Hyperthyroidism with Fibromyoma Uterus for Total Abdominal Hysterectomy on a 55 year old woman. Make an exam ready long case presentation for an anesthesia md exam using relevant information from standard books with mentioning hyperthyroidism and also management of lithotomy position in the intra-op period
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
This is a fully exam-ready long case presentation drawn directly from the standard anesthesia textbooks (Miller's 10e, Barash 9e, Morgan & Mikhail 7e). Here is a structured summary of what is covered and why it matters for your MD exam:
What This Long Case Covers
12 comprehensive sections:
- Case Presentation - Demographics, diagnosis, co-morbidity, ASA grade
- History - Fibromyoma + hyperthyroid symptoms, drug history, obstetric history
- Clinical Examination - Including thyroid, CVS, airway assessment, proptosis note
- Investigations - Routine + thyroid-specific + gynaecological; expected findings explained
- Preoperative Optimization - The single most critical point: render euthyroid; 6-8 week prep with PTU/methimazole + Lugol's iodine (after antithyroid drugs) + beta-blockers + glucocorticoids
- Pre-anaesthetic Visit - NPO, premedication, risk consent
- Anaesthetic Management - Monitoring, induction (propofol preferred, ketamine avoided), NMB cautions (myasthenia gravis risk), airway management for goiter, maintenance goals
- Lithotomy Position Management - Physiological changes (FRC decrease, cardiovascular shifts), technique (2-person rule, padding), full nerve injury table, compartment syndrome risk, mandatory BP check on leg lowering
- Thyroid Storm Management - Full drug protocol table; distinction from malignant hyperthermia (critical viva question)
- Regional Anaesthesia - Options and precautions (no epinephrine)
- Postoperative Management - ICU criteria, monitoring, analgesia, complications
- Viva Summary Table + Anticipated Examiner Questions
I want you to make it a case presentation with CSE as the choice of anaesthesia and with fake values and patient details
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
I have all the source material needed. Let me now write the complete case presentation.
LONG CASE PRESENTATION
MD Anaesthesiology Examination
CASE: HYPERTHYROIDISM WITH FIBROMYOMA UTERUS FOR TOTAL ABDOMINAL HYSTERECTOMY
Anaesthesia Technique: Combined Spinal-Epidural (CSE)
SECTION 1: PATIENT BIODATA
| Name | Mrs. Rekha Nambiar |
| Age | 55 years |
| Sex | Female |
| Weight | 58 kg |
| Height | 158 cm |
| BMI | 23.2 kg/m² |
| IP No. | 2024/GYN/04817 |
| Ward | Gynaecology Ward, Bed 12 |
| Date of Admission | 28th May 2026 |
| Date of Surgery | 4th June 2026 |
| Consultant Surgeon | Dr. Meera Pillai, MS (OBG) |
| Consultant Anaesthesiologist | Dr. Arjun Krishnamurthy, MD (Anaes) |
| Diagnosis | Fibromyoma Uterus with Hyperthyroidism (Graves' Disease) |
| Proposed Surgery | Total Abdominal Hysterectomy with Bilateral Salpingo-Oophorectomy (TAH + BSO) |
| ASA Status | ASA Grade II |
SECTION 2: CHIEF COMPLAINTS
- Heavy, prolonged, irregular menstrual bleeding for 3 years
- Lower abdominal heaviness and pelvic pressure for 2 years
- Increased urinary frequency for 6 months
- Palpitations, heat intolerance, and tremors for 2 years
- Loss of weight (approximately 7 kg over 18 months)
SECTION 3: HISTORY OF PRESENT ILLNESS
Mrs. Rekha Nambiar is a 55-year-old homemaker who presented to the gynaecology outpatient department with a 3-year history of progressively worsening menorrhagia and metrorrhagia, associated with passage of clots. She reports increasing lower abdominal heaviness and a feeling of pelvic fullness. Urinary frequency without dysuria or incontinence was noted over the last 6 months, likely attributable to uterine compression of the bladder.
Ultrasonography of the pelvis (dated 12 April 2026) confirmed: multiple intramural and subserosal fibroids, largest measuring 8.4 × 7.1 cm in the fundal region. Total uterine size equivalent to 18 weeks of gestation. No adnexal pathology detected.
Concurrently, she was diagnosed with Graves' disease 2 years ago on the basis of symptoms of thyrotoxicosis (palpitations, heat intolerance, weight loss, anxiety, tremors, increased stool frequency), elevated free T4, suppressed TSH, and positive anti-TSH receptor antibodies. She is currently on antithyroid medication and has been reviewed jointly by endocrinology.
SECTION 4: PAST HISTORY
- Medical: Hyperthyroidism (Graves' disease) - 2 years; on treatment
- Surgical: Lower segment caesarean section (LSCS) x2 (1994, 1997) - relevant for potential intraabdominal adhesions
- Anaesthetic: Two prior spinal anaesthetics for LSCS - uneventful; no post-dural puncture headache (PDPH)
- Psychiatric: Nil
- Allergies: No known drug allergies (NKDA)
SECTION 5: DRUG HISTORY
| Drug | Dose | Frequency | Duration |
|---|---|---|---|
| Tab. Carbimazole | 15 mg | OD | 18 months |
| Tab. Propranolol | 40 mg | BD | 18 months |
| Tab. Ferrous sulfate + Folic acid | 325 mg | BD | 6 weeks |
| Tab. Vitamin D3 | 60,000 IU | Weekly | 3 months |
Note: All antithyroid medications and beta-blockers continued without interruption through the morning of surgery.
