Thyroid inhibitors
Reading File
Finding Sources
Finding Sources
Searching PubMed
antithyroid drugs hyperthyroidism
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a thorough overview of thyroid inhibitors drawn from Goodman & Gilman's Pharmacological Basis of Therapeutics and Katzung's Basic and Clinical Pharmacology.
Thyroid Inhibitors
Thyroid inhibitors (also called antithyroid agents or goitrogens) are compounds that reduce thyroid hormone synthesis, release, or peripheral action. They fall into four main categories:
- Thioamides (antithyroid drugs)
- Ionic inhibitors
- High-dose iodine
- Radioactive iodine (¹³¹I)
1. Thioamides
These are the drugs of first choice for medical management of hyperthyroidism.
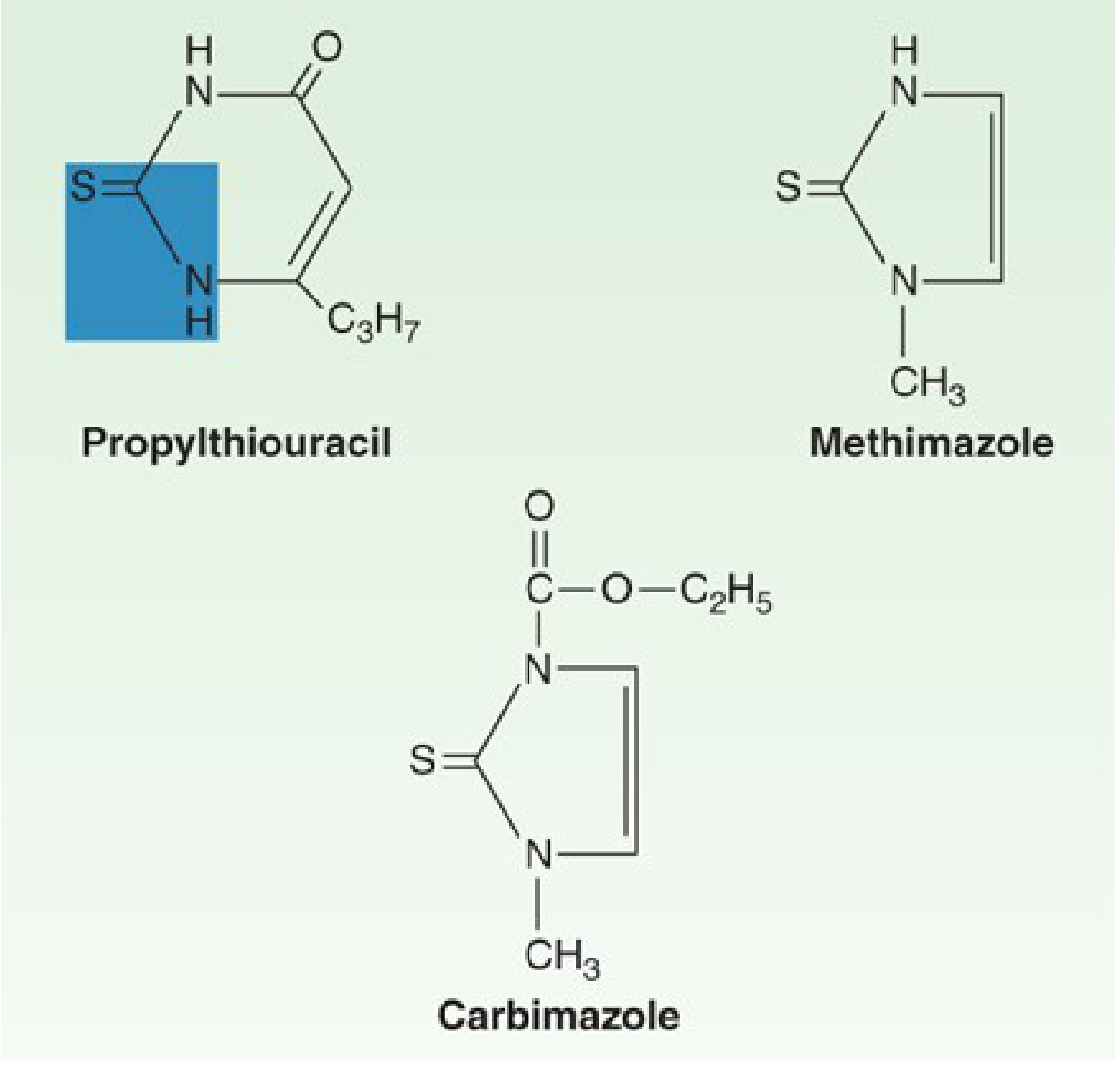
Drugs
- Methimazole (MMI) - first-line in most adults and children; ~10x more potent than PTU
- Propylthiouracil (PTU) - reserved for specific indications (see below)
- Carbimazole - prodrug of methimazole, used in the UK; converted to methimazole after absorption
The thiocarbamide group (C=S) is essential for antithyroid activity.
