I now have comprehensive information to construct a detailed answer on AUB as per DC Dutta's framework. Note that DC Dutta is not in the library, but I have excellent content from Berek & Novak's Gynecology and Sabiston, which align with DC Dutta's teaching framework. Let me now compile the full detailed answer.
Abnormal Uterine Bleeding (AUB) - As per DC Dutta's Framework
Note: DC Dutta's Textbook of Gynecology is not in the library database. However, the content below is compiled from Berek & Novak's Gynecology and Sabiston Textbook of Surgery, which cover exactly the same framework DC Dutta uses (PALM-COEIN classification, older DUB terminology, investigation, and management). The DC Dutta-specific nuances from his textbook are supplemented from my training knowledge.
Definition
Abnormal Uterine Bleeding (AUB) refers to any bleeding from the uterine corpus that is abnormal in regularity, frequency, duration, or volume in a non-pregnant woman of reproductive age.
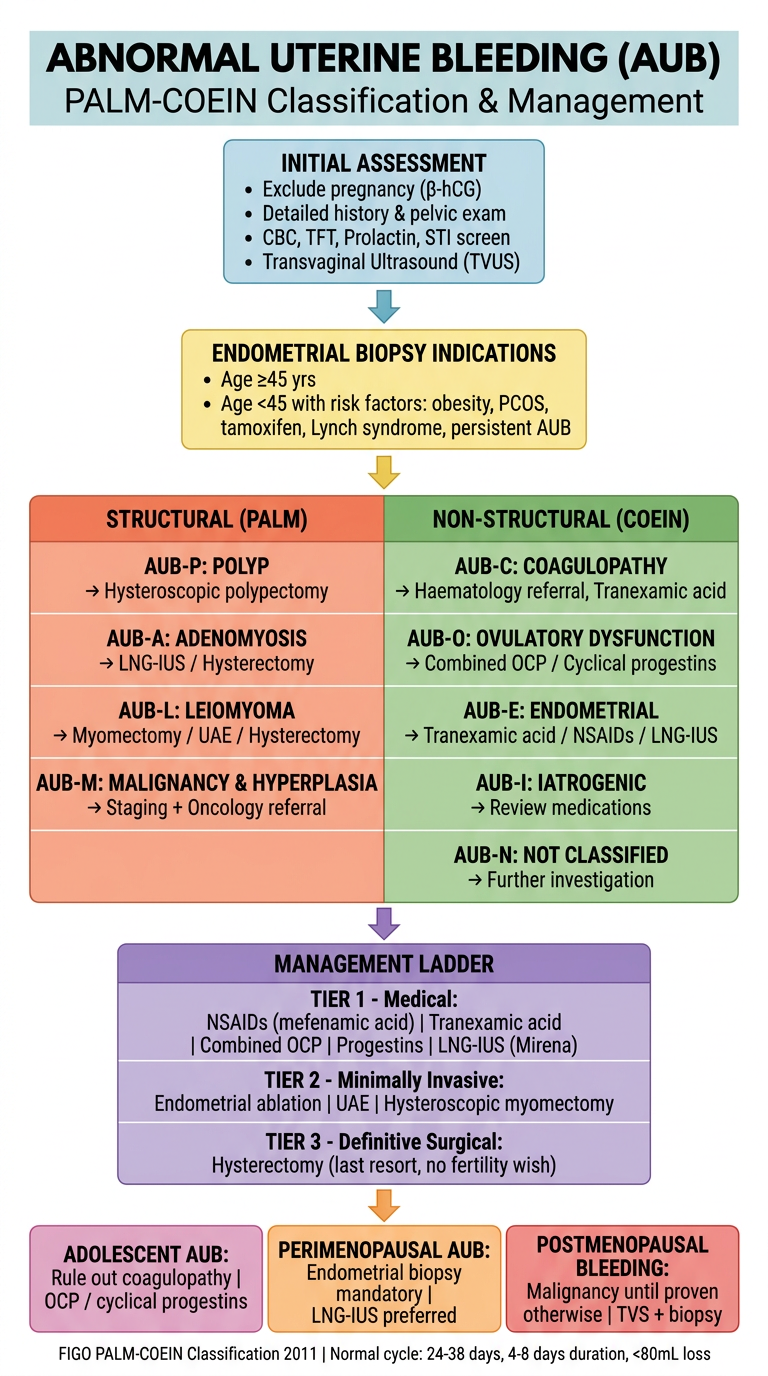
- Normal menstrual cycle: 24-38 days frequency
- Normal duration of flow: 4-8 days
- Normal blood loss: <80 mL per cycle
Previously used terms like menorrhagia, metrorrhagia, menometrorrhagia, and dysfunctional uterine bleeding (DUB) have now been replaced by the FIGO PALM-COEIN classification (since 2011). DC Dutta's older editions used DUB extensively, while newer editions incorporate PALM-COEIN.
