Parathyroid adenoma in surgical oncology case
Reading File
Finding Sources
Finding Sources
Searching PubMed
"parathyroid adenoma"[MeSH Terms] AND "parathyroidectomy"[MeSH Terms]
Reading File
Reading File
Searching PubMed
"primary hyperparathyroidism"[MeSH Terms] AND "parathyroidectomy"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the essential information for a thorough surgical oncology case presentation on parathyroid adenoma. Let me compile the full answer.
Parathyroid Adenoma - Surgical Oncology Case
Overview
Primary hyperparathyroidism (PHPT) is caused by a single benign parathyroid adenoma in approximately 85% of cases (range 66-93%). The remaining cases involve multigland disease (MGD, ~15%), including double adenoma (~6%), or the rare parathyroid carcinoma (~1%). PHPT prevalence is approximately 0.3% of adults, and is likely underdiagnosed.
Pathology
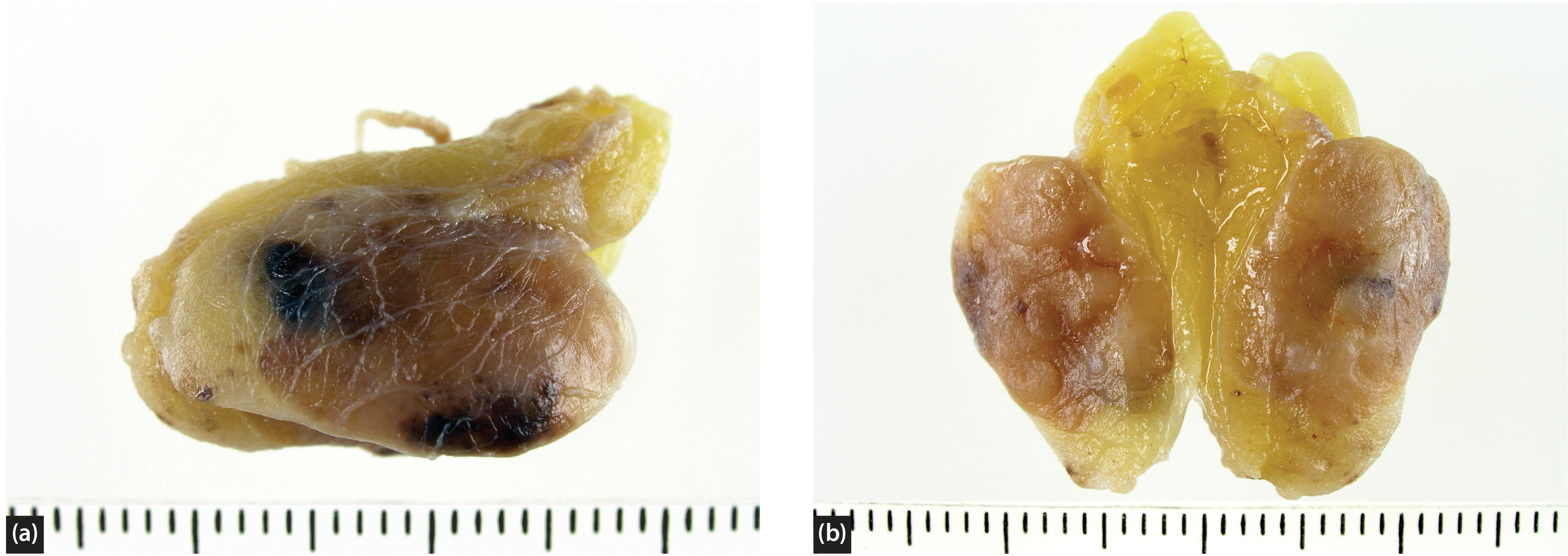
Gross appearance: Parathyroid adenomas are well-marginated, soft tumors varying from yellow-red to orange-brown. Mean weight is 0.55 g, though tumors as large as 53 g are recorded. Generally, the more severe the hypercalcemia, the bulkier the adenoma.
