Why is anticholinergic drug not used in acg
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a thorough explanation, backed by multiple textbooks:
Why Anticholinergic Drugs Are Contraindicated in Acute Angle-Closure Glaucoma (ACG)
The Core Mechanism: Pupillary Dilation Triggers Angle Closure
The fundamental problem in ACG is that the peripheral iris physically blocks the trabecular meshwork, preventing aqueous humor from draining out of the anterior chamber. This causes a rapid, dangerous rise in intraocular pressure (IOP).
The entire chain of events hinges on pupillary dilation (mydriasis). Anticholinergic drugs block muscarinic receptors in the iris sphincter muscle, causing the sphincter to relax. This allows the dilator muscle to dominate, producing mydriasis.
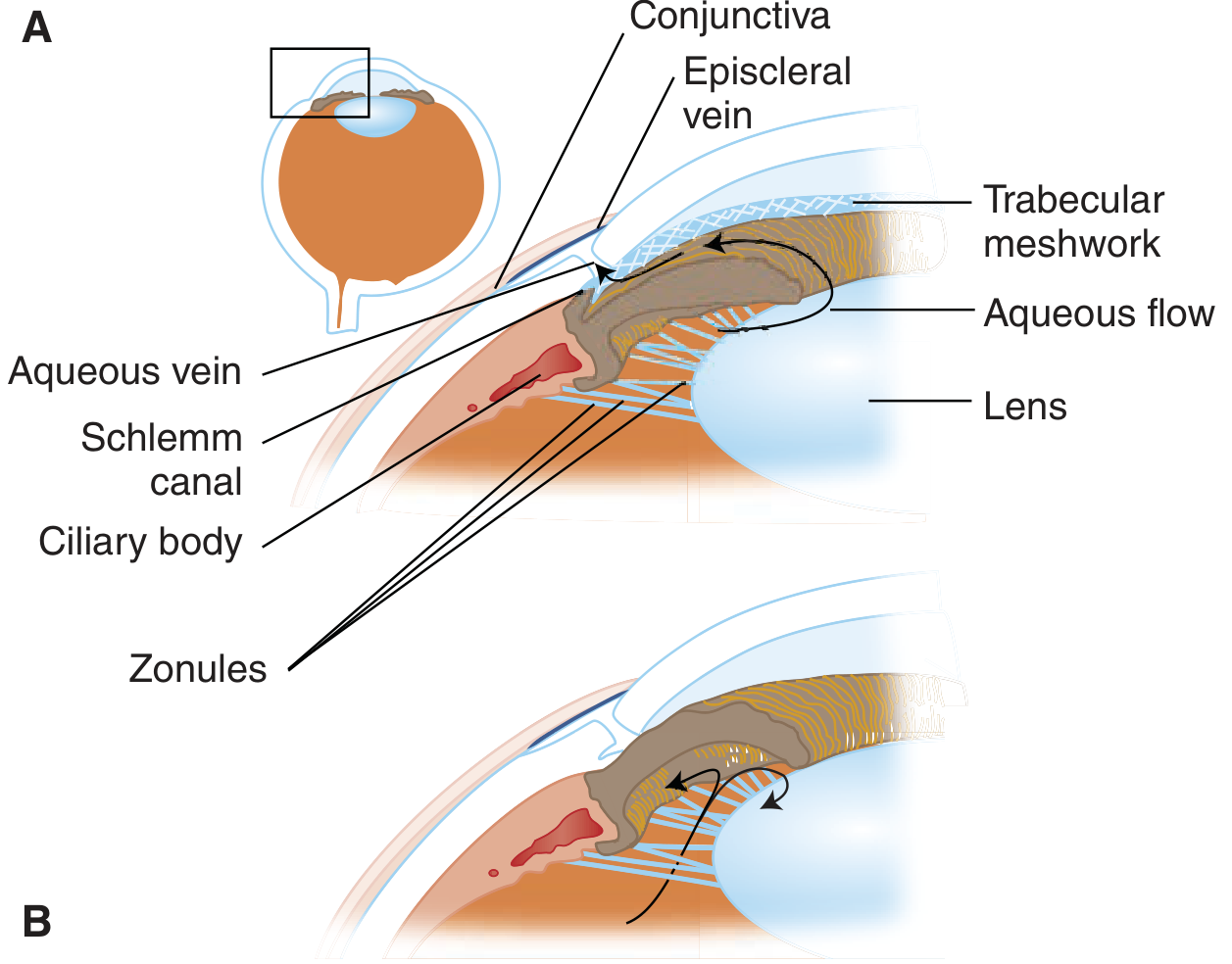
A = normal aqueous outflow through trabecular meshwork. B = angle-closure: the iris bows forward, blocks the angle, and aqueous cannot drain.
