Explain me 10 comman heart disease with ECG changes and Ecg images of those disease
Reading File
Finding Sources
Searching the Web
10 common heart diseases ECG changes electrocardiogram findings with images
Finding Sources
Finding Sources
Searching the Web
ECG images STEMI atrial fibrillation heart block ventricular tachycardia WPW hypertrophic cardiomyopathy
Finding Sources
Finding Sources
Searching the Web
ECG examples STEMI heart failure pericarditis cardiac tamponade long QT syndrome site:ecgwaves.com OR site:litfl.com
Loading Image
Loading Image
Searching the Web
ECG STEMI inferior anterior atrial fibrillation ventricular tachycardia complete heart block images site:litfl.com OR site:ecgwaves.com
Reading Web Page
https://litfl.com/inferior-stemi-ecg-library
I now have comprehensive information from authoritative sources. Let me compile the full, detailed response with ECG images.
10 Common Heart Diseases: ECG Changes & Images
Below is a clinical overview of 10 common cardiac conditions, their characteristic ECG changes, and illustrative ECG images from authoritative sources.
1. ST-Elevation Myocardial Infarction (STEMI)
Pathophysiology: Complete occlusion of a coronary artery causing full-thickness (transmural) myocardial ischemia/necrosis.
ECG Changes:
- ST elevation ≥ 1 mm in two or more contiguous leads (convex/tombstone morphology)
- Reciprocal ST depression in opposite leads (very characteristic)
- Hyperacute T waves - tall, peaked T waves in the earliest phase
- Pathological Q waves develop after infarction (>40 ms wide, >25% of R wave height)
- T-wave inversions evolve over hours-days
- Lead localization: Inferior STEMI = II, III, aVF | Anterior STEMI = V1-V4 | Lateral STEMI = I, aVL, V5-V6
ECG Image - Inferior STEMI:
 (Source: LITFL ECG Library - ST elevations in leads II, III, aVF with reciprocal changes in aVL)
(Source: LITFL ECG Library - ST elevations in leads II, III, aVF with reciprocal changes in aVL)
2. Atrial Fibrillation (AF)
Pathophysiology: Disorganized atrial electrical activity with multiple re-entrant circuits, causing chaotic atrial depolarization. Most common sustained arrhythmia (lifetime risk ~25% over age 40).
ECG Changes:
- Absent P waves - replaced by fine, irregular fibrillatory baseline (f-waves)
- Irregularly irregular RR intervals - the hallmark
- Narrow QRS (unless aberrant conduction or bundle branch block)
- Ventricular rate varies: rapid (~100-160 bpm in uncontrolled AF), normal, or slow
ECG Image - Atrial Fibrillation:
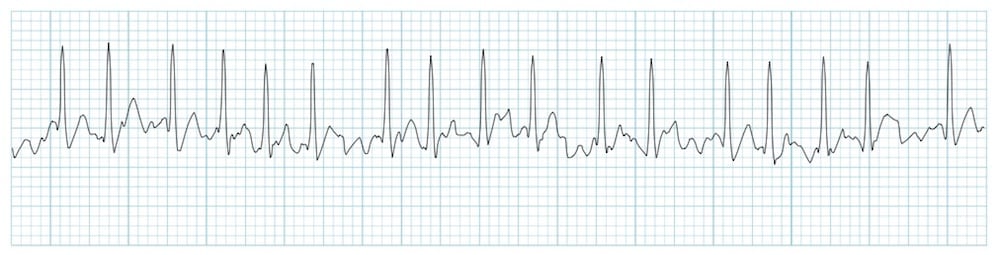 (Source: LITFL ECG Library - Atrial Fibrillation - Note absent P waves, irregular baseline, irregularly irregular QRS complexes)
(Source: LITFL ECG Library - Atrial Fibrillation - Note absent P waves, irregular baseline, irregularly irregular QRS complexes)
3. Ventricular Tachycardia (VT)
Pathophysiology: Rapid, organized rhythm originating from ventricular myocardium or Purkinje fibers, usually in the context of structural heart disease (post-MI scar, cardiomyopathy).