WHO Classification (4th Ed., 2017) of parathyroid gland tumors:
- Parathyroid carcinoma
- Parathyroid adenoma
- Secondary, mesenchymal and other tumors
Histological Variants:
| Variant | Key Features |
|---|---|
| Cystic adenoma | Cystic ab initio or secondary to infarction/hematoma |
| Lipoadenoma (parathyroid hamartoma) | Admixture with copious adipocytes, 20-90% fat; ~50% associated with hypercalcemia |
| Papillary variant | Rare; can mimic papillary thyroid carcinoma |
| Water-clear adenoma | Substantially or wholly composed of water-clear cells |
Secondary phenomena (non-specific diagnostically): inflammation, infarction, hemorrhage, hemosiderosis, fibrosis/hyalinosis, metaplastic ossification.
Location: Adenomas occur more frequently in the inferior parathyroid glands. Ectopic locations include mediastinum, thyroid, esophagus, and intrathyroidal - these may mimic thyroid adenoma or medullary thyroid carcinoma histologically.
Pathophysiology
PTH (84 amino acid peptide) raises serum calcium via three mechanisms:
- Bone resorption - PTH increases osteoclast maturation, shifting bone balance toward destruction and freeing stored calcium
- Renal calcium reabsorption - PTH acts on the distal tubule to increase reabsorption; paradoxically, sustained PTH elevation causes hypercalciuria (predisposing to nephrolithiasis)
- Activation of vitamin D - PTH stimulates 1-alpha-hydroxylase in the kidney, converting 25-OH-D3 to active 1,25-(OH)2-D3, increasing intestinal calcium absorption
In PHPT, one or more parathyroid glands function autonomously, independent of the negative feedback from hypercalcemia.
Clinical Presentation
The classic mnemonic is "Stones, Bones, Groans, and Psychic Moans":
- Nephrolithiasis/Renal: Calcium oxalate/phosphate stones, nephrocalcinosis, polyuria
- Skeletal: Osteoporosis, fractures, osteitis fibrosa cystica (severe/long-standing)
- GI/Abdominal: Nausea, constipation, peptic ulcers, pancreatitis
- Neuropsychiatric: Depression, anxiety, cognitive impairment, fatigue
Modern PHPT is predominantly asymptomatic at presentation (detected incidentally on routine chemistry).
Suspect parathyroid carcinoma when:
- Calcium >14 mg/dL
- PTH >5x upper limit of normal
- Palpable neck mass
- Idiopathic hoarseness
Diagnosis / Biochemistry
| Test | Finding in PHPT |
|---|---|
| Serum calcium | Elevated (hypercalcemia) |
| Serum PTH (intact) | Elevated or inappropriately normal |
| Serum phosphate | Low-normal to low |
| 24-hr urine calcium | Elevated |
| Vitamin D (25-OH) | Normal or low (exclude secondary HPT) |
| Alkaline phosphatase | Elevated (in bony disease) |
Normocalcemic PHPT is a diagnosis of strict exclusion after eliminating all secondary causes; ionized calcium must be measured.
Familial syndromes to screen for:
- MEN1 (hyperparathyroidism + pituitary + pancreatic tumors)
- MEN2A (hyperparathyroidism + medullary thyroid carcinoma + pheochromocytoma)
- Familial isolated hyperparathyroidism
- HPT-JT syndrome (jaw tumor syndrome)
Preoperative Localization
Surgery depends on accurate localization. The key modalities:
Ultrasound
- First-line, widely available, no radiation
- Sensitivity ~70-80% for single adenomas
- Limited for ectopic/mediastinal/deep glands
Sestamibi Scintigraphy (Tc-99m)
- Retained in mitochondria-rich oxyphil cells of hyperfunctioning parathyroids
- Planar: Sensitivity limited (12-25% negative)
- SPECT: 3D; sensitivity 87-91% for single adenomas
- SPECT/CT: Sensitivity up to 96% for single adenomas; significantly less radiation than 4D-CT; improved MGD detection
- Negative correlates with: small gland size, coexisting thyroid disease, superior location, calcium channel blocker use, MGD
4D-CT (Four-Dimensional CT)
- Dynamic contrast CT (3 spatial dimensions + time)
- Exploits rapid contrast uptake and washout by adenoma vs. surrounding tissue
- Excellent anatomic detail, useful for ectopic glands and reoperative cases
- Higher radiation dose than SPECT/CT
Concordant localization (two modalities agreeing) = strongest indication for focused/minimally invasive parathyroidectomy (MIP).
