Biological effects of radiation
Reading File
Finding Sources
Searching the Web
biological effects of radiation ionizing mechanisms tissue damage
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile a thorough, well-organized answer.
Biological Effects of Radiation
Ionizing radiation interacts with living tissue by ejecting electrons from atoms, initiating a cascade of chemical and biological damage. The effects are broadly classified by timing (acute vs. chronic), mechanism (direct vs. indirect), target (somatic vs. genetic), and dose-response relationship (deterministic vs. stochastic).
1. Mechanisms of Damage
Direct Effects
Radiation directly strikes DNA or other macromolecules, causing single-strand breaks (SSBs) or double-strand breaks (DSBs) in DNA. DSBs are the most biologically significant lesion.
Indirect Effects
More commonly, radiation ionizes water molecules in cells, producing highly reactive free radicals (especially hydroxyl radicals, OH•). These free radicals then attack DNA, proteins, and lipids - causing widespread cellular injury at doses too low to produce direct hits.
- ROSEN's Emergency Medicine: "Direct effects include single- and double-strand DNA breaks. Indirect effects act through generation of free radicals that then attack other molecules in the cell."
2. Somatic vs. Genetic Effects
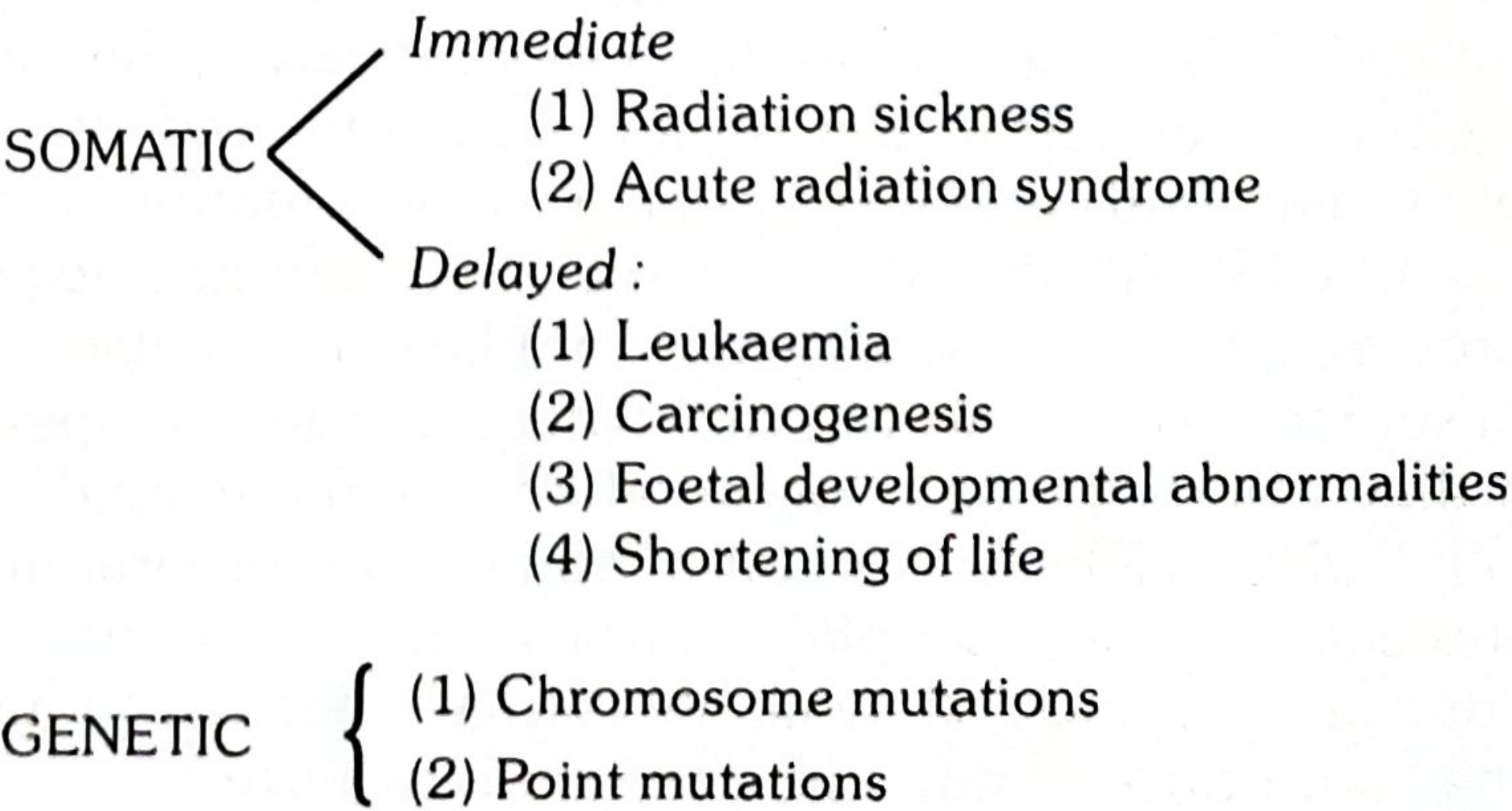
Somatic Effects (in the irradiated individual)
Immediate:
- Radiation sickness
- Acute Radiation Syndrome (ARS)
Delayed:
- Leukaemia
- Carcinogenesis (solid tumors)
- Foetal developmental abnormalities
- Shortening of life
Genetic Effects (in offspring)
Occur when radiation damages germ cells (eggs/sperm):
-
Chromosome mutations - associated with sterility
-
Point mutations - affect individual genes and can be passed to future generations
-
Park's Textbook of Preventive and Social Medicine: "While somatic effects are recognizable within the life span of the irradiated person, genetic effects would be manifest in the more or less remote offspring."
