in Turner syndrome (45,X - only one X chromosome, missing one PAR1 copy).
Clinical Features
- Deformity usually manifests in late childhood or early adolescence
- Decreased wrist motion (particularly wrist extension and supination)
- Minimal to moderate pain - from ulnocarpal impingement
- Prominent dorsal distal ulna (bayonet deformity appearance)
- Volar displacement of the hand relative to the forearm
- As growth occurs, the deformity worsens in appearance
Radiographic Findings (Table 85.8)
| Structure | Finding |
|---|---|
| Radius | Curved with convexity dorsal and radial; similar angulation of articular surface; "flame-shaped" notch at ulnar metaphysis (indicates Vickers ligament - can be confirmed on MRI) |
| Distal radial epiphysis | Triangular - due to failure of growth in ulnar and volar aspects; early physis closure |
| Forearm | Relatively short |
| Ulna | Dorsal and distal prominence; positive ulnar variance |
| Carpus | Triangular configuration; proximal migration of the lunate; reduced carpal angle; wedging of carpal bones between radius and ulna |
Advanced imaging: 3D CT is increasingly used for surgical planning in complex cases. MRI can confirm the Vickers ligament.
Treatment
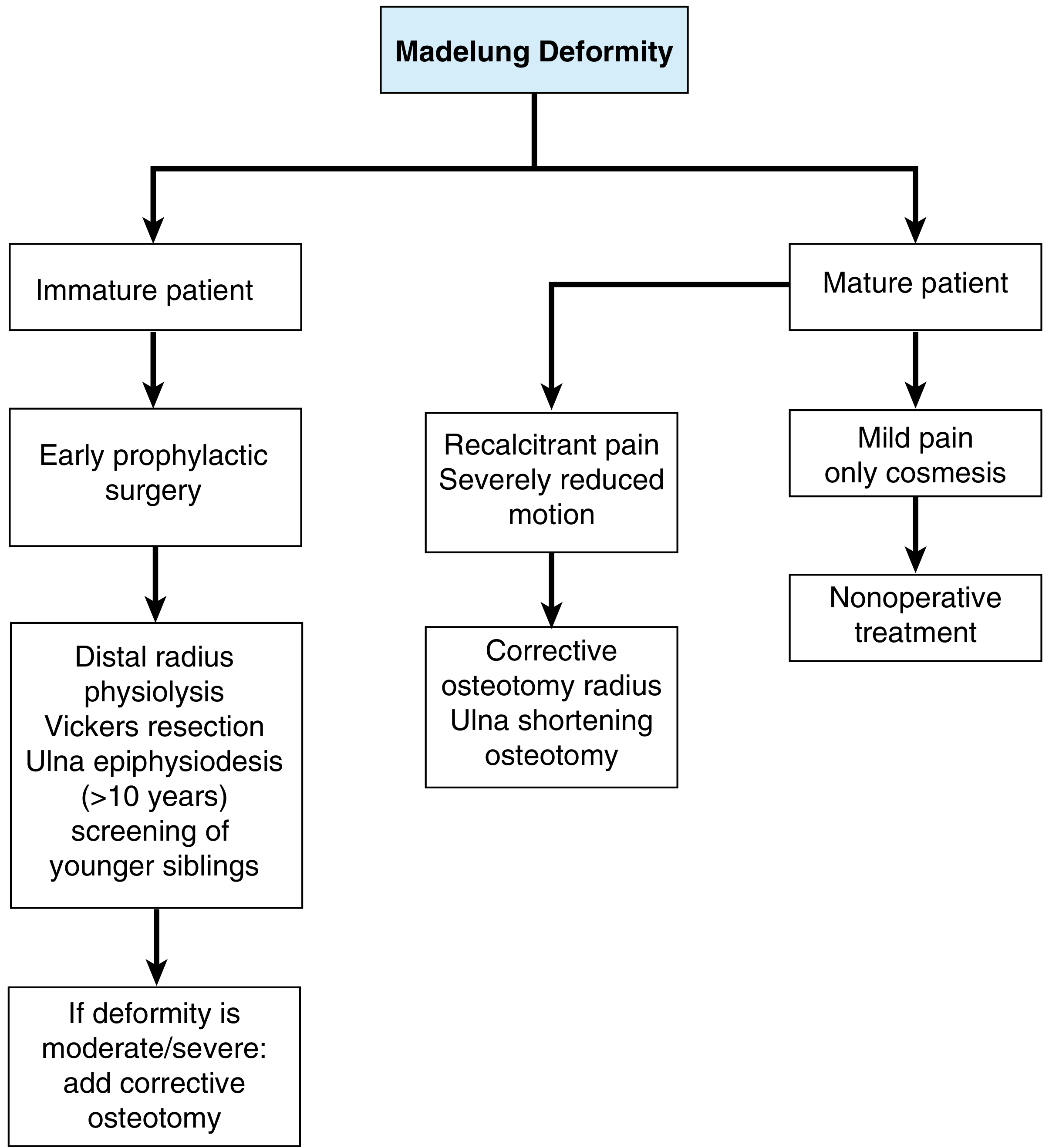
Conservative (Non-operative)
- Indicated for: mild symptoms, mature patient with cosmetic concerns only
- Oral NSAIDs, activity modification, wrist splinting
- Serial radiographs every 6 months until skeletal maturity
- Most children have minimal pain and excellent function - non-operative approach is warranted initially
Surgical Treatment
In Skeletally IMMATURE Patients
1. Physiolysis + Vickers Ligament Release (Langenskiöld / Vickers-Nielsen procedure)
- First-line for young patients with growth remaining
- The anomalous Vickers ligament is released from its radial attachment
- Combined with physeal bar resection and fat interposition to allow the physis to resume growth
- Guided growth (hemiepiphysiodesis) can augment the procedure
- Technique (Vickers-Nielsen):
- Volar transverse incision 1.5 cm proximal to the wrist crease
- Protect median nerve and radial artery
- Approach radial to the flexor tendons to the pronator quadratus
- Longitudinal osteotomy in the radius ~5 mm from the radioulnar joint
- Reflect the small volar-ulnar radial fragment ulnarward
- Identify and excise the physeal bar; interpose fat