Indications for Surgery
Surgery is the only curative treatment for PHPT. Standard indications include:
| Criterion | Threshold |
|---|---|
| Serum calcium | >1 mg/dL above upper limit of normal |
| Bone mineral density (T-score) | <-2.5 at any site, or vertebral fracture |
| Renal | CrCl <60 mL/min, 24-hr urine calcium >400 mg/day with nephrolithiasis risk, renal stones by imaging |
| Age | <50 years |
| Patient preference | Unable/unwilling for surveillance |
Benefits of curative parathyroidectomy are objective and extend to: bone mineral density, fracture-free survival, renal dysfunction, sleep, quality of life, neurocognitive function including depression/anxiety. ~80% of patients show objective benefit at 6 months.
Surgical Approaches
1. Minimally Invasive Parathyroidectomy (MIP)
Indication: Single adenoma with concordant preoperative localization
Technique:
Technique:
- Focused unilateral exploration through a small incision
- The adenoma is identified, circumferentially dissected, and excised
- Careful preservation of the recurrent laryngeal nerve (RLN)
- Hilar vessels clamped and ligated; gland sent for histology
Inferior adenoma: Usually anterior to RLN and inferior to inferior thyroid artery
Superior adenoma: Usually posterior (retropharyngeal/retroesophageal space); thyroid retracted medially; pedicle identified posteromedially, clipped, and divided
Superior adenoma: Usually posterior (retropharyngeal/retroesophageal space); thyroid retracted medially; pedicle identified posteromedially, clipped, and divided
2. Bilateral Neck Exploration (BNE)
Indication: Discordant/negative localization, suspected MGD, familial disease, failed MIP
Identifies all four glands; allows complete assessment of gland number and size.
Identifies all four glands; allows complete assessment of gland number and size.
3. Intraoperative PTH Monitoring (IOPTH) - "Miami Criterion"
- PTH half-life ~3-5 minutes
- Cure criterion: PTH falls by >50% from pre-excision baseline at 10 minutes post-excision
- Predictive of cure in ~98% of cases
- If PTH does not drop adequately, continued exploration is mandatory
- Replaces the need for bilateral exploration in focused surgery
Intraoperative Gland Recognition
| Feature | Normal Gland | Adenoma | Carcinoma |
|---|---|---|---|
| Weight | 20-50 mg | Variable, often >500 mg | Variable |
| Size | <5 mm | Enlarged | Variable |
| Color | Yellow-pink-ochre | Wider array; spherical, plump | White, firm |
| Adherence | Loose | Extrudes readily | Locally adherent |
Important: Capsule entry into parathyroid glands is strictly avoided to prevent parathyromatosis (seeding of parathyroid tissue). Normal-appearing glands are biopsied at only 50-100 mg.
Embryology & Ectopic Glands
| Gland | Branchial Pouch | Typical Location | Ectopic Migration Path |
|---|---|---|---|
| Superior (2) | 4th | Lateral/deep to RLN, tracheoesophageal groove | Posterior mediastinum, retroesophageal space |
| Inferior (2) | 3rd | Medial/anterior to RLN, lower thyroid pole | Anterior mediastinum (thymic descent), carotid sheath |
Up to 13% of people have 5 or more parathyroid glands (supernumerary), especially relevant in MEN1. Mediastinal adenomas may require thoracoscopic or open thoracic approach after definitive localization.
Complications of Parathyroidectomy
| Complication | Notes |
|---|---|
| Recurrent laryngeal nerve palsy | Uncommon; risk higher in reoperative/ectopic cases |
| Hypocalcemia (transient) | "Hungry bone syndrome" post-cure; supplement calcium |
| Permanent hypoparathyroidism | ~5% of adenoma cases |
| Persistent disease | Failure to remove causative gland |
| Recurrent disease | Regrowth from adenoma stump, unrecognized carcinoma, or incorrect diagnosis (e.g., familial hypocalciuric hypercalcemia - FHH) |
| Bleeding/hematoma | Monitor 4-6 hours post-op; airway emergency |
| Parathyromatosis | From capsule rupture/seeding |
Postoperative Care
- Calcium and PTH levels checked at 4-6 weeks to confirm cure
- Routine oral calcium supplementation on discharge (minimum 24-48 hours)
- Day-case procedure is standard in most centers; 4-6 hour minimum observation
- Wound review and biochemistry at 6-week follow-up
- Up to 10% of patients relapse, sometimes after many years
Concomitant Thyroid Disease
If a large (>4 cm), cytologically benign thyroid nodule is ipsilateral to a localized parathyroid adenoma, concurrent thyroid resection may be offered. All parathyroid glands should be examined during thyroid surgery.