SECTION 6: FAMILY AND PERSONAL HISTORY
- Family history: No known thyroid disease; no family history of bleeding disorders
- Menstrual history: Menarche at 13; cycles previously regular 28/4-5 days; now irregular 21-35 days cycle, 7-10 days duration, heavy with clots (soaking 6-8 pads/day)
- Obstetric history: G3P3+0 (LSCS x2, normal vaginal delivery x1); LMP: 18th May 2026 (heavy)
- Occupation: Homemaker; sedentary activity
- Appetite: Increased despite weight loss
- Bowel/Bladder: Frequency of stools (3-4/day); urinary frequency (9-10 times/day)
- Sleep: Disturbed; difficulty falling asleep
- Habits: Non-smoker, no alcohol, no tobacco
SECTION 7: GENERAL PHYSICAL EXAMINATION
| Parameter | Finding |
|---|---|
| Consciousness | Alert, oriented to time, place, person |
| Build and nutrition | Moderate; lean for age |
| Pallor | Present (+) |
| Icterus | Absent |
| Cyanosis | Absent |
| Clubbing | Absent |
| Lymphadenopathy | Absent |
| Oedema | Absent |
| Proptosis | Mild bilateral proptosis (Graves' ophthalmopathy) |
| Skin | Warm, moist, fine velvety texture |
| Tremors | Fine tremors of outstretched hands bilaterally |
SECTION 8: VITAL SIGNS
| Parameter | Value |
|---|---|
| Pulse rate | 88/min, regular, good volume, bilateral radial equal |
| Blood pressure | 134/72 mmHg (Right arm, sitting) - widened pulse pressure |
| Respiratory rate | 18/min |
| Temperature | 37.1°C (oral) |
| SpO2 | 99% on room air |
| Weight | 58 kg |
| Height | 158 cm |
SECTION 9: SYSTEMIC EXAMINATION
9.1 Cardiovascular System
- Hyperdynamic precordium
- Apex beat: 5th intercostal space, midclavicular line
- Heart sounds: S1, S2 heard, no murmurs; possible soft S3 (high-output state)
- No signs of cardiac failure; no raised JVP; no peripheral oedema
9.2 Respiratory System
- Equal bilateral air entry
- No added sounds; no wheeze
- Trachea: Central - no deviation from goiter compression
9.3 Thyroid Gland
- Diffusely enlarged, Grade II goiter
- Soft, non-tender, moves on swallowing
- Thyroid bruit present on auscultation
- Pemberton's sign: Negative
- No tracheal deviation
9.4 Per Abdomen
- Uterus palpable: hard, irregular; fundal height equivalent to 18 weeks gestation
- No ascites; no other palpable organomegaly
- Bowel sounds: Normal
9.5 Per Speculum / Per Vaginum (documented by gynaecologist)
- Cervix: Healthy; Os closed
- Uterus: Bulky, irregular, mobile; multiple fibroid masses
- Adnexa: No tenderness; no adnexal mass
SECTION 10: AIRWAY ASSESSMENT
| Parameter | Finding |
|---|---|
| Mouth opening | 4.5 cm (adequate: >3.5 cm) |
| Mallampati Class | Class II |
| Thyromental distance | 7.5 cm (adequate: >6.5 cm) |
| Sternomental distance | 14 cm (adequate: >12.5 cm) |
| Neck movements | Full range in all directions |
| Neck circumference | 37 cm |
| Dentition | Intact; no loose teeth; no caps or crowns |
| Jaw protrusion (ULBT) | Class I |
| BMI | 23.2 (non-obese) |
| Trachea | Midline; no extrinsic compression |
| Caution | Mild goiter present - re-examine if goiter enlarges; proptosis noted for eye care |
Airway Summary: Predicted EASY airway. However, given the presence of a thyroid goiter, difficult airway equipment must be available as a standard precaution.
SECTION 11: INVESTIGATIONS
11.1 Haematological
| Investigation | Result | Normal Range |
|---|---|---|
| Haemoglobin | 9.4 g/dL | 12-16 g/dL |
| Total WBC count | 8,400/mm³ | 4,000-11,000/mm³ |
| Platelet count | 2,18,000/mm³ | 1.5-4 lakh/mm³ |
| PCV (Haematocrit) | 31% | 36-46% |
| MCV | 72 fL | 80-100 fL |
| MCH | 23 pg | 27-32 pg |
| Peripheral smear | Microcytic hypochromic anaemia consistent with iron deficiency | |
| PT/INR | 13.2 sec / 1.0 | 11-14 sec / <1.2 |
| aPTT | 29 seconds | 25-35 seconds |
| Bleeding time | 2 min 30 sec | 1-3 minutes |
| Clotting time | 5 min 10 sec | 4-8 minutes |
Note: Thrombocytopenia not present - neuraxial anaesthesia NOT contraindicated. Platelet count >1,00,000 - CSE safe to proceed.
