Parotid gland from bd chaurasia
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive information to give a detailed answer. Note: BD Chaurasia's Human Anatomy is not in the library, but I have covered the parotid gland thoroughly from Gray's Anatomy for Students and other authoritative sources, presenting the content in BD Chaurasia style/format.
Note: BD Chaurasia's Human Anatomy is not available in the textbook library. The information below is drawn from Gray's Anatomy for Students and Scott-Brown's Otorhinolaryngology, which cover the same anatomy as BD Chaurasia - presented in the structured format you would find there.
Parotid Gland
Overview
The parotid gland is the largest of the three paired major salivary glands. It is a purely serous gland, producing watery saliva rich in salivary amylase (ptyalin), which initiates carbohydrate digestion. The gland is enclosed within the split investing layer of the deep cervical fascia (parotid fascia/parotid sheath).
Position and Extent
The parotid gland lies in the parotid region of the face, situated in a shallow, triangular-shaped trench bounded by:
- Anteriorly: Ramus of the mandible (and masseter muscle)
- Posteriorly: Sternocleidomastoid muscle and mastoid process
- Superiorly: Base of the external acoustic meatus and posterior aspect of the zygomatic arch
The gland extends:
- Upward to the zygomatic arch
- Downward to the lower border of the mandible
- Anteriorly over the masseter muscle (up to halfway across)
- Posteriorly over the anterior part of sternocleidomastoid
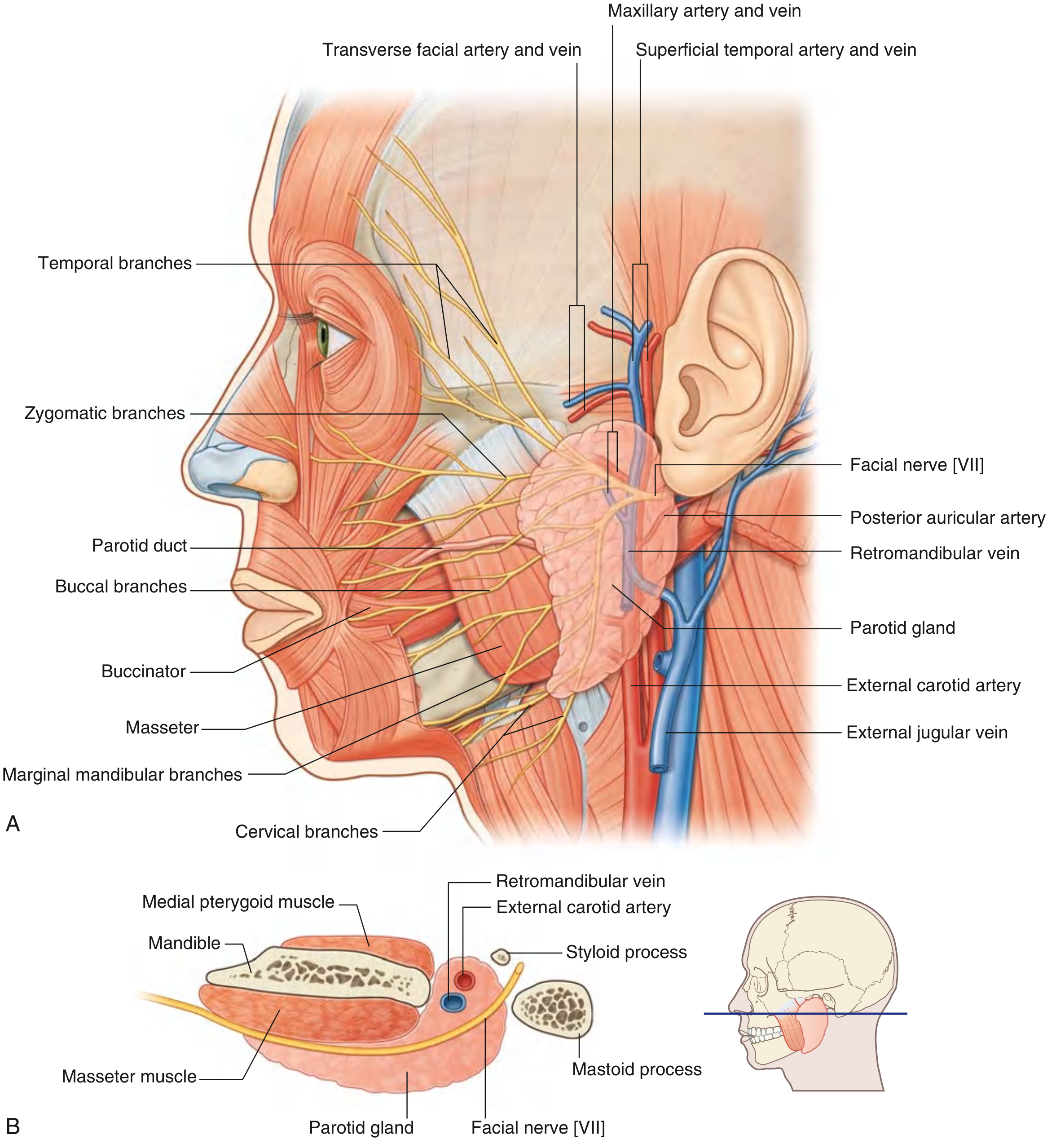
Fig. A - Parotid Gland: (A) Lateral view showing facial nerve branches, parotid duct, and vascular relations; (B) Cross-section showing deep relations
Lobes
The facial nerve [VII] passes through the gland and divides it into two lobes (a surgical concept, not a true anatomical division):
- Superficial lobe - lateral to the facial nerve (~80-90% of gland tissue)
- Deep lobe - medial to the facial nerve (~10-20%)
The deep lobe extends medially through the stylomandibular tunnel toward the parapharyngeal space.