Sources:
- Fischer's Mastery of Surgery, 8th Edition - Ch. 39 (Primary Hyperparathyroidism)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 1 - Ch. 58, 77
- Henry's Clinical Diagnosis and Management by Laboratory Methods
Anaemia in pregnancy
Reading File
Finding Sources
Finding Sources
Searching PubMed
"anemia"[MeSH Terms] AND "pregnancy"[MeSH Terms]
Finding Sources
Finding Sources
Reading Article
PMID: 41031541
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
I now have comprehensive, authoritative content from Creasy & Resnik's Maternal-Fetal Medicine. I have all I need for a thorough response. Let me compile the full answer now.
Anaemia in Pregnancy
Definition
WHO (and FIGO 2025) definition: Haemoglobin (Hb) < 11 g/dL in all trimesters of pregnancy and during the postpartum period.
Anaemia affects 32 million pregnant women globally, contributing to >115,000 maternal deaths and >591,000 perinatal deaths annually. Low- and middle-income countries bear the greatest burden (~50% of affected women). The global prevalence remains more than twice WHO's 2025 target of 15%.
Physiological Changes of Pregnancy (Understanding the Baseline)
During normal pregnancy, there is a disproportionate expansion of plasma volume vs. RBC mass:
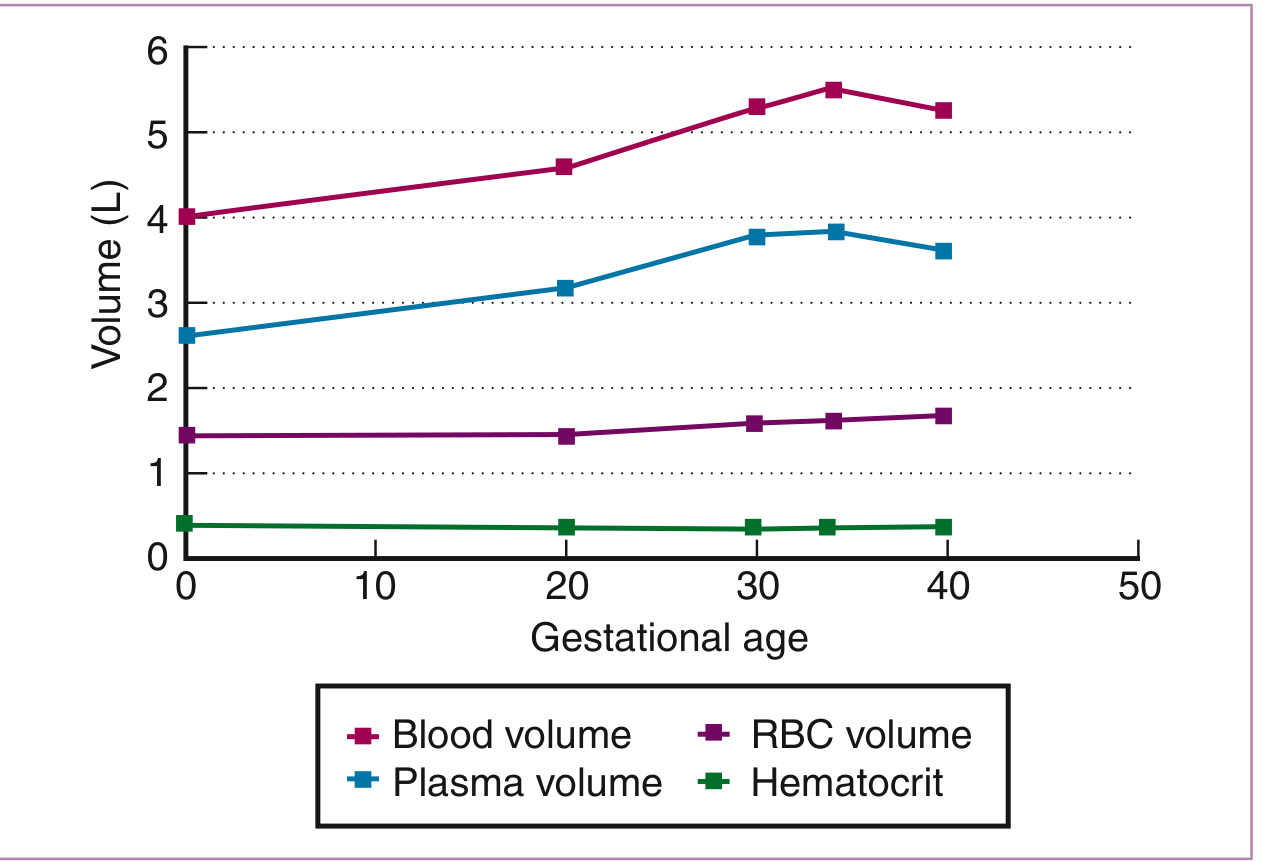
| Parameter | Change in Pregnancy |
|---|---|
| Blood volume | +40-45% (max at 34 weeks) |
| Plasma volume | +47% (max at 28-34 wks) |
| RBC mass | +17% (max at term) |
| Haemoglobin / Hct / RBC count | Relatively decreased (hemodilution) |
| MCV, MCHC | No change (useful in distinguishing dilutional from true IDA) |
"Physiologic anaemia of pregnancy": Normocytic anaemia with Hb >11 g/dL (late first trimester) or >10 g/dL (second/third trimester) in an uncomplicated pregnancy - no further workup needed. Lower values or microcytic/macrocytic picture requires investigation.
Key distinguishing point: In dilutional anaemia, MCV and MCHC remain constant. In progressive IDA, both decrease.
Classification & Causes
1. Iron Deficiency Anaemia (IDA) - Most Common (~75%)
Why pregnancy worsens iron balance:
- Total iron requirement of pregnancy = ~1130 mg (range 580-1340 mg)
| Required for | Average (mg) | Range (mg) |
|---|---|---|
| External iron loss | 170 | 150-200 |
| Expansion of RBC mass | 450 | 200-600 |
| Fetal iron | 270 | 200-370 |
| Placenta and cord | 90 | 30-170 |
| Blood loss at delivery | 150 | 90-310 |
| Total | 1130 | 580-1340 |
- Most women enter pregnancy with marginal iron stores (~two-thirds of healthy women have minimal marrow iron stores)
- Estimated average daily iron requirement in pregnancy = 22-23 mg/day; median dietary intake is only 15 mg/day