ECG Changes:
- Wide QRS complexes (≥ 120 ms), often bizarre morphology
- Rate 100-250 bpm, usually regular
- AV dissociation - P waves marching through at a slower independent rate (pathognomonic when visible)
- Capture beats and fusion beats (Dressler beats) - hallmark features
- Concordance in precordial leads (all positive or all negative)
- Left axis deviation (usually)
ECG Image - Ventricular Tachycardia:
 (Source: LITFL ECG Library - Regular wide complex tachycardia)
(Source: LITFL ECG Library - Regular wide complex tachycardia)
4. Complete (Third-Degree) AV Block
Pathophysiology: Complete interruption of conduction between atria and ventricles. The atria and ventricles beat independently. Often caused by inferior MI (RCA territory), fibrosis, or drugs.
ECG Changes:
- Complete AV dissociation - P waves and QRS have no fixed relationship
- P waves march at a faster rate than QRS complexes (atrial rate > ventricular rate)
- Escape rhythm is slow: junctional escape (40-60 bpm, narrow QRS) or ventricular escape (20-40 bpm, wide QRS)
- PR interval varies randomly
- First-degree AV block: PR > 200 ms only
- Mobitz II: sudden dropped beats without PR lengthening (most dangerous 2nd degree type)
ECG Image - Complete Heart Block:
 (Source: LITFL ECG Library - P waves (arrows) dissociated from slow wide QRS escape rhythm)
(Source: LITFL ECG Library - P waves (arrows) dissociated from slow wide QRS escape rhythm)
5. Acute Pericarditis
Pathophysiology: Inflammation of the pericardium, typically viral. ECG changes reflect subepicardial myocardial irritation rather than transmural ischemia.
ECG Changes (4 classic stages):
- Stage 1 (hours-days): Diffuse concave-up ST elevation in nearly all leads (except aVR and V1) + PR segment depression (best in leads II, V6), with PR elevation in aVR
- Stage 2 (within 1 week): ST and PR return to baseline, T-wave flattening
- Stage 3: Diffuse T-wave inversions after ST normalizes
- Stage 4: ECG normalization (may take weeks)
Key differentiator from STEMI: Pericarditis has no reciprocal ST depressions, PR depression is present, ST elevation is diffuse (not localized to a coronary territory), and ST shape is concave (saddle-shaped).
ECG Image - Acute Pericarditis:
 (Source: ECG Waves - Pericarditis - Note diffuse concave ST elevations without reciprocal depressions)
(Source: ECG Waves - Pericarditis - Note diffuse concave ST elevations without reciprocal depressions)
6. Left Ventricular Hypertrophy (LVH)
Pathophysiology: Thickened left ventricular wall from chronic pressure overload (hypertension, aortic stenosis), producing larger electrical forces.
ECG Changes:
- Voltage criteria (Sokolow-Lyon): S in V1 + R in V5 or V6 ≥ 35 mm
- Cornell criteria: R in aVL + S in V3 > 28 mm (men), > 20 mm (women)
- Left axis deviation
- ST depression + T-wave inversions in lateral leads (I, aVL, V5-V6) = "strain pattern" (most specific finding)
- Broad, notched P wave (P mitrale) from associated left atrial enlargement
- Wide QRS (may exceed 110 ms)
ECG Image - LVH:
 (Source: LITFL ECG Library - Tall lateral R waves with lateral ST depression/T inversion strain pattern)
(Source: LITFL ECG Library - Tall lateral R waves with lateral ST depression/T inversion strain pattern)
7. Wolff-Parkinson-White (WPW) Syndrome
Pathophysiology: An accessory pathway (Bundle of Kent) bypasses the AV node, causing ventricular pre-excitation. Can cause life-threatening rapid AF with direct ventricular conduction.
ECG Changes (classic triad):
- Short PR interval < 120 ms (bypasses AV nodal delay)
- Delta wave - slurred upstroke at the beginning of the QRS (pre-excitation of ventricular myocardium)
- Wide QRS > 120 ms (fusion of normal + pre-excited conduction)
- Pseudo-ST changes and T-wave inversions secondary to abnormal depolarization
- During tachycardia: narrow QRS (orthodromic AVRT) or wide QRS (antidromic AVRT or AF with pre-excitation)
ECG Image - WPW:
 (Source: LITFL ECG Library - Short PR interval, delta wave slurring at QRS onset, wide QRS complex)
(Source: LITFL ECG Library - Short PR interval, delta wave slurring at QRS onset, wide QRS complex)
8. Hypertrophic Cardiomyopathy (HCM)
Pathophysiology: Genetic (sarcomere protein mutations) disorder causing asymmetric septal hypertrophy with or without left ventricular outflow tract obstruction. Major cause of sudden cardiac death in young athletes.
