BIMALLEOLAR FRACTURE
Reading File
Finding Sources
Finding Sources
Searching PubMed
"bimalleolar fracture" AND treatment
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from Campbell's Operative Orthopaedics (2026), Rockwood & Green's (2025), Tintinalli's Emergency Medicine, and Rosen's Emergency Medicine to compile a thorough answer.
Bimalleolar Fracture
Definition
A bimalleolar fracture is a fracture of both the medial and lateral malleoli of the ankle. It disrupts the medial and lateral stabilizing structures of the ankle joint simultaneously, making it an inherently unstable injury. The ankle is viewed as a ring of bone and ligaments around the talus; two-component ring disruptions are characteristically unstable and typically require surgical fixation.
Radiographic Appearance
Figure 276-12 - Bimalleolar Fracture (Tintinalli's Emergency Medicine)
AP view:

Lateral view:

Mechanism and Biomechanics
Displacement of both malleoli:
- Reduces the tibiotalar contact area
- Alters joint kinematics
- Allows the talus to displace laterally and rotate externally within the mortise
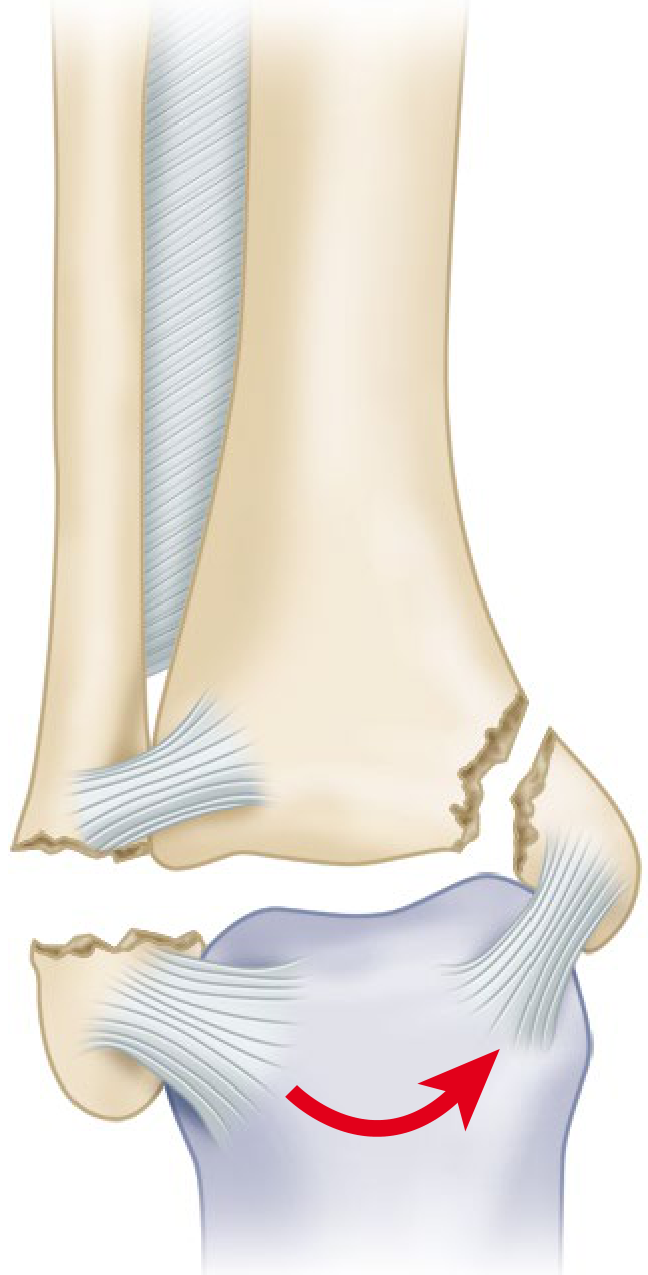
The most common mechanism is supination with external rotation (SER stage IV in Lauge-Hansen), producing an oblique fibular fracture plus a medial malleolar fracture (or deltoid ligament tear - a "bimalleolar equivalent").
The illustration below shows the ankle at the time of fracture with talar displacement:
Classification
Danis-Weber Classification (most commonly used clinically)
Based on the level of fibular fracture relative to the syndesmosis:
| Type | Fibular Fracture Level | Mechanism | Syndesmosis |
|---|---|---|---|
| A | Below the plafond/syndesmosis | Internal rotation + adduction | Intact |
| B | At the level of syndesmosis | External rotation | Variable (may be disrupted) |
| C | Above the syndesmosis | Abduction (C-1) or abduction + external rotation (C-2) | Disrupted |
~80-90% of lateral malleolar fractures are type B. Interobserver reliability: 78%; intraobserver: 85%.