Step-by-Step Pathophysiology
-
Anatomical predisposition: Some eyes have a shallow anterior chamber with a narrow angle between the cornea and iris. In these eyes, the lens and iris are already in closer contact than normal.
-
Anticholinergic drug administered: The drug (e.g., atropine, ipratropium, antihistamines, tricyclic antidepressants, scopolamine) blocks the iris sphincter → pupil dilates (mydriasis).
-
Mid-dilation is the danger zone: When the pupil is mid-dilated, two things happen simultaneously:
- The iris becomes thicker and bulkier, increasing contact area between the iris and lens.
- The peripheral iris has maximum laxity, allowing it to bow forward easily.
-
Pupillary block develops: The thickened iris presses tightly against the lens, acting like a ball-valve. Aqueous humor produced in the posterior chamber cannot pass through the pupil into the anterior chamber.
-
Iris bombé: Pressure builds behind the iris, pushing it forward - a condition called iris bombé. The peripheral iris root is thrust against the trabecular meshwork, closing the filtration angle completely.
-
IOP spikes dramatically: With outflow blocked and aqueous continuing to be produced, IOP rises precipitously - often to 40-80 mmHg (normal is ~10-21 mmHg).
-
Corneal edema and vision loss: The high IOP overwhelms the corneal pump mechanism, causing corneal edema and the characteristic foggy vision, halos around lights, and a hazy cornea on exam.
As Goodman & Gilman explains: "Anticholinergic, sympathomimetic, and antihistaminic drugs can lead to partial dilation of the pupil and a change in the force vectors between the iris and the lens. The aqueous humor is prevented from passing from the posterior chamber through the pupil to the anterior chamber through a ball (lens)-valve (pupil) type mechanism... The iris root is pushed against the angle wall, thereby covering the trabecular meshwork, closing the filtration angle, and markedly elevating IOP." - Goodman & Gilman's Pharmacological Basis of Therapeutics
Why Normal (Open-Angle) Glaucoma Is Different
In open-angle glaucoma, the drainage angle remains physically open. The problem is resistance within the trabecular meshwork itself. Anticholinergics do not acutely block a patent angle, so they are not contraindicated in the same way (though they can still be problematic).
In angle-closure glaucoma, the angle is already anatomically narrow - any mydriasis can mechanically seal it shut.
Which Anticholinergic Drugs Pose This Risk?
| Drug Class | Examples |
|---|---|
| Classic anticholinergics | Atropine, scopolamine, hyoscine |
| Antihistamines (1st gen) | Diphenhydramine, chlorpheniramine |
| Inhaled bronchodilators | Ipratropium (in nebulized combination with albuterol) |
| Tricyclic antidepressants | Amitriptyline, imipramine |
| Antiparkinsonian agents | Benztropine, trihexyphenidyl |
| Antipsychotics (with anticholinergic effect) | Chlorpromazine |
| Antispasmodics | Oxybutynin, propantheline |
As noted in Adams & Victor's Principles of Neurology, the presence of angle-closure glaucoma is explicitly listed as a contraindication to anticholinergic use in Parkinson's disease treatment.
Key Summary
| Factor | Effect |
|---|---|
| Anticholinergic drug | Blocks iris sphincter (M3 receptor) |
| Result | Pupillary dilation (mydriasis) |
| In narrow-angle eye | Iris becomes thick, bows forward (iris bombé) |
| Angle | Mechanically sealed shut by peripheral iris |
| Aqueous outflow | Blocked - IOP rises acutely |
| Consequence | Acute angle-closure attack - optic nerve damage, vision loss |
In short: Anticholinergics cause mydriasis, mydriasis causes iris bombé, and iris bombé seals the already-narrow drainage angle - converting a predisposed eye into a full-blown acute glaucoma emergency. This is why they are contraindicated in ACG. - Tintinalli's Emergency Medicine & Goodman & Gilman's Pharmacological Basis of Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.