11.2 Biochemistry
| Investigation | Result | Normal Range |
|---|---|---|
| Blood urea | 24 mg/dL | 15-40 mg/dL |
| Serum creatinine | 0.8 mg/dL | 0.5-1.1 mg/dL |
| Serum sodium | 138 mEq/L | 136-145 mEq/L |
| Serum potassium | 3.6 mEq/L | 3.5-5.0 mEq/L |
| Serum calcium | 9.2 mg/dL | 8.5-10.5 mg/dL |
| Random blood glucose | 104 mg/dL | <140 mg/dL |
| Liver function tests | Within normal limits (ALT 28 U/L, AST 24 U/L) | - |
| Total bilirubin | 0.7 mg/dL | 0.3-1.2 mg/dL |
| Total protein / Albumin | 6.8 / 3.9 g/dL | 6.5-8.5 / 3.5-5.0 |
11.3 Thyroid Function Tests
| Test | Patient Value | Normal Range | Interpretation |
|---|---|---|---|
| TSH (3rd generation) | 0.38 mIU/L | 0.4-4.0 mIU/L | Low-normal; ACCEPTABLE FOR SURGERY |
| Free T4 (FT4) | 16.2 pmol/L | 12-22 pmol/L | Normal |
| Free T3 (FT3) | 4.8 pmol/L | 3.1-6.8 pmol/L | Normal |
| Anti-TSH receptor Ab (TRAB) | 3.2 IU/L (elevated) | <1.75 IU/L | Confirms Graves' disease |
| Anti-TPO Ab | 64 IU/mL (elevated) | <35 IU/mL | Positive |
Endocrinology opinion (dated 27 May 2026): "Patient is biochemically euthyroid on current antithyroid therapy. TFTs acceptable. Cleared for elective surgery. Continue Carbimazole and Propranolol perioperatively."
11.4 Electrocardiogram (ECG)
- Rate: 88/min
- Rhythm: Normal sinus rhythm
- Axis: Normal
- P waves: Normal morphology
- PR interval: 0.16 sec
- QRS: 0.08 sec; no widening
- QTc: 420 ms (normal)
- ST-T changes: None
- Impression: Normal sinus rhythm; no evidence of atrial fibrillation or ischaemia
11.5 Chest X-ray (PA view)
- Trachea: Central, no deviation
- Lung fields: Clear bilaterally; no consolidation; no pleural effusion
- Heart: Normal in size (cardiothoracic ratio 0.48)
- Mediastinum: Normal width
- Bones: No abnormality
11.6 Ultrasonography Pelvis (12 April 2026)
- Multiple intramural and subserosal fibroids
- Largest fibroid: 8.4 × 7.1 cm (fundal)
- Total uterus size: 18 weeks equivalent
- Endometrial thickness: 9 mm (slightly thickened)
- Ovaries: Normal bilaterally
- No free fluid in pelvis
11.7 Echocardiography (30 April 2026)
- LV function: Preserved; EF 64%
- LV dimensions: Mild increase in LV end-diastolic diameter (52 mm) - consistent with high-output state
- No regional wall motion abnormality
- Valves: Normal; no regurgitation
- No pericardial effusion
- Impression: Mild hyperdynamic circulation consistent with partially treated hyperthyroidism; no structural cardiac disease
11.8 Blood Group and Crossmatch
- Blood group: O Positive
- Crossmatch: 2 units packed red blood cells (PRBC) crossmatched and held in blood bank
SECTION 12: PREOPERATIVE ANAESTHETIC ASSESSMENT & OPTIMIZATION
12.1 Problem List
- Hyperthyroidism (Graves' disease) - now biochemically euthyroid
- Mild iron-deficiency anaemia (Hb 9.4 g/dL)
- Mild hyperdynamic cardiac state (EF preserved; LV mildly dilated)
- Large fibromyoma uterus (18-week size) - increased surgical complexity
- Prior LSCS x2 - risk of intraabdominal adhesions
- Mild bilateral proptosis - eye protection required
- Normal airway, but goiter present - difficult airway equipment mandatory
12.2 Preoperative Optimization
Goal: Confirm and maintain euthyroid state before elective surgery.
(Barash's Clinical Anaesthesia 9e: "The most important goal in managing the hyperthyroid patient is to make the patient euthyroid before surgery.")
Achieved in this patient:
- TSH: 0.38 mIU/L (low-normal, acceptable)
- Free T4 and T3: Normal
- Resting heart rate: 88/min (target <90/min)
- 18 months of antithyroid therapy completed
Additional measures taken:
- Iron supplementation for 6 weeks (Hb improved from 7.8 to 9.4 g/dL)
- Cardiology and endocrinology clearance obtained
- Continue all antithyroid drugs and beta-blockers up to and including morning of surgery
12.3 Pre-anaesthetic Consent
Risks explained to patient including:
- Hypotension with neuraxial block (managed with fluids and vasopressors)
- Post-dural puncture headache (PDPH) - low risk with pencil-point needle
- Neurological complications (rare: <0.1%)
- Thyroid storm risk (low given euthyroid state; plan in place)
- Haemorrhage requiring transfusion (2 units crossmatched)
- Conversion to general anaesthesia if regional fails
- Lithotomy position: nerve injury risk, compartment syndrome (if prolonged)
- Epidural catheter complications: infection, intravascular placement, dural puncture
Patient given written information. Informed consent signed.