Parotid Duct (Stensen's Duct)
- Emerges from the anterior border of the gland, midway between the zygomatic arch and the corner of the mouth
- Runs transversely across the face, overlying the masseter muscle
- At the anterior border of masseter, turns medially, pierces the buccal fat pad and then the buccinator muscle
- Opens into the oral cavity at a small papilla opposite the crown of the second upper molar tooth
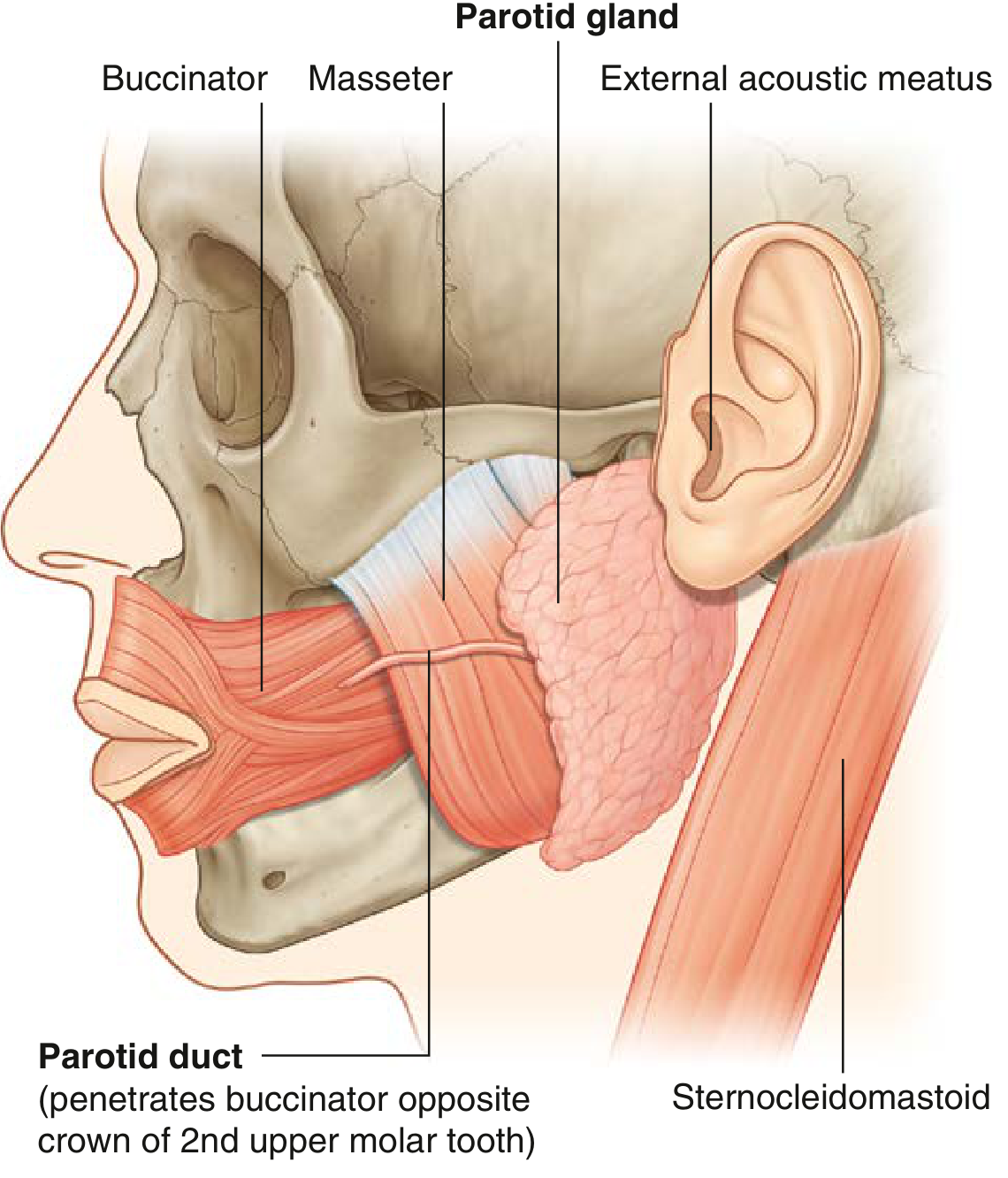
Fig. B - Parotid duct penetrating buccinator opposite the crown of the 2nd upper molar tooth
Structures Passing Through the Parotid Gland
Three major structures pass through (from superficial to deep - "FAR" mnemonic: Facial nerve, Artery (external carotid), Retromandibular vein):
1. Facial Nerve [VII] (most superficial)
- Exits skull via the stylomastoid foramen
- Enters the posterior surface of the gland and typically divides into upper (temporofacial) and lower (cervicofacial) trunks
- Further branches into five terminal groups that emerge from the borders of the gland:
- Temporal - from upper border
- Zygomatic - from upper border
- Buccal - from anterior border
- Marginal mandibular - from lower border
- Cervical - from lower border
2. External Carotid Artery (middle layer)
- Enters the inferior border of the gland
- Gives off the posterior auricular artery before dividing into two terminal branches within/just below the gland:
- Maxillary artery - passes horizontally deep to the mandible
- Superficial temporal artery - ascends, gives off the transverse facial artery, and emerges from the upper border
3. Retromandibular Vein (deepest)
- Formed within the gland by the union of the superficial temporal vein and maxillary vein
- Descends through the gland
- Divides just below the inferior border into:
- Anterior branch - joins the facial vein to form the common facial vein
- Posterior branch - joins the posterior auricular vein to form the external jugular vein
Nerve Supply
Secretomotor (Parasympathetic) - the important pathway:
| Step | Structure |
|---|---|
| Preganglionic origin | Inferior salivatory nucleus (medulla) |
| Nerve | Glossopharyngeal nerve [IX] → tympanic branch (Jacobson's nerve) → tympanic plexus → lesser petrosal nerve |
| Ganglion | Otic ganglion (just below foramen ovale) |
| Postganglionic fibers | Travel with the auriculotemporal nerve (branch of V3) to the gland |
Sensory
- Auriculotemporal nerve (branch of mandibular nerve V3) - also carries the postganglionic parasympathetic secretomotor fibers