Mechanism of Action
Thioamides inhibit thyroid peroxidase (TPO), blocking two key steps:
- Organification - incorporation of iodine into tyrosyl residues of thyroglobulin (forming MIT and DIT)
- Coupling - joining of iodotyrosyl residues to form T3 and T4
PTU additionally inhibits peripheral deiodination of T4 to T3 (via Deiodinase type 1, Dio1), making it preferred in thyroid storm.
These drugs deplete stored hormone as thyroglobulin is hydrolyzed and hormones already formed continue to be released - so onset of clinical effect takes several weeks.
- Goodman & Gilman, p. 970
Pharmacokinetics
| Feature | PTU | Methimazole |
|---|---|---|
| Plasma protein binding | ~75% | Nil |
| Plasma t½ | ~75 min | ~4-6 h |
| Dosing frequency | Every 6-8 h | Once daily (for mild-severe disease) |
| Thyroid concentration | Yes | Yes |
| Placental transfer | Yes | Yes |
| Breast milk | Small | More than PTU |
A single 30 mg dose of methimazole exerts antithyroid effects for >24 hours because it concentrates in the thyroid gland.
Clinical Indications
- Graves' disease (primary treatment or pre-surgical)
- Toxic nodular goiter
- Pre-operative preparation before thyroidectomy
- Adjunct before/after radioactive iodine
- Thyroid storm (PTU preferred)
PTU Preferred Situations
- First trimester of pregnancy (methimazole associated with "methimazole embryopathy": aplasia cutis, choanal atresia)
- Thyroid storm (additional T4-to-T3 conversion block)
- Adverse reaction to methimazole (excluding agranulocytosis/hepatitis)
Due to a black box warning about severe hepatitis, PTU should be reserved for use only during the first trimester of pregnancy, in thyroid storm, and when patients are intolerant of methimazole.
- Katzung, p. 1085
Adverse Effects
Common (both drugs):
- Rash, urticaria, pruritus (~5%)
- Arthralgia, myalgia
- Fever, GI disturbance
Serious:
- Agranulocytosis (0.1-0.5%) - most feared; usually in the first 3 months; patients must be warned to report sore throat or fever immediately
- Hepatotoxicity - PTU causes hepatocellular damage (black box warning, can be fatal); methimazole causes cholestatic pattern
- ANCA-associated vasculitis - mainly PTU
- Aplastic anemia - rare
- Both drugs cross the placenta and can cause fetal hypothyroidism and goiter
A 2025 meta-analysis (PMID 40745151) confirmed the dose-dependent risk of agranulocytosis with antithyroid drugs.
2. Ionic Inhibitors
These anions competitively block the sodium/iodide symporter (NIS), preventing iodide uptake into the thyroid.
| Agent | Notes |
|---|---|
| Perchlorate (ClO4-) | 10x more active than thiocyanate; 750 mg/day has been used for Graves disease; fatal aplastic anemia at >2-3 g/day limits use; also used diagnostically to "discharge" inorganic iodide |
| Thiocyanate (SCN-) | Not concentrated by the thyroid; in large doses also inhibits organification; occurs naturally in cruciferous vegetables |
| Fluoroborate (BF4-) | Similar potency to perchlorate |
| Nitrate | Weak inhibitor of NIS |
| Lithium (Li+) | Decreases release of T4 and T3 by mimicking iodide's inhibitory effect on secretion; overt hypothyroidism occurs in some patients on lithium for bipolar disorder |
Perchlorate (ClO4-) blocks the entrance of iodide into the thyroid by competitively inhibiting the NIS and can itself be transported by NIS into the thyroid gland. NIS inhibitors (perchlorate, thiocyanate, nitrate) are additive in inhibiting iodine uptake.
- Goodman & Gilman, p. 972
A 2024 systematic review (PMID 38195966) reviewed perchlorates in hyperthyroidism management, particularly for amiodarone-induced thyrotoxicosis.