SECTION 13: PRE-ANAESTHETIC MEDICATION AND PREPARATION
13.1 Night Before Surgery
- Tab. Carbimazole 15 mg (continue as scheduled)
- Tab. Propranolol 40 mg (continue as scheduled)
- Tab. Lorazepam 1 mg orally at 10 PM (anxiolysis)
- Tab. Ranitidine 150 mg orally at 10 PM (aspiration prophylaxis)
- NPO after midnight (solids 6 hours; clear fluids 2 hours before surgery)
13.2 Morning of Surgery (06:00 AM)
- Tab. Carbimazole 15 mg with a sip of water at 6 AM
- Tab. Propranolol 40 mg with a sip of water at 6 AM
- Tab. Ranitidine 150 mg orally at 6 AM
- Tab. Metoclopramide 10 mg orally at 6 AM
- IV access secured: 18G IV cannula in right dorsal hand vein
- Co-loading: Ringer's Lactate 500 mL commenced 30 min before block
SECTION 14: ANAESTHETIC MANAGEMENT
14.1 Choice of Anaesthesia: COMBINED SPINAL-EPIDURAL (CSE)
Rationale for choosing CSE over General Anaesthesia in this patient:
| Advantage | Relevance to This Case |
|---|---|
| Avoids airway instrumentation | Reduces sympathetic activation at laryngoscopy (critical in hyperthyroid patient) |
| Avoids sympathomimetic induction agents | No ketamine needed; no intubation-related catecholamine surge |
| Rapid, dense block from spinal component | Reliable surgical anaesthesia for TAH |
| Flexible duration via epidural catheter | TAH with BSO may be prolonged; adhesions from prior LSCS |
| Superior postoperative analgesia | Epidural reduces opioid requirement; lower postop sympathetic activation |
| Reduced catecholamine response | Blunts surgical stress - protective in hyperthyroid state |
| Regional analgesia reduces thyroid storm risk | Minimises physiological stress of surgery |
(Barash's Clinical Anaesthesia 9e: "Regional anesthesia is an excellent alternative when appropriate.")
(Morgan & Mikhail 7e: "CSE combines the benefit of rapid, reliable, intense blockade of spinal anesthesia with the flexible utility of an epidural catheter.")
Contraindications to CSE ruled out:
- Platelets >1,00,000 (2,18,000) - safe
- INR 1.0 (normal) - safe
- No systemic sepsis / skin infection at site
- No patient refusal
- No raised intracranial pressure
14.2 Monitoring Setup (Before Block)
All monitors attached and baseline values recorded:
| Monitor | Value at Baseline |
|---|---|
| ECG (5-lead) | NSR, HR 88/min |
| NIBP (right arm) | 134/72 mmHg |
| SpO2 | 99% on room air |
| Temperature (oropharyngeal/tympanic) | 37.1°C |
| Urine output via Foley catheter | Inserted pre-block; clear urine flowing |
IV Access:
- Right hand: 18G cannula (for drugs, fluids)
- Left antecubital fossa: 16G cannula (for rapid fluid/blood transfusion if needed)
Emergency drugs drawn up and labelled:
- Inj. Phenylephrine 100 mcg/mL (first-line vasopressor for neuraxial hypotension; preferred direct-acting agent in hyperthyroid patient) (Miller's Anaesthesia 10e)
- Inj. Mephenteramine 6 mg/mL (alternate vasopressor)
- Inj. Atropine 0.6 mg/mL (avoid unless truly needed; watch bradycardia from spinal)
- Inj. Esmolol 10 mg/mL ready (for tachycardia or impending thyroid storm)
- Inj. Ephedrine 6 mg/mL (as backup only - use cautiously given hyperthyroid state)
- Inj. Succinylcholine 100 mg (for failed CSE or emergency GA conversion)
Difficult Airway Trolley: Checked and immediately available (goiter present)
Warming devices: Forced-air warming blanket; warm IV fluids; OR temperature set to 22°C
14.3 Pre-loading
- Inj. Ringer's Lactate 500 mL co-loading commenced 30 minutes before spinal injection
- Rationale: Reduces incidence and severity of spinal-induced hypotension
14.4 CSE Technique
(Barash's Clinical Anaesthesia 9e; Morgan & Mikhail 7e)
Patient Position: Sitting upright (preferred over lateral for TAH - better landmark identification; more predictable hyperbaric bupivacaine spread; allows CSF visualisation)
Site: L3-L4 interspace (identified by Tuffier's line/iliac crest line)
(Barash 9e: "It is safest to perform a CSE block at the L3-L4 or L4-L5 interspaces")
Technique - Needle-Through-Needle:
Step 1 - Epidural space identification:
- Skin cleaning with 10% povidone-iodine; sterile draping
- Subcutaneous infiltration: Inj. Lignocaine 2% - 2 mL at L3-L4
- 16G Tuohy needle inserted at L3-L4 using midline approach
- Loss of resistance (LOR) to saline technique used
- Epidural space identified at 5.5 cm from skin
