Hi
Hi! How can I help you today?
Addision disease
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from multiple textbooks plus clinical images. Here is a full review:
Addison Disease (Primary Adrenocortical Insufficiency)
Definition
Addison disease is primary adrenocortical insufficiency - failure of the adrenal cortex to produce adequate glucocorticoids (cortisol), mineralocorticoids (aldosterone), and adrenal androgens. It affects approximately 1 in 10,000 individuals in the developed world.
- Costanzo Physiology 7th Edition, p. 440
- Tietz Textbook of Laboratory Medicine, 7th Edition, p. 2274
Etiology / Causes
| Setting | Most Common Cause |
|---|---|
| Developed countries | Autoimmune adrenalitis (~70-80%) |
| Worldwide | Tuberculosis (still #1 globally) |
| Children (>80%) | Genetic causes |
Autoimmune Addison Disease (AAD):
- Most common between ages 30-50 years
- Strongly associated with Autoimmune Polyglandular Syndrome (APS):
- APS type 2 (~70%): autosomal dominant, HLA-DRB1 mutation; co-occurs with type 1 diabetes, autoimmune thyroid disease, celiac disease
- APS type 1 (~10%): autosomal recessive, AIRE gene mutation (chromosome 21q22.3); classically presents with chronic candidiasis + hypoparathyroidism + AAD
- APS type 4 (~10%): miscellaneous autoimmune endocrinopathies not fitting APS 1/2/3
- Autoantibodies likely target 21-hydroxylase enzyme → destruction of adrenocortical cells
Other causes:
-
Infections: TB, Neisseria meningitidis (Waterhouse-Friderichsen syndrome), fungal, viral
-
Drugs inhibiting steroidogenesis: ketoconazole, fluconazole, posaconazole, etomidate, rifampicin
-
Neoplastic infiltration, hemorrhage, amyloidosis, hemochromatosis
-
In young boys: adrenoleukodystrophy (ABCD1 gene mutation) - hyperpigmentation precedes neurologic signs; check very-long-chain fatty acids
-
Bilateral adrenalectomy, SLE, antiphospholipid syndrome
-
Tietz Textbook of Laboratory Medicine, p. 2274-2275
Pathophysiology
All three zones of the adrenal cortex are destroyed, leading to:
| Lost Hormone | Consequence |
|---|---|
| Cortisol (glucocorticoid) | Hypoglycemia, anorexia, weight loss, nausea/vomiting, weakness |
| Aldosterone (mineralocorticoid) | Hyperkalemia, metabolic acidosis, hyponatremia, hypotension (decreased ECF volume) |
| DHEA/androstenedione (androgens) | Decreased pubic/axillary hair, decreased libido (women especially) |
Low cortisol removes negative feedback on the hypothalamic-pituitary axis → ACTH rises markedly. ACTH contains the α-MSH fragment, which binds to melanocortin-1 receptors → hyperpigmentation.
- Costanzo Physiology, p. 440
Clinical Features
Systemic:
- Fatigue, muscle weakness, anorexia, weight loss
- Nausea, vomiting, diarrhea
- Hypotension, lightheadedness on standing (orthostatic)
- Headaches, psychosis (in severe cases)
Laboratory:
- Hypoglycemia
- Hyponatremia
- Hyperkalemia
- Hypercalcemia
- Metabolic acidosis
Cutaneous (hallmark sign):
Hyperpigmentation is the most striking and diagnostically important skin finding. It occurs due to ACTH-driven melanocortin receptor stimulation.
Distribution of hyperpigmentation:
- Sun-exposed areas (face, neck, hands)
- Pressure/trauma sites (knees, elbows, knuckles, spine)
- Palmar creases
- Nipples, areolae, axillae, perineum, genitalia
- Mucous membranes
- Recent scars, nevi
Note: "White Addison disease" - rare form where pigmentation does NOT occur.
In women, decreased axillary and pubic hair occurs because androgen production primarily comes from the adrenals (not the ovaries).
Clinical photo - hyperpigmentation of hands in Addison disease:

- Andrews' Diseases of the Skin, p. 579; Fitzpatrick's Dermatology, p. 1391
Addisonian Crisis (Acute Adrenal Insufficiency)
A life-threatening emergency triggered by stress (infection, trauma, surgery).
Features:
- Circulatory collapse and shock
- Severe weakness and vomiting
- Tachycardia + hypotension
- Hyponatremia + hyperkalemia + acidosis
- Cortisol < 5 µg/dL
Glucocorticoid deficiency typically precedes mineralocorticoid deficiency during disease progression - making early diagnosis difficult because symptoms are nonspecific.