- IDA increases from 8% (1st trimester) to 62% (3rd trimester) even with average supplementation
Iron transfer to fetus: Maternal transferrin binds to syncytiotrophoblast receptors → iron released → binds placental ferritin → transferred to apotransferrin → enters fetal circulation as holotransferrin. Placental transferrin receptors upregulate if maternal iron is low - fetus is preferentially protected at mother's expense.
Three stages of iron deficiency:
- Prelatent: Decreased serum ferritin only (marrow stores depleted)
- Latent: Abnormal iron studies (↓ serum iron, ↑ TIBC, ↓ transferrin saturation); Hb normal
- Manifest IDA: ↓ Hb, then ↓ MCV (microcytic hypochromic anaemia)
Diagnosis:
- Serum ferritin - most accurate single test for IDA in pregnancy
- Ferritin < 12 µg/L = IDA; < 20 µg/L = iron deficiency (used by some authors)
- Caveat: ferritin is an acute phase reactant - may be falsely normal in infection/inflammation
- Measuring Hb alone is inadequate (only 6% of women with ferritin <20 µg/L have anaemia)
- Soluble transferrin receptor (sTfR): Not affected by inflammation; elevated value supports IDA; limited by lack of standardization
- Blood film: Microcytic, hypochromic RBCs, pencil cells, anisocytosis, poikilocytosis
2. Megaloblastic Anaemia
Folate deficiency (more common):
- Folate requirement increases from 400 µg/day (non-pregnant) to 600 µg/day during pregnancy
- Critical from periconception: adequate folate before and during first weeks of pregnancy reduces neural tube defects (spina bifida, anencephaly) by ~50-70%
- Higher requirement in: multiple pregnancy, haemolytic anaemia
- Absorption decreased by: anticonvulsants, oral contraceptives, alcohol, sulfa drugs
- Folate deficiency defined as serum level < 2.5-3 ng/mL
Vitamin B12 deficiency (less common in pregnancy):
- Dietary B12 absorbed via intrinsic factor (gastric parietal cells)
- Risk factors: strict vegetarianism/veganism, pernicious anaemia, gastrectomy
- Blood film: macrocytic anaemia, hypersegmented neutrophils
- Serum B12 level falls physiologically in pregnancy (not always true deficiency)
3. Haemoglobinopathies
Sickle cell disease (SCD) in pregnancy:
- Maternal complications: more frequent pain crises, increased risk of VTE, preeclampsia, pyelonephritis, pulmonary complications
- Treatment of pain crises: same as in non-pregnant patients
- Hydroxyurea is CONTRAINDICATED in pregnancy (known teratogenicity)
- Blood transfusion for severe anaemia; prophylactic transfusion in some centres
Thalassaemia:
- Alpha-thalassaemia trait: usually mild microcytic anaemia; Hb Bart's disease (hydrops fetalis) lethal