ECG Changes:
- LVH voltage changes (tall R waves, deep S waves)
- Deep, narrow Q waves ("dagger Q waves") in lateral and inferior leads (I, aVL, V5-V6, II, III, aVF) - due to septal hypertrophy
- ST depression and T-wave inversions in lateral leads
- Giant negative T waves in the apical variant (Yamaguchi syndrome, V3-V5)
- Left axis deviation
- Atrial fibrillation in advanced disease
- Pre-excitation pattern may coexist
9. Pulmonary Embolism (PE)
Pathophysiology: Acute right heart strain from pulmonary artery obstruction, causing acute RV pressure overload and dilatation.
ECG Changes:
- Sinus tachycardia - most common finding (~40% of PE)
- S1Q3T3 pattern - deep S wave in lead I, Q wave + T-wave inversion in lead III (present in ~20%, not specific)
- Right bundle branch block (RBBB) - new or incomplete
- Right axis deviation
- T-wave inversions in V1-V4 (right ventricular strain pattern - most specific)
- P pulmonale (tall, peaked P waves > 2.5 mm in II) from right atrial strain
- Atrial fibrillation or flutter
- Electrical alternans if associated with pericardial effusion
ECG Image - Pulmonary Embolism:
 (Source: LITFL ECG Library - S1Q3T3 pattern with right heart strain changes)
(Source: LITFL ECG Library - S1Q3T3 pattern with right heart strain changes)
10. Long QT Syndrome (LQTS) / Torsades de Pointes
Pathophysiology: Prolonged ventricular repolarization (congenital mutation in ion channel genes, or drug-induced/electrolyte abnormalities) predisposes to polymorphic VT called Torsades de Pointes (TdP), which can degenerate into VF and sudden death.
ECG Changes - LQTS:
- Prolonged QTc interval: QTc > 450 ms (men), > 460 ms (women) by Bazett formula
- T-wave morphology abnormalities: notched, bifid, or broad T waves
- U waves may be prominent
- QTc > 500 ms = high risk of Torsades
ECG Changes - Torsades de Pointes:
- Polymorphic VT - QRS complexes that "twist" around the isoelectric baseline
- Axis changes every 5-20 beats (waxing and waning amplitude)
- Initiated by a long-short RR sequence (R-on-T phenomenon)
- May be self-terminating or degenerate to VF
ECG Image - Torsades de Pointes:
 (Source: LITFL ECG Library - Characteristic "twisting" QRS morphology around the isoelectric baseline)
(Source: LITFL ECG Library - Characteristic "twisting" QRS morphology around the isoelectric baseline)
Quick Reference Summary Table
| # | Disease | Rate | Rhythm | Key ECG Feature |
|---|---|---|---|---|
| 1 | STEMI | Variable | Regular | ST elevation + reciprocal depressions, Q waves |
| 2 | Atrial Fibrillation | Varies | Irregularly irregular | No P waves, fibrillatory baseline |
| 3 | Ventricular Tachycardia | 100-250 | Regular | Wide QRS, AV dissociation, fusion beats |
| 4 | Complete Heart Block | Slow | Regular (escape) | P-QRS dissociation (P rate > QRS rate) |
| 5 | Pericarditis | Normal/fast | Regular (usually) | Diffuse saddle ST elevation, PR depression |
| 6 | LVH | Normal | Regular | High voltage + lateral strain pattern |
| 7 | WPW | Normal (or fast) | Regular | Short PR, delta wave, wide QRS |
| 8 | HCM | Normal | Regular | Deep narrow Q waves, LVH, T inversions |
| 9 | Pulmonary Embolism | Fast | Regular/AF | Sinus tach, S1Q3T3, RV strain V1-V4 |
| 10 | Long QT / Torsades | Normal/fast | Polymorphic | Prolonged QTc, twisting QRS (TdP) |
Key Resources for ECG Learning:
- LITFL ECG Library - comprehensive free ECG examples
- ECG Waves (ecgwaves.com) - detailed ECG teaching with case-based learning
- Harrison's Principles of Internal Medicine 22E - Myocardial Ischemia and Infarction chapter
- Tintinalli's Emergency Medicine - Electrocardiography section
Note: ECG interpretation must always be correlated with clinical history, symptoms, and other investigations. If some images don't render due to external hosting, click the source links above to view them directly on LITFL or ECGwaves.
This is a shared conversation. Sign in to Orris to start your own chat.