Beta blockers
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
I now have comprehensive information from multiple authoritative textbooks. Let me compile a thorough answer.
Beta-Blockers (Beta-Adrenergic Receptor Antagonists)
Classification
Beta-blockers are categorized into three generations based on receptor selectivity and additional properties:
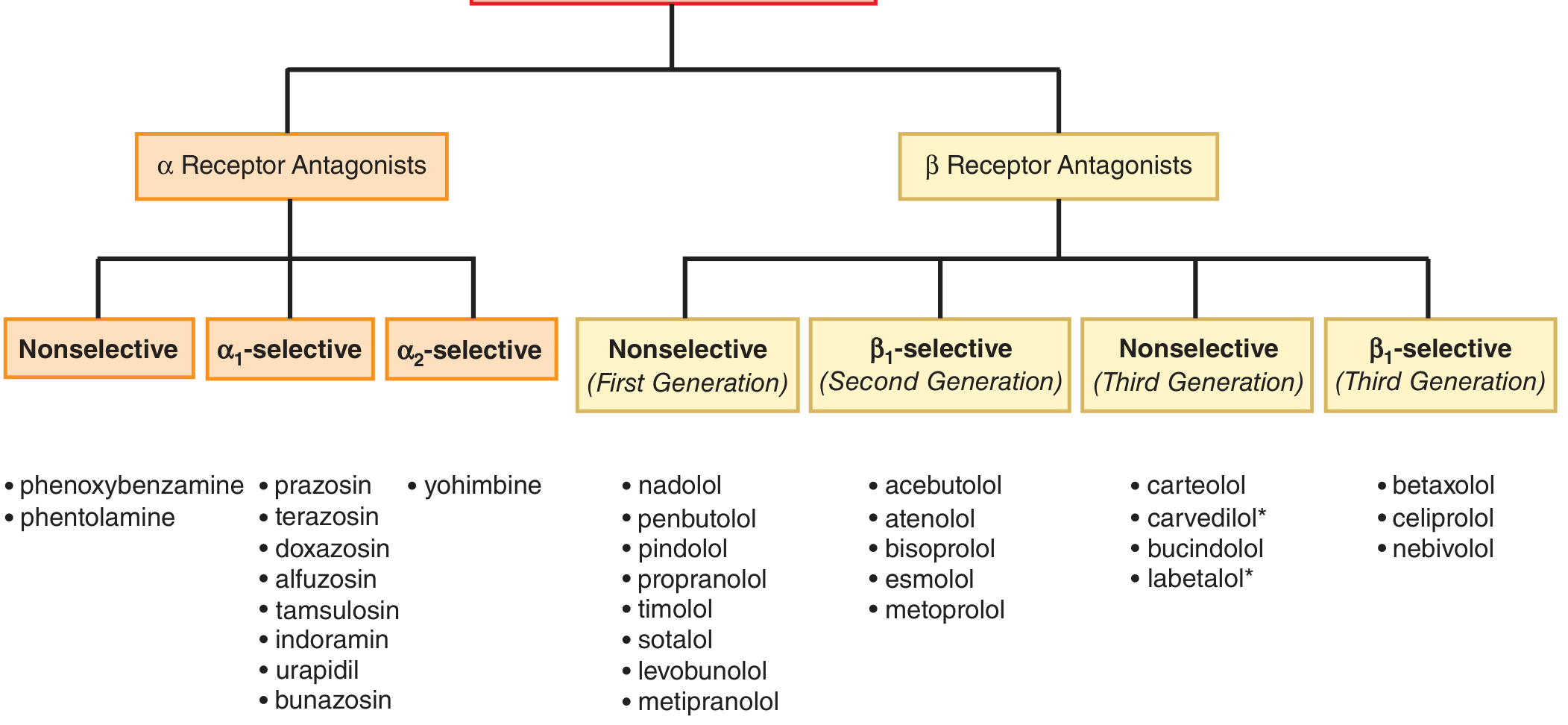
| Generation | Type | Agents |
|---|---|---|
| 1st | Nonselective (β1 + β2) | Propranolol, nadolol, timolol, sotalol, pindolol, penbutolol |
| 2nd | β1-selective (cardioselective) | Metoprolol, atenolol, bisoprolol, esmolol, acebutolol |
| 3rd | Nonselective + vasodilation | Carvedilol (α1 block), carteolol, bucindolol, labetalol (α1 block) |
| 3rd | β1-selective + vasodilation | Nebivolol (NO release), betaxolol, celiprolol |
Mechanism of Action
Beta-blockers competitively antagonize catecholamines (norepinephrine, epinephrine) at adrenergic receptors. Most of the deleterious effects of sympathetic activation in disease are mediated via β1 receptors (heart). β2 receptors are found in bronchial and vascular smooth muscle. Key receptor effects:
- β1 blockade: Negative chronotropy (HR), negative inotropy (contractility), slowed AV nodal conduction, decreased renin release
- β2 blockade (with nonselective agents): Bronchoconstriction, vasoconstriction, inhibition of glycogenolysis (masking hypoglycemia symptoms)
- β1 + β2 + α1 blockade (carvedilol, labetalol): Additional vasodilation via α1 block
Some agents (pindolol, acebutolol, penbutolol) have intrinsic sympathomimetic activity (ISA) - they are partial agonists that cause less resting bradycardia but are generally less effective post-MI.