- Beta-thalassaemia trait: microcytic hypochromic anaemia, Hb A2 >3.5%; partner screening essential
- Beta-thalassaemia major: requires transfusion support throughout pregnancy (rare to reach reproductive age without treatment)
Investigation: Hb electrophoresis (reference: Hb A > 98%, Hb A2 < 3.5%)
4. Autoimmune Haemolytic Anaemia (AIHA)
- Warm-reactive antibodies (IgG): directed against Rh antigens; associated with lupus, lymphoproliferative disorders, drugs (penicillin, methyldopa)
- Cold-reactive antibodies (IgM): against I/i antigens; associated with Mycoplasma, EBV
- Diagnosis: hyperproliferative macrocytic anaemia + positive direct Coombs test + peripheral smear showing spherocytes, polychromatophilia
- Treatment: blood transfusion, corticosteroids (~80% respond with warm AIHA), immunosuppression; splenectomy (second-line, ~60% effective for warm AIHA); rituximab (anti-CD20) used successfully in refractory cases during pregnancy without adverse maternal/fetal outcomes
5. G6PD Deficiency
- X-linked; affects >400 million people worldwide
- G6PD maintains glutathione in reduced state to protect RBCs from oxidant stress
- Female heterozygotes generally unaffected but some may have low G6PD activity (Lyon hypothesis)
- Haemolytic crises triggered by: oxidant drugs, infections, fava beans
- Drugs to avoid: primaquine, nitrofurantoin, sulfa drugs, dapsone, aspirin (high dose)
6. Aplastic Anaemia in Pregnancy
- Rare; may be pregnancy-induced (some cases remit after delivery)
- Pancytopenia; hypocellular bone marrow
- Treatment: supportive transfusions, immunosuppression; haematopoietic stem cell transplant deferred until after delivery
7. Anaemia of Chronic Disease / Inflammation
- Normocytic normochromic anaemia; both serum iron and TIBC decreased; transferrin saturation usually normal; ferritin normal or elevated
Laboratory Reference Ranges in Pregnancy (Creasy & Resnik's)
| Test | Reference Range |
|---|---|
| MCV | 81-96 µm³ (1st), 82-97 (2nd), 81-99 (3rd) |
| MCHC | 32-35 g/dL |
| Serum ferritin | >20 µg/L (1st trimester: 72-143 µg/dL) |
| Serum iron | 44-178 µg/dL (2nd); 30-193 µg/dL (3rd) |
| TIBC | 235-408 µg/dL (1st); rises through 3rd trimester |
| Transferrin saturation | 16-60% |
| Serum folate | 26-150 µg/L (1st trimester) |
| Serum vitamin B12 | 118-438 pg/mL (1st); 130-656 (2nd); 99-526 (3rd) |
| Direct Coombs | Negative |
| Hb electrophoresis | >98% A; <3.5% A2 |
Management
Screening (FIGO 2025 Guideline)
- Screen all pregnant women at booking and again at 28 weeks with full blood count (FBC), or packed cell volume/Hb where FBC is unavailable.