- (Air avoided in LOR syringe to allow clear differentiation of CSF from air when spinal needle inserted)
Step 2 - Subarachnoid block:
- 25G Whitacre pencil-point spinal needle inserted through Tuohy needle (needle-through-needle technique)
- Subtle "pop" felt as dura pierced; stylet withdrawn
- Free flow of clear CSF confirmed in upright position
- Spinal needle hub and Tuohy hub stabilised by pinching between thumb and index finger (Barash 9e)
- Intrathecal injection:
- Inj. Bupivacaine 0.5% heavy (hyperbaric) - 2.2 mL (11 mg)
- Inj. Fentanyl 25 mcg (0.5 mL) - intrathecal adjuvant (enhances quality and duration of block, reduces bupivacaine requirement)
- Inj. Morphine 0.1 mg (intrathecal, for postoperative analgesia)
- Total intrathecal volume: 2.7 mL
- Injection over 20 seconds; barbotage avoided
Step 3 - Epidural catheter placement:
- After spinal injection, spinal needle withdrawn
- 18G epidural catheter threaded through Tuohy needle - 4 cm in the epidural space (total 9.5 cm from skin)
- Tuohy needle withdrawn; catheter aspirated (no blood, no CSF)
- Test dose: Inj. Lignocaine 2% with adrenaline 1:200,000 - 3 mL via epidural catheter
- Monitor for 5 minutes: no tachycardia (caution in hyperthyroid patient - baseline HR 88/min), no sensory change in upper limbs (intrathecal)
- Test dose NEGATIVE - catheter in epidural space
- Note for hyperthyroid patients: The tachycardia criterion for positive intravascular test dose may be unreliable due to baseline tachycardia and beta-blockade; rely on blood pressure and CNS symptoms
- Catheter secured and labelled "EPIDURAL"
Patient positioned supine with left lateral tilt of 15° (for aortocaval decompression; large uterus may compress IVC in supine)
14.5 Assessment of Block
Dermatomal level assessed with cold sensation (ethyl chloride spray):
| Time | Upper Sensory Level | Comment |
|---|---|---|
| 5 min post-spinal | T8 | Bilateral |
| 10 min post-spinal | T6 | Bilateral |
| 15 min post-spinal | T4 | Target achieved |
| Surgery started (20 min post-spinal) | T4 | Maintained |
- Motor block (Bromage scale): Grade 3 bilaterally at 15 minutes (unable to move legs)
- Haemodynamics at 15 minutes: BP 118/68 mmHg, HR 80/min
- Mild hypotension managed (see below)
- Patient comfort: Comfortable; no pain; pressure sensation at lower abdomen (acceptable and expected)
Target sensory level for TAH: T4 bilaterally (to cover peritoneal, uterine, and upper abdominal manipulation)
14.6 Management of Haemodynamics During Block
| Time | BP | HR | Action Taken |
|---|---|---|---|
| Baseline | 134/72 | 88 | - |
| 5 min post-spinal | 124/68 | 84 | Continue RL co-load |
| 10 min post-spinal | 108/62 | 80 | Inj. Phenylephrine 100 mcg IV bolus |
| 12 min post-spinal | 116/66 | 78 | Stable; no further vasopressor |
| 15 min post-spinal | 118/68 | 80 | Surgery commenced |
| Intraoperative (45 min) | 122/70 | 82 | Stable |
| Intraoperative (90 min) | 120/72 | 84 | Stable |
| Post-delivery of uterus | 116/66 | 80 | Epidural top-up planned |
Why Phenylephrine preferred over Ephedrine:
In hyperthyroid patients with enhanced catecholamine sensitivity, direct-acting vasopressors (phenylephrine - alpha-1 agonist, no beta stimulation) are preferred. Indirect agents like ephedrine release catecholamines and may exacerbate tachycardia and hypertension. (Miller's Anaesthesia 10e)
14.7 Epidural Catheter Management Intraoperatively
Epidural top-up given at 90 minutes (sensory block receding to T6):
- Inj. Bupivacaine 0.5% isobaric - 8 mL via epidural catheter (fractionated: 3 mL + 5 mL with 2-minute interval)
- Sensory level restored to T4 within 15 minutes
- No adverse event from top-up
Epidural infusion commenced at closure:
- Inj. Bupivacaine 0.1% + Fentanyl 2 mcg/mL infusion at 8 mL/hour via epidural catheter (postoperative analgesia)
14.8 Sedation / Anxiolysis During Surgery
- Patient awake but comfortable; mild anxiety noted at start
- Inj. Midazolam 1 mg IV given slowly (avoid excessive sedation; titrate cautiously in hyperthyroid state due to heightened CNS sensitivity)
- Supplemental oxygen: 3L/min via nasal prongs (SpO2 maintained 99-100%)
SECTION 15: MANAGEMENT OF LITHOTOMY POSITION (INTRAOPERATIVE)
(Morgan & Mikhail's Clinical Anaesthesiology 7e, p.1298-1300)
TAH in this patient was performed in modified lithotomy position for the initial surgical exposure.
