Anemia during pregnancy
Reading File
Finding Sources
Searching PubMed
"anemia" AND "pregnancy"
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of anemia during pregnancy, drawn from Creasy & Resnik's Maternal-Fetal Medicine, Goldman-Cecil Medicine, and Rosen's Emergency Medicine.
Anemia During Pregnancy
Definition
Anemia in pregnancy is defined as:
- Hemoglobin (Hb) < 11 g/dL in the 1st and 3rd trimesters
- Hb < 10.5 g/dL in the 2nd trimester (some sources use < 10 g/dL)
Note: the threshold is lower than in non-pregnant women (12 g/dL) because of the normal dilutional effect of pregnancy.
1. Physiologic (Dilutional) Anemia of Pregnancy
This is a normal and expected change, not a pathological condition.
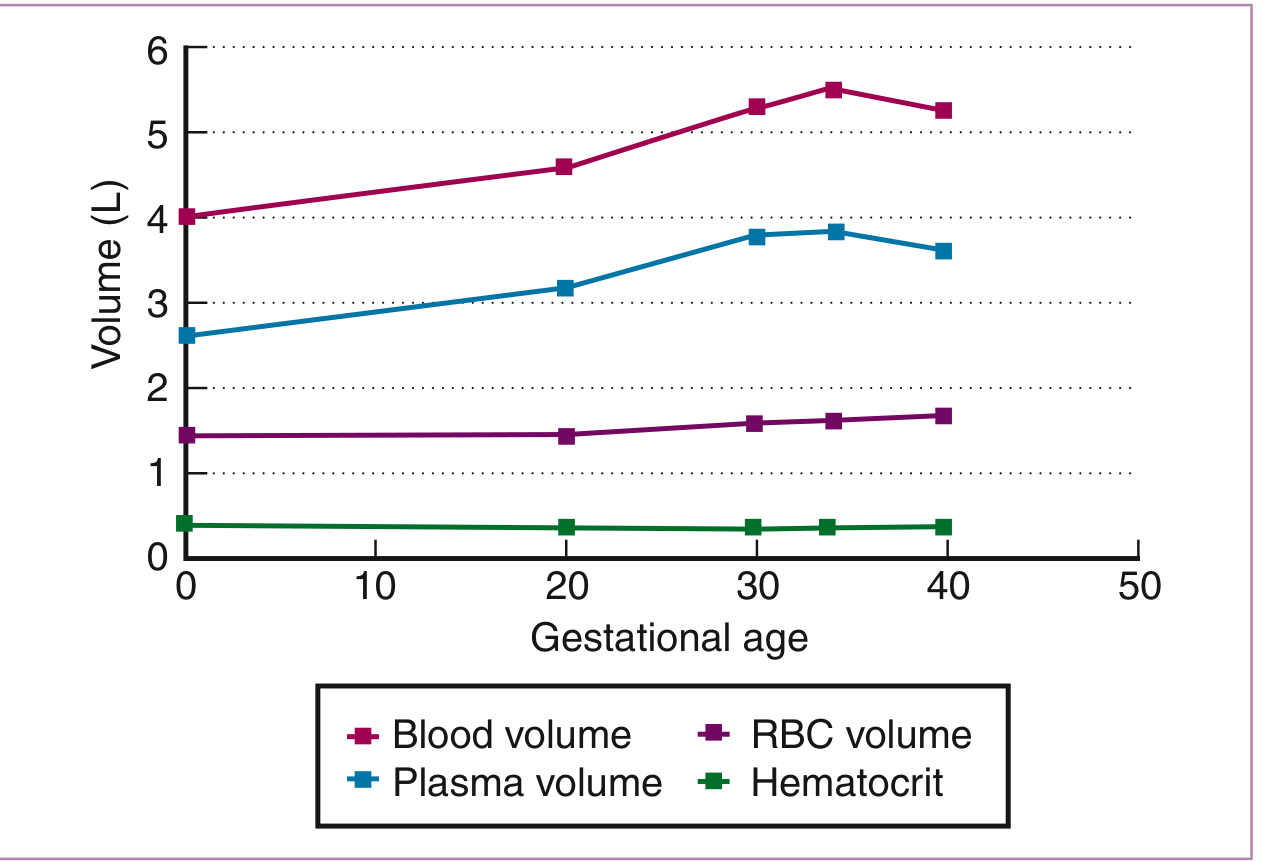
- Starting around week 6-7, blood volume increases by ~40-50% by 34 weeks, primarily driven by a 47% rise in plasma volume
- Red cell mass rises by only 17%, peaking at term
- This disproportionate plasma expansion causes hemodilution, with Hb nadir between weeks 26-28
- MCV and MCHC remain unchanged in pure dilutional anemia - serial monitoring of these indices helps distinguish it from progressive iron deficiency anemia (IDA), where they fall progressively
Gravid patients with hemoglobin values of 13-15 g/dL may actually have inadequate plasma volume expansion, which is linked to low birthweight and preterm birth.
2. Causes of Pathologic Anemia in Pregnancy
| Cause | Type | Frequency |
|---|---|---|
| Iron deficiency | Microcytic, hypochromic | Most common (~18% iron deficient; ~5% have IDA) |
| Folate deficiency | Macrocytic, megaloblastic | 2nd most common |
| Vitamin B12 deficiency | Macrocytic, megaloblastic | Less common |
| Hemoglobinopathies (sickle cell, thalassemia) | Variable | Important in at-risk populations |
| Aplastic anemia | Normocytic | Rare |
| Hemolytic anemias | Variable | Rare |
3. Iron Deficiency Anemia (IDA)
Pathophysiology
Pregnancy imposes heavy iron demands. Approximately 2/3 of healthy non-pregnant women already have minimal bone marrow iron stores. The iron requirements of pregnancy (fetal needs, expanding red cell mass, placenta) exceed the iron saved from 9 months of amenorrhea. Incidence of iron deficiency rises from 18% in the 1st trimester to 29% by the 3rd trimester in US women.