- Tietz Textbook of Laboratory Medicine, p. 2276
Diagnosis
Step 1: Morning plasma cortisol + ACTH
Step 2: Cosyntropin (ACTH analog) stimulation test
- Failure to rise above 18-20 µg/dL (or delta < 7-10 µg/dL) after 1 hour = abnormal
- Elevated plasma ACTH confirms primary adrenal insufficiency (vs. secondary, where ACTH is normal/low)
Diagnostic algorithm:
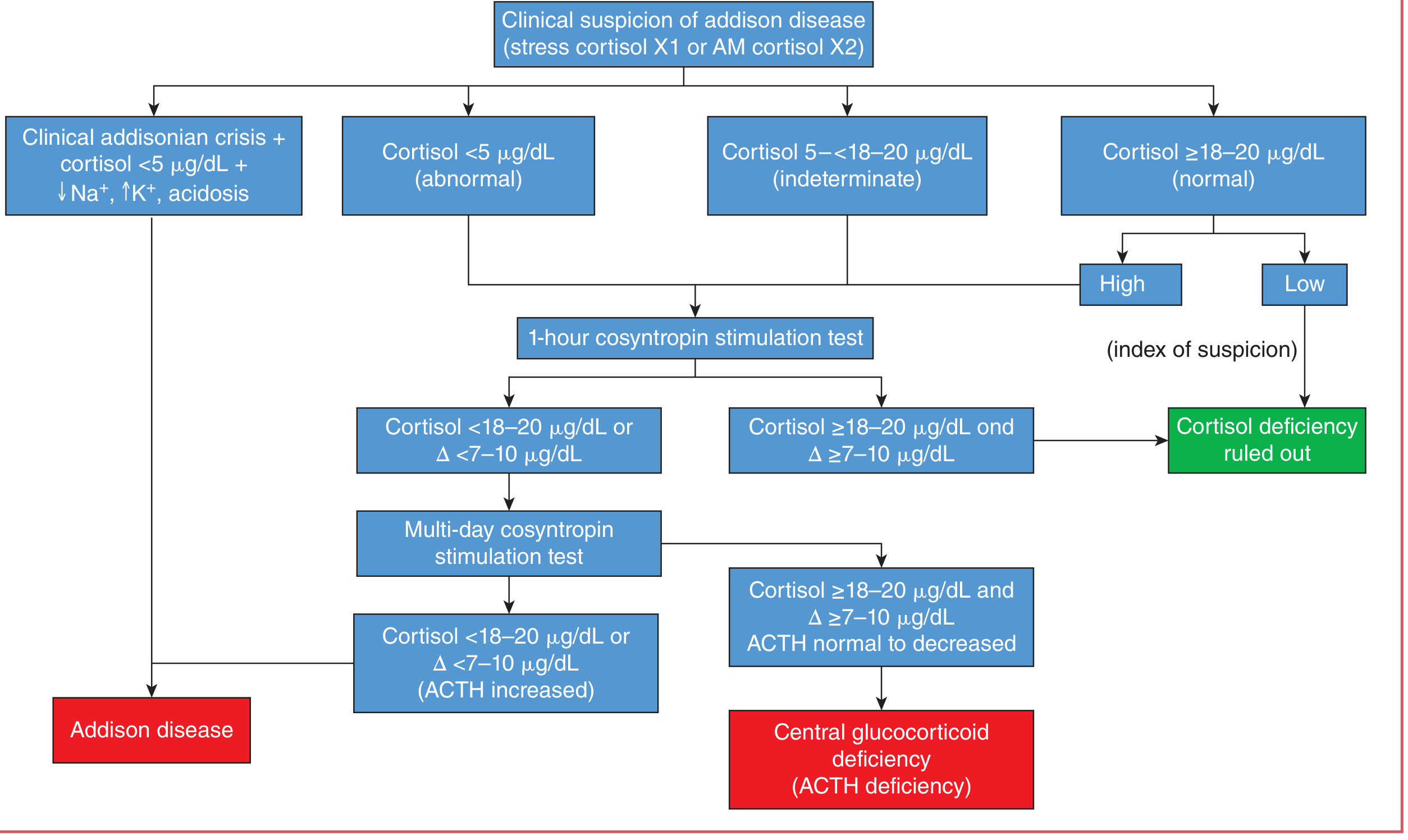
Step 3: CT adrenals - to exclude infiltration, infection, or hemorrhage
- Andrews' Diseases of the Skin, p. 579; Tietz Textbook of Laboratory Medicine
Treatment
-
Glucocorticoid replacement - hydrocortisone (or equivalent)
-
Mineralocorticoid replacement - fludrocortisone
-
Stress dosing during illness, surgery, or trauma
-
Patient education: sick-day rules, medical alert bracelet
-
Costanzo Physiology, p. 440; Andrews' Diseases of the Skin, p. 579
Key Distinguishing Points (Primary vs. Secondary Adrenal Insufficiency)
| Feature | Primary (Addison) | Secondary (pituitary/hypothalamic) |
|---|---|---|
| ACTH level | HIGH | Low or normal |
| Hyperpigmentation | Present | Absent |
| Mineralocorticoid deficiency | Yes | No (aldosterone regulated by renin-angiotensin) |
| Cause | Adrenal destruction | ACTH deficiency |
Sources: Costanzo Physiology 7th Ed. | Tietz Textbook of Laboratory Medicine 7th Ed. | Andrews' Diseases of the Skin | Fitzpatrick's Dermatology | Bradley and Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.