- Goodman & Gilman's Pharmacological Basis of Therapeutics, p. 288
- Katzung's Basic and Clinical Pharmacology, 16th ed.
Pharmacokinetics
Despite similar pharmacodynamic profiles, beta-blockers differ substantially in pharmacokinetics:
| Property | Lipophilic (e.g., propranolol, metoprolol) | Hydrophilic (e.g., atenolol, nadolol) |
|---|---|---|
| Absorption | High, but significant first-pass effect | Lower |
| Bioavailability | ~30% (propranolol) | Higher |
| CNS penetration | Yes (lipophilic) | Minimal |
| Elimination | Hepatic | Renal |
| Half-life | Short (requires more frequent dosing) | Long (once daily) |
Propranolol is nearly 100% absorbed but first-pass hepatic metabolism reduces bioavailability to ~30% with significant inter-patient variability. Esmolol is ultra-short acting (IV use), metabolized by red blood cell esterases, with rapid offset making it useful when beta-blockade needs to be quickly reversible.
- Braunwald's Heart Disease, p. 464
Clinical Indications
Cardiovascular
- Heart failure with reduced EF (HFrEF) (Class I): Three agents proven to reduce mortality - bisoprolol, sustained-release metoprolol succinate, and carvedilol. They cause initial deterioration (negative inotropy) but lead to reverse LV remodeling and improved EF long-term. Must be started at low doses and up-titrated every 2 weeks.
- Post-MI: Reduce total and sudden cardiac death. Mechanism may involve reduction of ischemic injury, antiarrhythmic effects, and autonomic modulation.
- Hypertension: Reduce cardiac output and renin release.
- Angina pectoris: Reduce oxygen demand (HR, contractility, wall stress). Abrupt withdrawal in angina patients can precipitate worsening angina, arrhythmia, or acute MI due to receptor upregulation.
- Arrhythmias: Control ventricular rate in atrial flutter/fibrillation (prolong AV nodal refractoriness); terminate/prevent AVNRT, inappropriate sinus tachycardia; treat arrhythmias in thyrotoxicosis, pheochromocytoma, long QT syndrome, and post-MI VF reduction.
- Hypertrophic obstructive cardiomyopathy (HOCM)
- Aortic dissection: IV labetalol/esmolol to reduce dP/dt
Non-Cardiovascular
-
Glaucoma: Timolol, betaxolol, levobunolol (ophthalmic drops) - reduce aqueous humor production
-
Essential tremor: Propranolol
-
Migraine prophylaxis: Propranolol, metoprolol, timolol
-
Anxiety/performance anxiety: Propranolol (blocks peripheral adrenergic symptoms)
-
Portal hypertension / variceal bleeding prophylaxis: Propranolol, nadolol (reduce portal pressure via reduced cardiac output and splanchnic vasoconstriction)
-
Hyperthyroidism / thyroid storm: Propranolol (also inhibits T4→T3 conversion)
-
Pheochromocytoma: Used after adequate alpha-blockade (never first - unopposed alpha stimulation can cause hypertensive crisis)
-
Braunwald's Heart Disease, p. 154, 464
Adverse Effects and Contraindications
| Effect | Mechanism | Notes |
|---|---|---|
| Bradycardia / heart block | β1 blockade | Contraindicated in sick sinus syndrome, high-degree AV block |
| Hypotension | Reduced CO | Dose-dependent |
| Bronchoconstriction | β2 blockade | Avoid nonselective agents in asthma/COPD; cardioselective agents safer but not risk-free |
| Masking hypoglycemia | β2 blockade inhibits glycogenolysis | Sweating still occurs (cholinergic); use with caution in type 1 DM |
| Fatigue / weakness | CNS (lipophilic agents) | Often resolves over weeks |
| Cold extremities | Peripheral vasoconstriction | |
| Dyslipidemia | Metabolic (nonselective) | Raise TG, lower HDL slightly |
| Impotence | Reduced blood flow | |
| CNS effects | Lipophilic agents (propranolol) | Nightmares, depression, insomnia |
Withdrawal syndrome: Abrupt discontinuation after chronic use causes receptor upregulation (increased beta-receptor density). In angina or post-MI patients, this can precipitate unstable angina, MI, or ventricular arrhythmias. Always taper gradually.