15.1 Physiological Changes and Management
A. Respiratory:
- FRC decreases in lithotomy position - predisposes to atelectasis and hypoxia (Morgan & Mikhail 7e)
- Supplemental O2 via nasal prongs maintained at 4L/min
- SpO2 monitored continuously; maintained at 99-100%
B. Cardiovascular - Leg Elevation Phase:
- Elevation of legs acutely autotransfuses ~300-500 mL blood into central circulation - cardiac output and MAP may transiently increase (Morgan & Mikhail 7e)
- In this hyperthyroid patient (already hyperdynamic, EF 64%), this caused brief increase in BP to 128/78 mmHg at leg elevation; HR 86/min
- Esmolol 10 mg IV given as a slow bolus to manage the rise; HR settled to 80/min
C. Cardiovascular - Leg Lowering Phase (CRITICAL):
- Lowering legs from lithotomy acutely reduces venous return, causing SUDDEN HYPOTENSION (Morgan & Mikhail 7e)
- Blood pressure MEASURED IMMEDIATELY after legs lowered - mandatory (Morgan & Mikhail 7e)
- Both legs lowered simultaneously and slowly by two theatre staff members
- BP at 1 minute post-lowering: 112/64 mmHg - mild hypotension - treated with Inj. Phenylephrine 50 mcg IV; BP normalised to 122/70 mmHg within 90 seconds
15.2 Positioning Technique Used
| Step | Action Taken |
|---|---|
| Personnel | Two theatre assistants raised and lowered both legs simultaneously |
| Stirrups | Allen stirrups used; padded at all leg contact points |
| Straps | Not compressing popliteal fossa; pulse checked distal to straps |
| Arms | Tucked to sides; hands and fingers COMPLETELY enclosed in cotton wool padding (protection from OR table section injury) (Morgan & Mikhail 7e) |
| Ankle position | Neutral; no forced dorsiflexion or plantar flexion |
| Hip flexion | Moderate (not excessive); thigh-trunk angle <90° |
| External rotation | Minimal; avoid extreme external rotation of hip |
| Duration in lithotomy | 55 minutes (acceptable; <2 hours for compartment syndrome risk) |
15.3 Nerve Injury Prevention
| Nerve | Risk | Prevention Applied |
|---|---|---|
| Common peroneal | Lateral knee on stirrup | Allen stirrup with padded lateral support; knee checked |
| Saphenous | Medial compression | No medial strap used; lateral holder only |
| Obturator | Excessive thigh flexion | Hip angle kept moderate |
| Sciatic | Extreme hip flexion | Hip flexion kept <80° |
| Lumbosacral plexus | Stretch/compression | Most vulnerable - monitored; position regularly re-examined |
| Brachial plexus | Axilla hyperextension | Arms tucked; no abduction; no hyperextension |
Pre-existing neuropathy documented: Nil (documented in pre-anaesthetic notes as per protocol) (Morgan & Mikhail 7e)
15.4 Compartment Syndrome Precautions
- Total lithotomy time: 55 minutes - low risk
- No tight straps or circumferential compression applied
- Calves checked for tense compartments at end of surgery - soft bilaterally
- Plan: CK level at 6 hours postoperatively (protocol for lithotomy >30 minutes)
SECTION 16: INTRAOPERATIVE VIGILANCE FOR THYROID STORM
16.1 Triggering factors in this case
- Surgical stress (intraabdominal surgery, peritoneal handling)
- Prior anxiety (mitigated by anxiolysis)
- Blood loss
16.2 Intraoperative Course (Thyroid Storm - Not Occurred)
- Temperature monitored every 30 minutes throughout surgery
- Highest temperature recorded: 37.4°C (no fever; no storm)
- HR range: 78-88/min throughout
- No tachyarrhythmia; no ST changes on ECG
16.3 Thyroid Storm Protocol - STANDING ORDERS IN OR
(Barash 9e Table 47-3; Morgan & Mikhail 7e)
If features of thyroid storm arise (hyperthermia >38.5°C, unexplained tachycardia >120/min, altered sensorium, haemodynamic instability):
| Priority | Drug / Intervention | Dose |
|---|---|---|
| 1 | Aggressive IV fluid resuscitation | Ringer's Lactate 500 mL stat |
| 2 | Inj. Esmolol infusion | 50-350 mcg/kg/hr; target HR <100/min |
| 3 | PTU via nasogastric tube | 200-400 mg q6h |
| 4 | Sodium iodide (after PTU) | 250 mg IV q6h (Wolff-Chaikoff effect) |
| 5 | Inj. Hydrocortisone | 100 mg IV q8h (blocks T4-T3 conversion; treats adrenal insufficiency) |
| 6 | Active cooling | Cold saline, cooling blanket |
| 7 | Inj. Paracetamol | 1 g IV q6h (avoid salicylates - worsen thyrotoxicosis) |
| 8 | Inj. Pethidine | 25 mg IV q4h (prevent shivering) |
| 9 | ICU transfer | Invasive monitoring; arterial line; CVP |
Distinguish from Malignant Hyperthermia (MH):
Thyroid storm does NOT cause muscle rigidity, does NOT elevate creatine kinase, does NOT produce marked lactic acidosis. MH responds to dantrolene; thyroid storm does not. (Morgan & Mikhail 7e; Miller's 10e)
SECTION 17: INTRAOPERATIVE SUMMARY
| Parameter | Value |
|---|---|
| Total surgical time | 2 hours 10 minutes |
| Total anaesthesia time | 2 hours 40 minutes |