Lauge-Hansen Classification
Based on foot position + deforming force at time of injury:
| Pattern | Abbreviation | Frequency |
|---|---|---|
| Supination-External Rotation | SER | ~60% |
| Supination-Adduction | SAD | ~20% |
| Pronation-Abduction | PAB | ~8% |
| Pronation-External Rotation | PER | ~12% |
Bimalleolar fractures most commonly result from SER stage IV (oblique fibular fracture + medial malleolar fracture or deltoid ligament disruption).
Note: Neither classification has proven prognostic significance, and Lauge-Hansen has demonstrated limitations in predicting soft-tissue injuries on MRI.
Key Clinical Points
- 20% of bimalleolar fractures involve intraarticular injuries to the talus and tibia that go untreated when closed methods are used
- Nonunion rate with closed treatment: ~10% (not always symptomatic)
- Randomized, prospective, long-term studies show superior results with operative over nonoperative treatment
- Closed reduction can often be achieved but not maintained as swelling subsides
Treatment
Emergency Management
- Posterior splint + stirrup application - keep non-weight bearing
- If fracture-dislocation present: immediate closed reduction is mandatory to prevent skin necrosis, even if definitive ORIF is delayed
- Analgesics, elevation, and ice
- Urgent orthopedic consultation
Operative Timing
ORIF can be performed within the first 12 hours, or delayed 2-3 weeks until swelling subsides. Equally good functional results have been shown with both immediate and delayed ORIF of Weber B bimalleolar fractures, though immediate surgery offers shorter hospitalization and less pain in some studies.
Delayed surgery is justified when there is:
- Severe closed soft-tissue injury
- Fracture blisters present
ORIF Technique (Campbell's Technique 59.1)
The standard approach is ORIF of both malleoli:
1. Lateral Malleolus (usually fixed first):
- Lateral longitudinal incision; protect the superficial peroneal nerve
- Oblique fracture: 1-2 lag screws (anterior to posterior), 1 cm apart
- Transverse fracture: intramedullary device (titanium elastic nail, interlocking rod, or malleolar screw)
- Standard fixation: one-third semitubular 3.5-mm plate and screws
- Posterior antiglide technique for Weber B fractures (avoids intraarticular screws, less palpable implants, stronger construct)
- Exception: if lateral comminution is severe, fix the medial malleolus first to avoid over-reduction inhibiting anatomic medial reduction
Fixation options for lateral malleolar fractures (Campbell's Figure 59.3):
- Plate and screws (standard)
- Multiple lag screws (simple oblique fractures, patients <50y, minimal comminution)
- Intramedullary screw
- Tension band wiring
2. Medial Malleolus:
- Two 4-mm cancellous lag screws perpendicular to the fracture (or bicortical 3.5-mm screws for increased construct strength)
- Small fragments: one lag screw + one K-wire to prevent rotation
- Comminuted/too-small fragments: two K-wires + tension band
- Vertical fractures: horizontally directed screws or antiglide plate
AO fixation technique (Figure 59.6): Drill 3.2-mm hole, measure length, insert malleolar screw without tapping while fragment is held reduced with bent K-wires.
Syndesmotic Assessment
- If the fibular fracture is above the level of the distal tibiofibular joint (Weber C), the syndesmosis is assumed disrupted and must be anatomically reduced
- Syndesmotic fixation may not be required if there is no medial injury, but disruptions extending >4.5 cm proximal to the ankle joint alter joint mechanics when a medial lesion is present
Postoperative Care
- Ankle immobilized in posterior plaster splint in neutral position, elevated
- Good bone quality + secure fixation: splint removed at first visit, replaced with removable splint or fracture boot; range-of-motion exercises begun
- Weight bearing restricted for 6 weeks (without syndesmotic injury), then progressive partial weight bearing if healing progressing well
- Poor bone quality / comorbidities (diabetes, neuropathy): short-leg cast, non-weight bearing 8-12 weeks
- Multiple studies are evaluating potential benefits of early weight bearing after ankle fixation
Bimalleolar Equivalent Fracture
A deltoid ligament tear + lateral malleolar fracture is mechanically equivalent to a bimalleolar fracture (same supination-external rotation mechanism). The deep deltoid ligament prevents lateral displacement and external rotation of the talus. Treatment is the same - ORIF of the lateral malleolus, with repair of the medial ligamentous complex if significant medial instability persists after lateral fixation.
Complications
- Nonunion (~10% with closed treatment)
- Intraarticular injury to talus/tibia (20%) - missed with closed management
- Wound complications - particularly over medial malleolus (poor skin coverage)
- Implant prominence - lateral plate symptomatic in some; only ~50% relief after removal
- Peroneal tendon injury (30% after posterior plate implant removal)
- Peroneal tendinitis (transient, with posterior antiglide plating)
- Compartment syndrome - rare, with severe comminuted injuries
- Post-traumatic arthritis - results generally inferior to trimalleolar fractures
Sources: Campbell's Operative Orthopaedics 15th Ed 2026, pp. 3322-3328; Rockwood and Green's Fractures in Adults 10th Ed 2025, p. 3297; Tintinalli's Emergency Medicine, p. 1910
This is a shared conversation. Sign in to Orris to start your own chat.