Menstrual Terminology (DC Dutta)
| Term | Definition |
|---|
| Menorrhagia | Heavy and/or prolonged bleeding at regular intervals (>80 mL or >7 days) |
| Metrorrhagia | Irregular bleeding between regular periods |
| Menometrorrhagia | Frequent, heavy, and irregular bleeding |
| Polymenorrhoea | Frequent bleeding at intervals <21 days |
| Oligomenorrhoea | Infrequent periods at intervals >35 days |
| Intermenstrual bleeding (IMB) | Bleeding between regular periods |
| Postcoital bleeding (PCB) | Bleeding after intercourse |
| Postmenopausal bleeding (PMB) | Bleeding >12 months after menopause |
PALM-COEIN Classification (FIGO 2011)
The current gold standard classification used in DC Dutta's recent editions:
Structural Causes - PALM
| Code | Cause |
|---|
| AUB-P | Polyp (endometrial/cervical) |
| AUB-A | Adenomyosis |
| AUB-L | Leiomyoma (submucosal, SM; other, O) |
| AUB-M | Malignancy and hyperplasia |
Non-structural Causes - COEIN
| Code | Cause |
|---|
| AUB-C | Coagulopathy |
| AUB-O | Ovulatory dysfunction |
| AUB-E | Endometrial (primary disorder) |
| AUB-I | Iatrogenic |
| AUB-N | Not yet classified |
Each Cause in Detail
AUB-P: Polyps
- Endometrial polyps are overgrowths of endometrial glands and stroma (sessile or pedunculated)
- Causes: intermenstrual bleeding, heavy menstrual bleeding, postmenopausal bleeding, and rarely dysmenorrhea
- Associated with: tamoxifen use, obesity, hypertension, PCOS, increasing age
- Incidence increases with age throughout the reproductive years
- Malignant transformation: up to 5% of polyps; risk higher in postmenopausal women (0% to 13% malignancy; 0.2% to 24% premalignant change)
- Diagnosis: transvaginal ultrasound (endometrial thickening), sonohysterography, hysteroscopy
- Treatment: hysteroscopic polypectomy; smaller polyps may regress spontaneously (27% at 1 year)
- (Berek & Novak's Gynecology)
AUB-A: Adenomyosis
- Endometrial glands and stroma within the myometrium
- Presents with heavy menstrual bleeding, dysmenorrhea, and an enlarged, globular, tender uterus
- Diagnosis: MRI (most accurate); ultrasound shows heterogeneous myometrium
- Treatment: Medical (progestins, LNG-IUS, NSAIDs); Definitive - hysterectomy
AUB-L: Leiomyoma (Fibroids)
- Most common benign gynecologic tumor; affects up to 70% of patients by age 50
- Higher prevalence and severity in Black patients (earlier onset, more numerous, larger)
- FIGO classification by location:
- Type 0: Pedunculated intracavitary
- Types 1-2: Submucosal
- Types 3-5: Intramural
- Types 6-7: Subserosal
- Type 8: Cervical
- Submucosal fibroids (types 0, 1, 2) are most likely to cause AUB
- Diagnosis: Pelvic ultrasound, saline infusion sonography, MRI
- Treatment: Hysteroscopic myomectomy (submucosal), abdominal/laparoscopic myomectomy, uterine artery embolization (UAE), GnRH agonists, hysterectomy
- (Sabiston Textbook of Surgery)
AUB-M: Malignancy and Hyperplasia
- Endometrial hyperplasia (with or without atypia) and endometrial carcinoma
- Non-structural causes include the COEIN group; structural causes include PALM
- Endometrial biopsy is mandatory for:
- All women ≥45 years with AUB
- Women <45 with risk factors: obesity, anovulation, unopposed estrogen, family history of Lynch syndrome
- 90% of patients with endometrial cancer present with abnormal uterine bleeding
- (Sabiston Textbook of Surgery)
AUB-C: Coagulopathy
- Coagulation disorders account for a significant proportion of heavy menstrual bleeding
- von Willebrand disease is the most common inherited coagulation disorder causing AUB
- Others: thrombocytopenia, platelet function disorders, factor deficiencies
- Screen if: heavy bleeding since menarche, family history of coagulopathy, signs of systemic bleeding (easy bruising, nosebleeds), anticoagulant use
- (Berek & Novak's Gynecology)
AUB-O: Ovulatory Dysfunction
- Anovulatory cycles are the most common cause of AUB in reproductive age women
- Causes of anovulation:
- PCOS (most common in reproductive age)
- Thyroid disorders (hypothyroidism / hyperthyroidism)
- Hyperprolactinemia
- Hypothalamic dysfunction (stress, exercise, weight loss)