| Time in lithotomy | 55 minutes |
| Estimated blood loss | 620 mL |
| IV fluids administered | Ringer's Lactate 2000 mL; Normal Saline 500 mL |
| Urine output | 340 mL (1.3 mL/kg/hr) |
| Blood transfusion | 1 unit PRBC transfused (Hb dropped to 8.1 g/dL intraop) |
| Temperature range | 37.1°C - 37.4°C |
| HR range | 78 - 88/min |
| BP range | 108/60 - 128/78 mmHg |
| Vasopressor used | Phenylephrine 150 mcg total |
| SpO2 | 99-100% throughout |
| Antiemetics given | Inj. Ondansetron 4 mg IV (nausea during peritoneal closure) |
| Additional sedation | Inj. Midazolam 1 mg IV (early); Inj. Dexmedetomidine 0.4 mcg/kg/hr infusion (for sedation during prolonged closure - well tolerated) |
| Epidural top-up | 1 top-up at 90 minutes (Bupivacaine 0.5% 8 mL) |
SECTION 18: POSTOPERATIVE MANAGEMENT
18.1 Immediate Recovery (PACU)
Monitored in recovery room for 2 hours:
- ECG: Continuous
- NIBP: Every 5 minutes for 30 minutes, then every 15 minutes
- SpO2: Continuous
- Temperature: Every 30 minutes
- Urine output: Hourly via Foley catheter
- Neurological status: Every 15 minutes
Recovery room vitals (30 min post-surgery):
- BP: 124/72 mmHg
- HR: 82/min
- SpO2: 99%
- Temperature: 37.2°C
- Pain score (NRS): 1/10 (epidural working well)
- Sensory level: T8 (receding appropriately)
18.2 Postoperative Analgesia
- Epidural infusion (commenced intraop): Inj. Bupivacaine 0.1% + Fentanyl 2 mcg/mL at 8 mL/hr (PCEA mode with 3 mL bolus, 30-min lockout)
- Inj. Paracetamol 1 g IV q6h (non-opioid adjunct; safe in hyperthyroid patient)
- Tab. Ibuprofen 400 mg q8h (from Day 2 if Hb adequate and renal function normal)
- Epidural catheter to be removed at 48 hours (standard post-surgical protocol)
18.3 Thyroid Storm Surveillance
- Temperature monitored 4-hourly for 48 hours
- Peak risk: 6-24 hours postoperatively (Morgan & Mikhail 7e)
- Continue Carbimazole 15 mg via NGT/orally as early as possible post-surgery
- Continue Propranolol 40 mg BD orally (restart once tolerating oral fluids)
- Endocrinology notified of surgery; will review on postoperative Day 1
18.4 Lower Limb Neurology Check (Lithotomy Position Protocol)
| Assessment | Finding at 2 Hours Post-Surgery |
|---|---|
| Sensation in both lower limbs | Recovering (T10-L1 level, bilateral) |
| Motor power (Bromage) | Grade 1 (returning) |
| Dorsiflexion power (peroneal nerve) | Intact bilaterally |
| Medial calf sensation (saphenous nerve) | Intact bilaterally |
| Posterior thigh sensation (sciatic nerve) | Intact bilaterally |
| Calf compartment tension | Soft bilaterally |
CK level at 6 hours: 148 U/L (normal <200 U/L) - no rhabdomyolysis
18.5 Other Postoperative Orders
- Deep breathing exercises and incentive spirometry (every 2 hours)
- Early ambulation: Sit up at 24 hours; walk with assistance at 48 hours
- TED stockings + LMWH (Inj. Enoxaparin 40 mg SC OD from 12 hours postop) - VTE prophylaxis (TAH is high-risk)
- Hb recheck at 24 hours; reassess transfusion need
- NPO until bowel sounds return (~24-36 hours)
- IV fluids continue until oral intake adequate
- Foley catheter: In situ for 48 hours (TAH; urinary tract monitoring)
- Check serum electrolytes at 24 hours
18.6 Criteria for ICU/HDU Transfer (Not Required in This Patient)
Would have been required if:
- Thyroid storm developed intraoperatively
- Haemodynamic instability not responding to treatment
- Blood loss >1500 mL requiring >3 units PRBC
- ECG evidence of AF or ischaemia
This patient was transferred to high-dependency ward (Bed 8, Gynae HDU) for 24-hour monitoring and then to general ward on Day 2.
SECTION 19: POSTOPERATIVE COMPLICATIONS - NONE IN THIS PATIENT
| Complication | Status |
|---|---|
| Thyroid storm | Did NOT occur; TFTs repeated Day 1 - TSH 0.42, FT4 17.1 - stable |
| Haemorrhage | 1 unit PRBC transfused; Hb 9.2 on Day 1; no further bleeding |
| PDPH | Not present (pencil-point 25G Whitacre needle used) |
| Nerve injury | No neurological deficit documented at 24h and 48h check |
| Compartment syndrome | CK normal; calves soft |
| Ureteric injury | Urine clear; output adequate; no haematuria |
| DVT/PE | No clinical features; on LMWH prophylaxis |
| Nausea/Vomiting | Mild; controlled with Ondansetron 4 mg IV |
SECTION 20: DISCHARGE SUMMARY (Day 5)
- Patient discharged on Day 5 in stable condition
- Continue: Tab. Carbimazole 15 mg OD + Tab. Propranolol 40 mg BD
- Follow-up with endocrinology in 4 weeks (TFT reassessment; may reduce Carbimazole dose)
- Follow-up with gynaecology in 2 weeks (wound check, histopathology review)
- Return immediately if: fever, palpitations, extreme anxiety, tremors (signs of thyroid storm)
SECTION 21: DISCUSSION POINTS (For Oral Examination)
Q1. Why CSE was chosen over GA for this patient?