3. High-Dose Iodine (Wolff-Chaikoff Effect)
Paradoxically, high concentrations of iodide inhibit thyroid hormone synthesis and release via multiple mechanisms:
- Limits its own transport (NIS downregulation)
- Transiently inhibits organification - the Wolff-Chaikoff effect: high intrathyroidal iodide inhibits TPO
- Inhibits hormone release - the most clinically important acute effect; reduces vascularity of the gland
- Escape occurs after 1-2 weeks as the thyroid adapts (via reduced NIS expression), so iodide alone is not adequate for sustained treatment
Preparations
- Lugol's solution - 8% iodine + 19% potassium iodide; ~8 mg iodide per drop
- Saturated solution of potassium iodide (SSKI/KISS) - 50 mg iodide per drop
Clinical Uses
- Thyroid storm: given after the first dose of PTU/methimazole (never before, to avoid providing substrate for hormone synthesis)
- Pre-operative preparation (Plummer's iodine): reduces vascularity and firmness of the gland before thyroidectomy; given for 7-14 days pre-op
- Radiation emergency: potassium iodide blocks radioactive iodine uptake (protective)
- Neonatal Graves disease: Lugol's solution 1 drop every 8 hours
4. Radioactive Iodine (¹³¹I)
Mechanism
- ¹³¹I behaves chemically identical to stable ¹²⁷I - it is trapped and organified by the thyroid
- Emits beta (β) particles (main therapeutic effect - destroys follicular cells) and gamma rays
- t½ = 8 days; >99% of radiation is expended within 56 days
- Destruction is highly selective - adjacent tissues receive minimal damage
Indications
- Hyperthyroidism in older patients or those with cardiac disease (clearest indication)
- Graves disease that persists or recurs after subtotal thyroidectomy
- Prolonged antithyroid drug treatment without remission
- Toxic nodular goiter
- Thyroid ablation after thyroid cancer surgery
- Treatment of metastatic differentiated thyroid cancer
Dosing
- Usual dose: 4-15 mCi total; targeting delivery of 8 mCi to the thyroid based on 24-h radioiodine uptake
- 80% of patients cured with a single dose; ~20% need a second dose
Contraindications
- Pregnancy (absolute) - causes fetal hypothyroidism
- Breastfeeding
- Children (relative - most centers avoid)
Consequence
- Hypothyroidism in a large proportion of patients over time (the main long-term adverse effect); patients require lifelong levothyroxine replacement
5. Adjunct / Peripheral Inhibitors
These agents do not reduce thyroid hormone synthesis but blunt peripheral effects or T4-to-T3 conversion:
| Agent | Mechanism | Use |
|---|---|---|
| Beta-blockers (propranolol, atenolol) | Block adrenergic manifestations (tachycardia, tremor, sweating) | Immediate symptom relief in hyperthyroidism and thyroid storm |
| Calcium channel blockers | Control heart rate | When beta-blockers contraindicated (e.g., asthma) |
| Amiodarone | Inhibits T4-to-T3 conversion (Dio1) + iodine load (can cause hypo- or hyperthyroidism) | Antiarrhythmic; affects thyroid as a side effect |
| Oral cholecystographic agents (iopanoic acid, ipodate) | Potent Dio1 inhibitors; also reduce T4 release | Rarely used; rapid T3 lowering in thyroid storm |
| Glucocorticoids | Inhibit Dio1; reduce T4-to-T3 conversion; treat type II amiodarone-induced thyrotoxicosis | Used in thyroid storm and amiodarone-induced thyrotoxicosis (type II) |
6. Drugs That Disrupt Thyroid Hormone Synthesis/Metabolism (Summary Table)
| Mechanism | Agents |
|---|---|
| Iodide uptake (NIS block) | Perchlorate, fluoroborate, thiocyanate, nitrate |
| Organification of iodine | Thioamides (PTU, methimazole, carbimazole), thiocyanate, sulfonamides |
| Coupling reaction | Sulfonamides, thioamides |
| Hormone release | Li+ salts, iodide |
| Peripheral deiodination (T4→T3) | PTU, amiodarone, oral cholecystographic agents |
| Accelerated hepatic metabolism | Phenobarbital, rifampin, carbamazepine, phenytoin, sertraline, bexarotene |
| TSH/TRH suppression | Dopamine, glucocorticoids, somatostatin, bexarotene, metformin |
- Goodman & Gilman, Table 47-4, p. 970
Thyroid Storm - Treatment Protocol
Thyroid storm is treated with all four drug classes in sequence:
- PTU (large doses) - blocks synthesis AND peripheral conversion
- Iodide (Lugol's or SSKI) - given 1 hour AFTER PTU - blocks release
- Beta-blocker (propranolol) - controls adrenergic symptoms
- Glucocorticoids - inhibit Dio1, treat adrenal insufficiency
- Treat precipitating cause
- Supportive care (IV fluids, cooling, antipyretics)
Sources:
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, pp. 970-973
- Katzung's Basic and Clinical Pharmacology, 16th Ed., pp. 1085-1092
- Recent evidence: PMID 40891035 (mortality comparison: drugs vs RAI vs surgery, 2025 network meta-analysis), PMID 40745151 (agranulocytosis dose-risk, 2025 meta-analysis), PMID 38195966 (perchlorates in hyperthyroidism, 2024 systematic review)
This is a shared conversation. Sign in to Orris to start your own chat.