Counter current mechanism 10m
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I have all the content I need. Let me now write the comprehensive answer.
Countercurrent Mechanism
The countercurrent mechanism is the renal process that creates and maintains a hyperosmotic medullary interstitium, enabling the kidney to produce concentrated urine. It involves two distinct but related processes: countercurrent multiplication (by the loop of Henle) and countercurrent exchange (by the vasa recta), plus a supporting role from urea recycling.
Overview
A countercurrent system is one in which inflow runs parallel to, counter to, and in close proximity to the outflow. This arrangement exists in both the loop of Henle and the vasa recta in the renal medulla. The final gradient achieved creates a corticopapillary osmotic gradient from ~300 mOsm/L at the cortex to ~1200-1400 mOsm/L at the tip of the papilla.
- Ganong's Review of Medical Physiology, 26e, p.687
- Guyton and Hall Textbook of Medical Physiology, p.373
Part 1: Countercurrent Multiplication (Loop of Henle)
This is an active process that establishes the corticopapillary gradient. It depends on three structural/functional properties of the loop of Henle:
| Segment | Water Permeability | Active NaCl Transport | Notes |
|---|---|---|---|
| Thin descending limb | High (via aquaporin-1) | None | Water freely exits |
| Thin ascending limb | Zero | None | Passive NaCl exit |
| Thick ascending limb | Zero | High | Na⁺-K⁺-2Cl⁻ cotransport |
The "Single Effect"
The key pump is the Na⁺-K⁺-2Cl⁻ cotransporter in the thick ascending limb (TAL). It actively transports NaCl from tubular lumen into the medullary interstitium. Because the TAL is impermeable to water, water cannot follow - the tubular fluid in the ascending limb becomes dilute while the interstitium becomes concentrated. This single effect establishes a 200 mOsm/L gradient at any given cross-sectional level.
The descending limb, being permeable to water, equilibrates with the concentrated interstitium - water leaves the descending limb and its osmolarity rises.
- Costanzo Physiology, 7e, p.306
Stepwise Multiplication
The gradient is amplified by the continuous flow of fluid. Illustrating in steps (starting at 300 mOsm/L throughout):
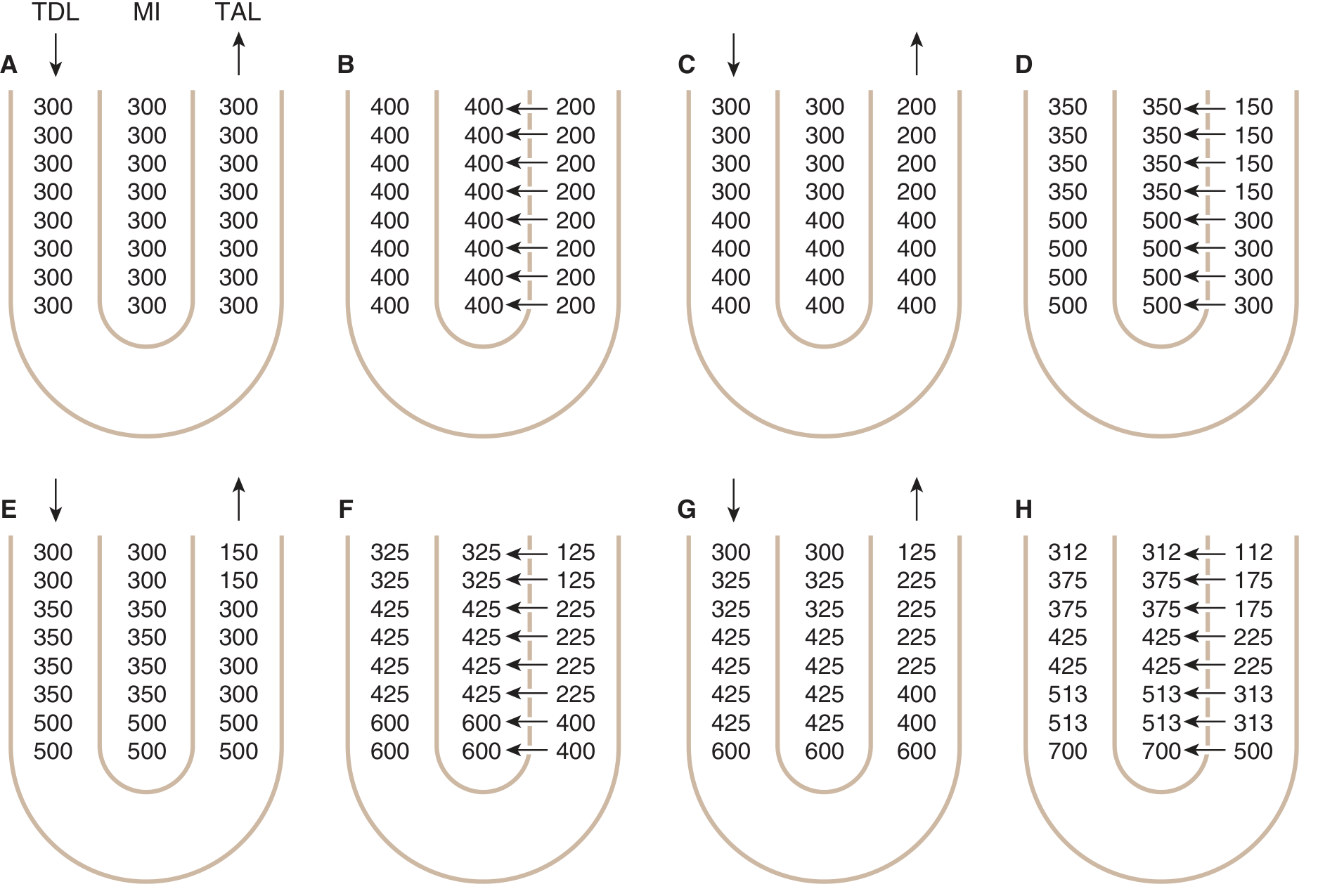
TDL = thin descending limb; MI = medullary interstitium; TAL = thick ascending limb. Panels A-H show progressive cycles of single effect + fluid flow multiplying the axial gradient.