- Release the Vickers ligament from its radial attachment
2. Distal Radial Osteotomy + Ulnar Shortening (Milch recession)
- Preferred for immature patients with moderate to severe existing deformity
- Radial osteotomy can be closing or opening wedge as needed
- Dome osteotomy: provides better volar coverage of the lunate and corrects positive ulnar variance; combined with Vickers ligament release gives best long-term results
3. Ulnar Epiphysiodesis
- For patients over age 10 years
- Prevents progressive ulnar overgrowth and may avoid later ulnar shortening
Carter & Ezaki series (23 wrists): Vickers ligament present in 91%; dome osteotomy used in 16 wrists and relieved pain in all; 25-year follow-up showed maintained correction and good-to-excellent functional results.
In Skeletally MATURE Patients
For recalcitrant pain or severely reduced motion:
- Distal radius corrective osteotomy (dome or wedge) + ulnar shortening osteotomy
- Darrach procedure (distal ulnar head resection) - with radial osteotomy
- Sauvé-Kapandji procedure - DRUJ arthrodesis with a proximal ulnar osteotomy (creates a pseudarthrosis above the fusion)
- Watson balanced radial osteotomies with matched ulnar resection - preserves radial length
- Radial osteotomy with callus distraction using external fixator (for severe cases)
- Radioscapholunate arthrodesis with neo-DRUJ - for severely abnormal sigmoid notch (experimental)
- Distal radioulnar arthroplasty
For mild pain or cosmetic concerns only in the mature patient: non-operative treatment.
Summary
| Feature | Detail |
|---|---|
| Eponym | Otto Madelung, 1878 |
| Primary defect | Volar-ulnar distal radial physeal growth arrest |
| Key structure | Vickers ligament (present in 83%) |
| Deformity triad | Volar-ulnar radial bowing + dorsal ulna prominence + triangular carpus |
| Sex | Females 4x more affected |
| Laterality | Usually bilateral |
| Key association | Leri-Weill dyschondrosteosis (SHOX gene mutation) |
| Gold-standard early surgery | Physiolysis + Vickers ligament release |
| Mature patient surgery | Corrective osteotomy ± Darrach / Sauvé-Kapandji |
- Campbell's Operative Orthopaedics, 15th Ed. (2026); Grainger & Allison's Diagnostic Radiology
- Most recent review: Madelung Deformity: A Current Concepts Review (Taleghani et al., J Hand Surg Am, Feb 2026 - PMID: 41686103)
This is a shared conversation. Sign in to Orris to start your own chat.