Risks of IDA
The severity of anemia correlates with adverse outcomes:
- Mild-moderate anemia: higher risk of preterm birth, low birth weight
- Severe anemia (Hb < 6-7 g/dL): increased fetal mortality, abnormal fetal oxygenation, premature rupture of membranes, gestational hypertension, reduced amniotic fluid
Diagnosis
Serum ferritin is the most sensitive and specific test:
- Ferritin cutoff of 30 ng/mL = 92% sensitivity, 98% specificity for IDA in pregnancy
- Note: ferritin is an acute-phase reactant and may be falsely normal in inflammation
- MCV and TIBC are less sensitive/specific than ferritin
- Measuring Hb alone is inadequate to screen for iron deficiency (only 6% of women with ferritin < 20 μg/L are also anemic)
Treatment of IDA
Oral iron (first-line for mild-moderate IDA):
- Ferrous sulfate 325 mg 1-3x daily (most common in the US)
- WHO recommends 60 mg elemental iron + folic acid daily; 30 mg may suffice with micronutrients
- A single daily dose is as effective as multiple doses and reduces GERD risk
- Coadministration with 500 mg ascorbic acid enhances absorption
- Reticulocytosis expected within 7-10 days; Hb can rise ~1 g/dL/week in severe cases
- Continue iron for 6 months after resolution to replenish stores
- Intermittent dosing (2-3x/week) provides equivalent benefit with fewer GI side effects
IV iron (preferred in specific situations):
- Contraindicated in the 1st trimester
- Treatment of choice for IDA in the 3rd trimester and severe IDA (Hb < 9 g/dL) in the 2nd trimester
- Available IV preparations: iron sucrose (most used), ferric carboxymaltose, ferric gluconate, low-molecular-weight iron dextran, ferumoxytol, iron isomaltoside
- Dose formula for IV iron sucrose: weight × (target Hb - actual Hb) × 0.24 + 500 mg; target Hb = 11-12 g/dL; max 200 mg/day
- Meta-analyses confirm significantly higher Hb and fewer adverse events with IV vs. oral iron
Erythropoietin: Used in refractory severe IDA (Hb < 8.5 g/dL unresponsive to oral iron) as an adjunct; no significant maternal risks reported.
4. Folate Deficiency Anemia
- Folate requirements increase 5-10 fold during pregnancy
- Results in megaloblastic anemia (macrocytic with hypersegmented neutrophils, oval macrocytes)
- Low folate is strongly linked to neural tube defects, placental abruption, preterm birth, low birth weight, preeclampsia, spontaneous abortion
- Risk factors: multiple gestations, short interpregnancy intervals, hyperemesis gravidarum, malabsorption, alcoholism, antiepileptic drug use, poor diet
- Treatment: folic acid supplementation; 0.8 mg/day is sufficient where food fortification is standard; higher doses required in high-risk patients
5. Vitamin B12 Deficiency
- Less common but should be considered, especially in vegans, those with pernicious anemia, or malabsorption syndromes
- Also causes megaloblastic anemia
- Anti-intrinsic factor (AIF) antibody test if pernicious anemia is suspected
6. Hemoglobinopathies in Pregnancy
Sickle cell disease:
- Increased frequency of pain crises during pregnancy
- Elevated risk of VTE and preeclampsia
- Treatment of pain crises same as in non-pregnant patients
- Hydroxyurea is contraindicated (teratogenic)
Thalassemia trait: Usually mild; monitor closely; genetic counseling recommended
7. Laboratory Evaluation Summary
| Test | Reference Range (pregnancy-adjusted) |
|---|---|
| Hb | 1st: depends on trimester; 2nd nadir ~10 g/dL |
| MCV | 81-99 μm³ (stable in dilutional anemia) |
| Serum ferritin | > 20 μg/L (< 30 ng/mL suggests deficiency) |
| Serum iron | Decreases in IDA |
| TIBC | Increases in IDA (rises physiologically in pregnancy) |
| Transferrin saturation | 16-60% |
| Serum folate | Varies by trimester |
| Serum B12 | 99-656 pg/mL (varies by trimester) |
| Direct Coombs test | Negative (positive = immune hemolysis) |
| Reticulocyte count | 0.5-1.5% |
8. Prevention / Prophylaxis
- ACOG, WHO, and major health authorities recommend at least 30 mg elemental iron daily throughout pregnancy for all women
- Routine supplementation reduces the risk of IDA at term
- Women with normal Hb and ferritin > 30 mg/dL do not require treatment, but prophylactic supplementation is still widely recommended
Recent Evidence (2024-2026)
- A 2024 Cochrane meta-analysis (PMID 39145520) on daily oral iron supplementation in pregnancy confirms benefit for reducing IDA and low birth weight.
- A 2025 systematic review (PMID 39087437) found recombinant erythropoietin is a viable option for IDA in pregnancy when other treatments fail.
Sources: Creasy & Resnik's Maternal-Fetal Medicine (9780323828499), Goldman-Cecil Medicine (9780323930345), Rosen's Emergency Medicine (9780323757898)
This is a shared conversation. Sign in to Orris to start your own chat.