Step 1 (Single Effect): NaCl is pumped from TAL → interstitium. Interstitial osmolarity rises to 400 mOsm/L; descending limb equilibrates to 400 mOsm/L; ascending limb dilutes to 200 mOsm/L.
Step 2 (Flow of fluid): New 300 mOsm/L fluid enters from proximal tubule, pushing the high-osmolarity fluid in the descending limb down toward the bend of the loop. The corticopapillary gradient begins to emerge.
Step 3 (Single Effect again): NaCl is pumped out again. The gradient at each level is further increased.
Step 4 (Flow again): Further displacement of hyperosmolar fluid toward the tip.
These two steps repeat cyclically. Because each cycle multiplies the axial gradient, the final result is a progressive osmolarity increase from cortex to papilla, reaching ~1200 mOsm/L at the hairpin bend of juxtamedullary nephrons. In desert rodents with longer loops, this can reach 3000 mOsm/L.
- Costanzo Physiology, 7e, pp.306-307; Ganong's 26e, p.687; Guyton and Hall, pp.373-374
Key point: The longer the loop of Henle, the steeper the corticopapillary gradient. This is why juxtamedullary nephrons (with long loops dipping into the deep papilla) are critical - only ~25% of nephrons are juxtamedullary, but they generate the gradient.
Part 2: Urea Recycling
Urea recycling is the second mechanism contributing to the corticopapillary gradient, especially in the inner medulla. It depends on ADH:
- In the cortical and outer medullary collecting ducts, ADH increases water permeability but NOT urea permeability. Water is reabsorbed, but urea stays behind - so urea concentration in the tubular fluid progressively rises.
- When this concentrated tubular fluid reaches the inner medullary collecting duct, ADH activates urea transporter UT1, allowing facilitated diffusion of urea into the interstitium down its concentration gradient.
- This recycled urea enters thin limbs of the loop of Henle and circulates back, adding to the medullary osmolarity.
- When ADH is absent (e.g., central diabetes insipidus), urea recycling does not occur and the corticopapillary gradient is diminished.
ADH thus enhances the gradient by two mechanisms: stimulating Na⁺-K⁺-2Cl⁻ cotransport (amplifying the single effect) AND enabling urea recycling into the inner medulla.
- Costanzo Physiology, 7e, pp.307-308
Part 3: Countercurrent Exchange (Vasa Recta)
The vasa recta are U-shaped capillaries that parallel the loops of Henle. They carry only ~5% of total renal blood flow, keeping medullary flow very slow.
Key difference from multiplication:
- Countercurrent multiplication = active process that establishes the gradient
- Countercurrent exchange = passive process that maintains the gradient
The vasa recta are freely permeable to both water and small solutes. As blood flows down the descending vasa recta into the increasingly hyperosmotic medulla:
- Solutes (NaCl, urea) diffuse in from the interstitium
- Water diffuses out into the interstitium
- Blood becomes progressively more concentrated
As blood flows up the ascending vasa recta back toward the cortex:
- Solutes diffuse out back into the interstitium
- Water diffuses in back from the interstitium
- Blood osmolarity returns toward normal
The solutes picked up on the way down are returned to the medulla on the way up - trapping solutes in the medulla rather than washing them out. This is why slow blood flow through the vasa recta is essential: if it were fast, solutes would be washed away and the gradient would collapse.
- Costanzo Physiology, 7e, pp.308-309
How Concentrated Urine is Actually Formed
The corticopapillary osmotic gradient alone doesn't concentrate urine - ADH is required:
| ADH Level | Collecting Duct Permeability | Urine |
|---|---|---|
| High (e.g., dehydration) | High (aquaporins inserted) | Water reabsorbed → concentrated urine (up to 1200 mOsm/L) |
| Low (e.g., water loading) | Low | Water stays in tubule → dilute urine (as low as 50 mOsm/L) |
The gradient built by the loop acts as a "standing osmotic gradient" - ADH determines how much water the collecting duct extracts from it.
Summary Table
| Component | Process Type | Function |
|---|---|---|
| Thick ascending limb (TAL) | Active (Na⁺-K⁺-2Cl⁻ pump) | Single effect; deposits NaCl in interstitium |
| Thin descending limb | Passive (water permeable) | Water exits; tubular fluid concentrates |
| Loop flow (countercurrent) | Geometric amplification | Multiplies single effect into axial gradient |
| Inner medullary collecting duct + ADH | Facilitated diffusion (UT1) | Urea recycling; contributes ~500 mOsm/L at tip |
| Vasa recta | Passive exchange | Maintains gradient; prevents washout |
| ADH + collecting duct | Osmosis | Translates gradient into actual urine concentration |
Key drugs affecting this mechanism:
-
Loop diuretics (furosemide): block Na⁺-K⁺-2Cl⁻ in TAL → abolish single effect → flatten gradient → inability to concentrate urine
-
ADH analogs (desmopressin): restore collecting duct permeability in central DI
-
Lithium/demeclocycline: cause nephrogenic DI by blocking ADH action on collecting duct
-
Guyton and Hall Textbook of Medical Physiology, p.374; Costanzo Physiology, 7e, pp.306-309; Ganong's Review of Medical Physiology, 26e, pp.687-688
This is a shared conversation. Sign in to Orris to start your own chat.