Sympathetic (vasomotor)
- Postganglionic fibers from the superior cervical sympathetic ganglion, travelling along the external carotid artery plexus
Blood Supply
- Arterial: Branches from the arteries passing through the gland (external carotid, superficial temporal, transverse facial arteries)
- Venous: Via retromandibular vein and its tributaries
Lymphatic Drainage
Drains into:
- Superficial parotid (preauricular) lymph nodes (within parotid fascia)
- Deep parotid lymph nodes (within the gland substance)
- These drain to the deep cervical lymph nodes
Accessory Parotid Gland
A small detached portion of parotid tissue that lies along the parotid duct anterior to the main gland, overlying the masseter muscle. Present in ~20% of individuals. About 1% of parotid tumors arise here.
Clinical Relevance
| Condition | Key Points |
|---|---|
| Parotitis (Mumps) | Viral infection causing painful swelling of the parotid; trismus due to stretching of the parotid fascia |
| Parotid calculus (sialolithiasis) | Stone in parotid duct → pain on salivation, swelling; lemon juice test positive |
| Parotid tumors | 80% benign; most common = pleomorphic adenoma (mixed tumor); second = Warthin's tumor (adenolymphoma) |
| Frey's syndrome | Post-parotidectomy gustatory sweating - aberrant regeneration of auriculotemporal parasympathetic fibers to sweat glands of skin |
| Parotidectomy | Facial nerve must be identified and preserved; division of the nerve during surgery causes facial palsy |
| Mumps complications | Orchitis, oophoritis, meningitis, pancreatitis, sensorineural hearing loss |
Important Anatomical Points (Exam Focus)
- The parotid is the only salivary gland to have lymph nodes within it - explains why metastatic nodes can present as a parotid swelling
- The facial nerve divides the gland into superficial and deep lobes - it is the key surgical landmark in parotidectomy
- The parotid duct opens opposite the 2nd upper molar (not 1st or 3rd)
- Frey's syndrome after parotidectomy is due to aberrant innervation via the auriculotemporal nerve
- The parotid fascia is dense (unlike other salivary gland capsules) - hence parotitis is extremely painful (no room to expand)
- The parotid is the site of the largest proportion of salivary gland tumors (~70% of all salivary gland tumors occur here)
Sources: Gray's Anatomy for Students (9780323934237); Scott-Brown's Otorhinolaryngology Head & Neck Surgery (9781138094642)
This is a shared conversation. Sign in to Orris to start your own chat.