Iron Deficiency Anaemia
Supplementation/Prevention:
- Supplementation with 60 mg elemental iron/day during second and third trimesters meets daily requirements
- Iron supplementation reduces incidence of anaemia by up to 73%
- National Academy of Medicine: offer supplementation to women with ferritin < 20 µg/L
- Routine supplementation (regardless of ferritin) is common practice in the US
Oral iron:
- First-line for mild-moderate IDA; second and second/third trimester
- Ferrous sulfate 200 mg TDS (65 mg elemental iron each) or ferrous gluconate/fumarate
- Take on empty stomach or with vitamin C to enhance absorption
- Side effects: nausea, constipation - may limit compliance
Intravenous iron:
- Contraindicated in first trimester (anaphylaxis risk + limited safety data)
- Treatment of choice for IDA in third trimester and for severe IDA in second trimester
- Also used when oral iron is not tolerated or insufficient
- Formulations: ferric carboxymaltose, iron sucrose, low-molecular-weight iron dextran
- A 2024 Cochrane review (PMID: 39145520) confirmed daily oral iron supplementation during pregnancy reduces maternal anaemia and improves haemoglobin at term
Folate Deficiency
- Folic acid 5 mg/day for treatment of established megaloblastic anaemia
- 400 µg/day for prevention in low-risk pregnancies (start periconception)
- 5 mg/day periconceptionally for high-risk (previous NTD, epilepsy, malabsorption, twins, haemolytic anaemia)
Vitamin B12 Deficiency
- Cyanocobalamin or hydroxocobalamin supplementation
- IM injections if malabsorption/pernicious anaemia
Severe / Symptomatic Anaemia
- Blood transfusion when Hb <7 g/dL or symptomatic (dyspnoea at rest, cardiac decompensation)
- Threshold may be higher (Hb <8-9 g/dL) in haemoglobinopathies or those with poor tolerance
- Always use leukodepleted, CMV-negative blood in haemoglobinopathy patients (to minimise alloimmunisation)
Malaria / Helminth Prophylaxis (FIGO 2025)
- In endemic regions: intermittent preventive treatment with sulphadoxine-pyrimethamine (IPTp-SP) reduces malaria-associated anaemia
- Anti-helminthic chemoprophylaxis (mebendazole/albendazole) in endemic areas reduces hookworm-associated IDA - give after first trimester
Maternal and Fetal Consequences
| Consequence | Mechanism |
|---|---|
| Preterm labour / low birth weight | Placental insufficiency, fetal hypoxia |
| Increased postpartum haemorrhage (PPH) risk | Pre-existing anaemia worsens haemodynamic impact of blood loss |
| Maternal mortality | Severe anaemia + PPH = leading cause in LMICs |
| Perinatal mortality | Fetal hypoxia, placental insufficiency |
| Impaired neonatal iron stores | Iron-deficient mother → reduced fetal iron stores |
| Neurodevelopmental impairment | Neonatal iron deficiency affects myelination and cognitive development |
| Neural tube defects | Periconceptional folate deficiency |
Key Points Summary
- Anaemia in pregnancy = Hb < 11 g/dL (all trimesters, WHO/FIGO)
- IDA is most common (~75%); serum ferritin is the best single diagnostic test
- Plasma volume rises disproportionately to RBC mass → physiologic hemodilution
- Three-stage progression of IDA: ferritin ↓ → iron studies abnormal → Hb ↓ → MCV ↓
- Oral iron is first-line; IV iron is preferred in 3rd trimester and severe IDA; avoid in 1st trimester
- Folate 400 µg/day periconceptionally prevents neural tube defects; 5 mg/day for high-risk women
- Screen at booking and at 28 weeks (FIGO 2025)
- Hydroxyurea is contraindicated in pregnancy (sickle cell)
Sources:
- Creasy & Resnik's Maternal-Fetal Medicine, 8th Edition, Ch. 55
- Goldman-Cecil Medicine, 27th Edition, Ch. 150
- Rosen's Emergency Medicine, 9th Edition, Ch. 177
- FIGO Good Practice Recommendations on Anemia in Pregnancy, 2025 (PMID: 41031541)
- Cochrane Review: Daily oral iron supplementation during pregnancy, 2024 (PMID: 39145520)
This is a shared conversation. Sign in to Orris to start your own chat.