- Perimenopause
- Mechanism: Lack of progesterone leads to unopposed estrogen stimulation of the endometrium, causing irregular shedding and heavy bleeding
- DC Dutta's older editions classified most of these as DUB (Dysfunctional Uterine Bleeding)
- (Berek & Novak's Gynecology)
DC Dutta's DUB Classification (Historical - still exam-relevant):
| Type | Feature |
|---|
| Anovulatory DUB (75-80%) | No ovulation; no corpus luteum; unopposed estrogen; common in adolescents and perimenopausal women |
| Ovulatory DUB (20-25%) | Ovulation occurs; luteal phase defect or irregular ripening; typically in reproductive age |
AUB-E: Endometrial Causes
- Primary disorders of the endometrium in the absence of other identifiable causes
- Includes disorders of:
- Endometrial hemostasis (deficient local vasoconstriction)
- Prostaglandin balance (increased PGE2/PGI2 relative to PGF2-alpha)
- Fibrinolysis (increased endometrial fibrinolytic activity)
- These are essentially ovulatory women with heavy periods but no structural cause
AUB-I: Iatrogenic
- Bleeding caused by medications:
- Exogenous hormones: OCP (breakthrough bleeding), progestin-only pills, implants, DMPA
- LNG-IUS: irregular spotting especially in first 3-6 months
- Anticoagulants: warfarin, heparin, NOACs
- Copper IUD: increases menstrual blood loss
- Tamoxifen: endometrial stimulation
- Antipsychotics/dopamine antagonists: hyperprolactinemia causing anovulation
AUB-N: Not Yet Classified
- AVM (arteriovenous malformations) of the uterus
- Myometrial hypertrophy
- Endometritis (chronic)
Investigations
Step 1 - Basic Workup (all patients)
- Detailed history - cycle characteristics, contraceptive use, medications, systemic illness
- Pelvic examination - size/shape of uterus, adnexal masses, cervical lesions
- Urine/serum β-hCG - exclude pregnancy
- CBC - hemoglobin (to assess blood loss), platelet count
- Thyroid function tests (TSH)
- Prolactin level
- Cervical smear (if not up to date)
- STI screening (chlamydia, gonorrhoea) in at-risk patients
Step 2 - Imaging
- Transvaginal ultrasound (TVUS): First-line imaging; assesses endometrial thickness, fibroids, polyps, ovarian pathology
- Saline infusion sonography (SIS)/Sonohysterography: Better than TVUS for intracavitary lesions
- MRI: Best for adenomyosis, leiomyoma mapping, deep infiltrating endometriosis
Step 3 - Endometrial Sampling
- Indications (DC Dutta / ACOG):
- Age ≥45 years
- Age <45 with: obesity, PCOS, anovulation, tamoxifen use, Lynch syndrome, persistent AUB refractory to medical treatment
- Pipelle biopsy - office-based; 90-95% sensitivity for endometrial cancer
- Dilatation & Curettage (D&C) - if Pipelle fails; also diagnostic and sometimes therapeutic
- Hysteroscopy + biopsy - gold standard; allows directed biopsy of focal lesions
Step 4 - Coagulation Screen (selected cases)
- PT, APTT, platelet count
- Von Willebrand factor antigen and activity
- Bleeding time
Management
Principles (DC Dutta Framework)
Management depends on:
- Age and reproductive wishes
- Severity of bleeding
- Underlying etiology
- Medical fitness
Medical Management
1. Hormonal Therapy
| Drug | Mechanism | Use |
|---|
| Combined OCP | Suppresses endometrium, regulates cycle | Anovulatory AUB, AUB-O |
| Progestins (norethisterone, medroxyprogesterone) | Opposes estrogen, stabilizes endometrium | Anovulatory DUB, luteal defects |
| LNG-IUS (Mirena) | Local progestogen, atrophies endometrium | HMB, AUB-A, AUB-L; 1st-line for ovulatory HMB |
| GnRH agonists | Hypoestrogenic state, amenorrhoea | Fibroids (preoperative), AUB-L, bridge to surgery |
| Danazol | Androgenic, atrophies endometrium | Rarely used due to side effects |
2. Non-hormonal Therapy
| Drug | Mechanism | Use |
|---|
| Tranexamic acid | Antifibrinolytic | Heavy ovulatory bleeding; reduces blood loss by 40-50% |
| NSAIDs (mefenamic acid, naproxen) | Inhibit prostaglandins, reduce blood loss | Ovulatory AUB, dysmenorrhoea; reduces blood loss by 25-30% |
DC Dutta's Progesterone Regimen for DUB:
- Anovulatory DUB: Norethisterone 5 mg TDS from Day 5-25 of cycle (to impose cyclical withdrawal bleeding)