3. Deterministic vs. Stochastic Effects
| Feature | Deterministic | Stochastic |
|---|---|---|
| Dose-response | Severity increases with dose | Probability increases with dose (not severity) |
| Threshold | Yes (effects appear above a threshold) | No safe threshold assumed |
| Examples | Bone marrow suppression, cataracts, skin erythema, organ damage | Cancer, heritable genetic mutations |
- ROSEN's Emergency Medicine: "Deterministic effects are those in which the severity of injury is a function of dose... Stochastic or probabilistic effects are those in which the probability of an effect, rather than its severity, is a function of dose."
Organ-Specific Deterministic Late Effects (after high-dose radiotherapy)
| Organ | Local Effect | Systemic Effect |
|---|---|---|
| Brain/cranial nerves | Focal weakness, vision loss | Neurocognitive deficit |
| Lung | Bronchial stricture | Shortness of breath |
| Heart | Coronary stenosis | Pericarditis, cardiomyopathy |
| Bladder | Bleeding | Urinary frequency |
| Bowel | Ischemia, bleeding | Enteritis |
(Goldman-Cecil Medicine)
4. Cellular Radiosensitivity
Cells are not equally sensitive to radiation. The most radiosensitive cells are those that:
- Divide rapidly
- Are undifferentiated
- Have high metabolic activity
Most radiosensitive (Law of Bergonie and Tribondeau):
- Bone marrow stem cells
- Lymphocytes
- Spermatogonia
- Ovarian follicle cells
- Intestinal crypt cells
- Epidermal basal cells
Least radiosensitive:
- Connective tissue cells
- Central nervous system neurons (minimal cell turnover)
5. Acute Radiation Syndrome (ARS)
ARS occurs after whole-body or large partial-body exposure above a threshold dose. Three distinct syndromes occur in sequence with increasing dose:
| Dose (Gray) | Syndrome | Outcome |
|---|---|---|
| ~1-6 Gy | Hematopoietic syndrome | LD 50/60 ~6 Gy without treatment; bone marrow failure |
| ~6-10 Gy | Gastrointestinal syndrome | Destruction of GI mucosa; near-certain death |
| >10-12 Gy | Neurovascular (cerebrovascular) syndrome | Multiple organ failure; death within days |
Dose-response summary (in rad):
| Dose | Effect |
|---|---|
| < 5 rad | No immediate observable effects |
| 5-50 rad | Slight blood changes detectable on testing |
| 50-150 rad | Blood changes + nausea, fatigue, vomiting |
| 150-1,100 rad | Severe blood changes; ~50% mortality at 300-500 rad within 60 days (hematopoietic syndrome) |
| 1,100-2,000 rad | GI syndrome; 100% mortality within 1-2 weeks |
| >2,000 rad | CNS syndrome; death is certain, often within hours |
6. Radiation Carcinogenesis (Stochastic)
Radiation acts primarily as a multiplier of natural cancer rates. Most radiation-induced cancers appear many years later, typically in the usual "cancer-prone" years (55-75 years).
Key exceptions (earlier onset):
- Hematopoietic cancers (leukemia) - appear within a few years
- Thyroid cancer - appears within a few years
Risk data from atomic bomb survivors (Goldman-Cecil Medicine):
- At 1 Gy dose: 64% increased risk of solid cancer in females; 20% increase in males (at 50+ year follow-up)
- Hereditary effects in children of survivors were NOT detected despite extensive study
Age matters: People exposed at younger ages carry higher lifetime cancer risks.
7. Special Considerations
Fetal Exposure
Fetal tissue is extremely radiosensitive. In utero exposure can cause:
- Growth retardation
- Organ malformations
- Microcephaly (especially 8-15 weeks gestation)
- Increased lifetime cancer risk
Internal vs. External Exposure
For internal contamination (ingested/inhaled radionuclides):
- The effective half-life determines duration of exposure: 1/effective t½ = 1/biologic t½ + 1/physical t½
- Example: Iodine-131 has a physical half-life of ~8 days and a biologic half-life of ~57 days
Linear Energy Transfer (LET)
The quality factor (Q) reflects how densely ionizing a radiation type is:
- X-rays, gamma rays, electrons: Q = 1
- Alpha particles: Q = 20 (far more biologically damaging per unit energy)
8. Radiation Protection
- Natural background radiation: ~0.1 rad/year (no significant hazard at this level)
- ICRP-recommended limit from man-made sources: 5 rad/year for workers
- Genetic dose limit: no more than 5 rems over 30 years for the whole population
- Protective measures: lead shielding (0.5 mm lead apron reduces scattered X-rays by >90%), film badges/dosimeters, minimizing unnecessary exposures
Sources:
- Park's Textbook of Preventive and Social Medicine (p. 846)
- Goldman-Cecil Medicine, International Edition
- ROSEN's Emergency Medicine: Concepts and Clinical Practice (p. 2847)
- NCBI: Mechanisms of Biological Effects - Ionizing Radiation
This is a shared conversation. Sign in to Orris to start your own chat.