Absolute Contraindications
- Cardiogenic shock
- Decompensated acute heart failure (relative)
- Significant bradycardia or high-degree AV block (without pacemaker)
- Severe reactive airway disease (nonselective agents)
Overdose / Toxicity
The most toxic beta-blocker is propranolol - 2-3x the therapeutic dose can cause serious toxicity because of its sodium channel-blocking properties (similar to TCAs) and high CNS lipophilicity. Features include bradycardia, hypotension, wide QRS (propranolol), and seizures.
Treatment: Standard resuscitation + glucagon (5-10 mg IV) as the primary antidote. Glucagon raises intracellular cAMP via non-beta-receptor pathways, bypassing the blockade. High-dose insulin therapy and IV lipid emulsion are also used in refractory cases.
- Katzung's Basic and Clinical Pharmacology, p. 1624
Key Drug Comparisons
| Drug | Selectivity | ISA | Additional Features |
|---|---|---|---|
| Propranolol | Nonselective | No | Prototype; lipophilic; Na-channel block at high dose |
| Atenolol | β1 | No | Hydrophilic; once daily; renally cleared |
| Metoprolol | β1 | No | Succinate (XL) for HF; hepatic metabolism (CYP2D6) |
| Bisoprolol | β1 | No | Proven in HF; once daily |
| Carvedilol | β1+β2+α1 | No | Proven in HF; antioxidant properties |
| Labetalol | β1+β2+α1 | Yes | IV use in hypertensive emergencies, aortic dissection |
| Esmolol | β1 | No | Ultra-short acting (t½ ~9 min); titratable IV |
| Nebivolol | β1 | No | NO-mediated vasodilation; 3rd generation |
| Pindolol | Nonselective | Yes | Partial agonist; less bradycardia |
| Sotalol | Nonselective | No | Also Class III antiarrhythmic (K-channel block); prolongs QT |
| Timolol | Nonselective | No | Ophthalmic use (glaucoma); oral for post-MI |
| Acebutolol | β1 | Yes | ISA; less bradycardia; used in HF-intolerant patients |
Clinical Pearls
- HF paradox: Beta-blockers worsen acute decompensated HF but dramatically improve outcomes in stable chronic HFrEF. Only bisoprolol, carvedilol, and metoprolol succinate have proven mortality benefit.
- Selectivity is dose-dependent: At high doses, β1-selective agents lose selectivity and also block β2 receptors.
- Pheochromocytoma rule: Never give a beta-blocker without prior alpha-blockade - this leaves alpha receptors unopposed, causing severe hypertension.
- Sotalol is different: It has beta-blocking AND Class III antiarrhythmic (potassium channel blocking) properties. It prolongs the QT interval and can cause torsades de pointes.
- ISA agents (pindolol, acebutolol): Cause less resting bradycardia and cold extremities. Less effective post-MI than agents without ISA.
- Labetalol IV: Drug of choice for hypertensive emergencies in pregnancy (eclampsia) and aortic dissection because it blocks both α and β receptors.
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics; Katzung's Basic and Clinical Pharmacology, 16th ed.; Braunwald's Heart Disease, 12th ed.; Harrison's Principles of Internal Medicine, 22nd ed.
This is a shared conversation. Sign in to Orris to start your own chat.