- Acute heavy bleeding: High-dose progestogens (norethisterone 5 mg TDS) or combined OCP to stop acute bleeding
Surgical Management
Indications for Surgery:
- Medical treatment failed or contraindicated
- Structural cause identified
- Patient does not wish to preserve fertility
- Suspected malignancy
Procedures:
1. Endometrial Ablation
- Destroys the endometrium
- 1st and 2nd generation techniques:
- 1st generation: rollerball, laser, wire loop (hysteroscopic)
- 2nd generation: thermal balloon (NovaSure), microwave, cryotherapy (office-based)
- Success rate: ~80% patient satisfaction; ~20-30% achieve amenorrhoea
- Important: Not appropriate if future pregnancy desired; must exclude endometrial cancer first
- 29% of patients who had ablation ultimately needed hysterectomy at 5 years (Berek & Novak's)
2. Uterine Artery Embolization (UAE)
- For symptomatic fibroids
- Non-surgical; fibroid infarction and shrinkage
- 31% ultimately required hysterectomy in long-term follow-up (Berek & Novak's)
- Preserves uterus but not recommended if future pregnancy desired
3. Myomectomy
- For women with symptomatic fibroids who want to preserve fertility
- Hysteroscopic (type 0-2 submucosal), laparoscopic, or open (abdominal)
4. Hysterectomy
- Definitive treatment; curative
- Reserved for:
- Failure of medical and conservative surgical treatment
- No desire for future fertility
- Confirmed or suspected malignancy
- Adenomyosis (definitive)
- Routes: vaginal, abdominal, laparoscopic, robotic
- Endometrial sampling must be done before hysterectomy for AUB
- D&C alone is not effective for controlling AUB long-term and is not necessary before hysterectomy (Berek & Novak's)
Special Situations (DC Dutta)
Adolescent AUB
- Most commonly due to anovulation (immature HPO axis)
- Rule out coagulopathy (von Willebrand disease) - especially if heavy since menarche
- Manage conservatively with hormones (OCP or cyclical progestins)
- Endometrial biopsy rarely needed
Perimenopausal AUB
- Most common cause: anovulatory cycles due to declining ovarian reserve
- Must always exclude endometrial hyperplasia/carcinoma
- Endometrial biopsy is mandatory
- LNG-IUS is an excellent option if no malignancy
Postmenopausal Bleeding
- Not part of PALM-COEIN (classified separately)
- Any postmenopausal bleeding = malignancy until proven otherwise
- Most common cause overall: endometrial atrophy
- Most dangerous cause: endometrial carcinoma (90% of endometrial cancer patients present with PMB)
- Workup: TVUS (endometrial thickness) + endometrial biopsy
- Endometrial thickness ≤4 mm: low risk; biopsy may be deferred
-
4 mm or focal lesion: endometrial biopsy mandatory
- Note: The 4 mm cutoff has been shown to underdiagnose endometrial cancer in Black patients (Sabiston)
Summary Algorithm
AUB in Reproductive Age
|
Exclude pregnancy
|
History + Exam + CBC + TFT + Prolactin + TVUS
|
Structural cause (PALM)? Non-structural (COEIN)?
| |
Polyp → polypectomy Anovulatory → hormones
Fibroid → medical/surgical Coagulopathy → haematology
Adenomyosis → LNG-IUS/Hx Iatrogenic → adjust meds
Malignancy → staging + Rx
Key DC Dutta High-Yield Points
- DUB (now AUB-O/E) is a diagnosis of exclusion - all organic causes must be ruled out first
- Anovulatory DUB is more common (75-80%); seen at extremes of reproductive life (adolescence + perimenopause)
- Ovulatory DUB is less common (20-25%); affects women in their 30s; regular but heavy periods
- The LNG-IUS (Mirena) is the most effective medical treatment for heavy menstrual bleeding with a uterine cause
- Tranexamic acid reduces blood loss by ~50% and is the best non-hormonal option for ovulatory HMB
- Endometrial biopsy before any surgical procedure for AUB
- D&C is diagnostic, not therapeutic for AUB (does not provide long-term relief)
- Postmenopausal bleeding: endometrial thickness ≤4 mm on TVS makes endometrial cancer very unlikely
- TVUS is the first-line imaging in all cases of AUB
Sources: Berek & Novak's Gynecology; Sabiston Textbook of Surgery, 21st Ed.; DC Dutta's Textbook of Gynecology (6th-9th Ed.) from training knowledge (not in library database)