CSE avoids laryngoscopy and intubation, thereby preventing the catecholamine surge that would exacerbate tachycardia, hypertension, and risk of arrhythmias in a hyperthyroid patient. It provides a superior postoperative analgesic profile via the epidural catheter, reducing the sympathetic response to pain in the postoperative period - a period of maximum thyroid storm risk (6-24 hours). GA with ketamine is absolutely contraindicated in hyperthyroid patients.
Q2. What is the level of spinal block required for TAH?
T4 bilaterally - to cover the peritoneum and upper abdominal manipulation during uterine delivery. The epidural catheter allows extension or maintenance of the block if surgery is prolonged beyond the duration of the intrathecal bupivacaine.
Q3. Why is phenylephrine the preferred vasopressor in this patient?
Phenylephrine is a pure alpha-1 adrenergic agonist. It raises blood pressure by vasoconstriction without stimulating beta receptors. In hyperthyroid patients, catecholamine sensitivity is increased (increased beta-adrenergic receptor density reported). Indirect agents such as ephedrine release endogenous catecholamines and may precipitate severe tachycardia and hypertension. (Miller's Anaesthesia 10e)
Q4. What is the mandatory BP check rule in lithotomy?
Blood pressure MUST be measured immediately after lowering the legs from lithotomy position. Sudden leg lowering causes acute reduction in venous return, cardiac output, and blood pressure - exacerbated by vasodilation from neuraxial anaesthesia. Failure to check can result in unrecognised hypotension. (Morgan & Mikhail 7e)
Q5. How do you distinguish thyroid storm from malignant hyperthermia intraoperatively?
| Feature | Thyroid Storm | Malignant Hyperthermia |
|---|---|---|
| Muscle rigidity | Absent | Present (masseter spasm, generalised) |
| Creatine kinase | Normal or mildly elevated | Markedly elevated (thousands of U/L) |
| Lactic acidosis | Absent | Present (metabolic acidosis, high lactate) |
| Respiratory acidosis | Absent | Present |
| Response to dantrolene | No response | Dramatic response |
| Triggering agent | Surgery/stress (not volatile agents) | Succinylcholine, volatile halogenated agents |
| Treatment | PTU, iodide, beta-blockade, steroids, cooling | Dantrolene, cooling, bicarbonate, hyperventilate |
(Morgan & Mikhail 7e; Miller's 10e)
Q6. What are the specific risks of lithotomy position in this patient?
The hyperthyroid myopathy and potential myasthenic-type weakness increase nerve vulnerability in lithotomy. The high-output cardiac state makes haemodynamic shifts at leg elevation and lowering more pronounced. Temperature monitoring is critical as the hyperdynamic state raises baseline metabolic rate and any storm-related hyperthermia could be masked.
REFERENCES
- Morgan & Mikhail's Clinical Anaesthesiology, 7th Edition - Chapter 32 (Lithotomy position, p.1298-1300); Chapter 56 (Thyroid and Parathyroid Disease)
- Miller's Anaesthesia, 10th Edition - Thyroid Disease chapter, p.4251-4253; Combined Spinal-Epidural Anaesthesia
- Barash, Cullen & Stoelting's Clinical Anaesthesia, 9th Edition - Chapter 47: Thyroid Disease (Table 47-3: Thyroid Storm Management, p.3992-3994); CSE Technique (p.2832-2833)
- Goldman-Cecil Medicine, 26th Edition - Thyroid Storm/Crescendo Thyrotoxicosis
- Bailey and Love's Short Practice of Surgery, 28th Edition - Lithotomy and Lloyd-Davies position
ASA = American Society of Anesthesiologists; CSE = Combined Spinal-Epidural; TAH = Total Abdominal Hysterectomy; BSO = Bilateral Salpingo-Oophorectomy; TFT = Thyroid Function Tests; PTU = Propylthiouracil; LOR = Loss of Resistance; PACU = Post-Anaesthesia Care Unit; LMWH = Low Molecular Weight Heparin; PRBC = Packed Red Blood Cells; PDPH = Post-Dural Puncture Headache; MH = Malignant Hyperthermia
Anesthesia inhaled uptake and distribution, from stoeltings and millers
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have everything needed for a thorough, well-sourced answer. Let me compose the full response.
Inhaled Anaesthetic Uptake and Distribution
From Miller's Anaesthesia (10th ed.) and Barash's Clinical Anaesthesia (9th ed.)
THE FA/FI CONCEPT - THE FOUNDATION
The most clinically useful way to track uptake is the ratio of the alveolar anesthetic fraction (FA) to the inspired fraction (FI) plotted against time. The faster FA rises toward FI, the faster the speed of induction - because FA is directly proportional to the partial pressure of anesthetic in the CNS:
FA = PA / Pbarometric, and PA = Pblood = PCNS
(Barash 9e, p.1388)
The classic FA/FI curves (Barash Fig. 18-2) show that the least soluble agents (N₂O, desflurane, sevoflurane) rise fastest toward FI, while the most soluble agent (halothane) rises most slowly:
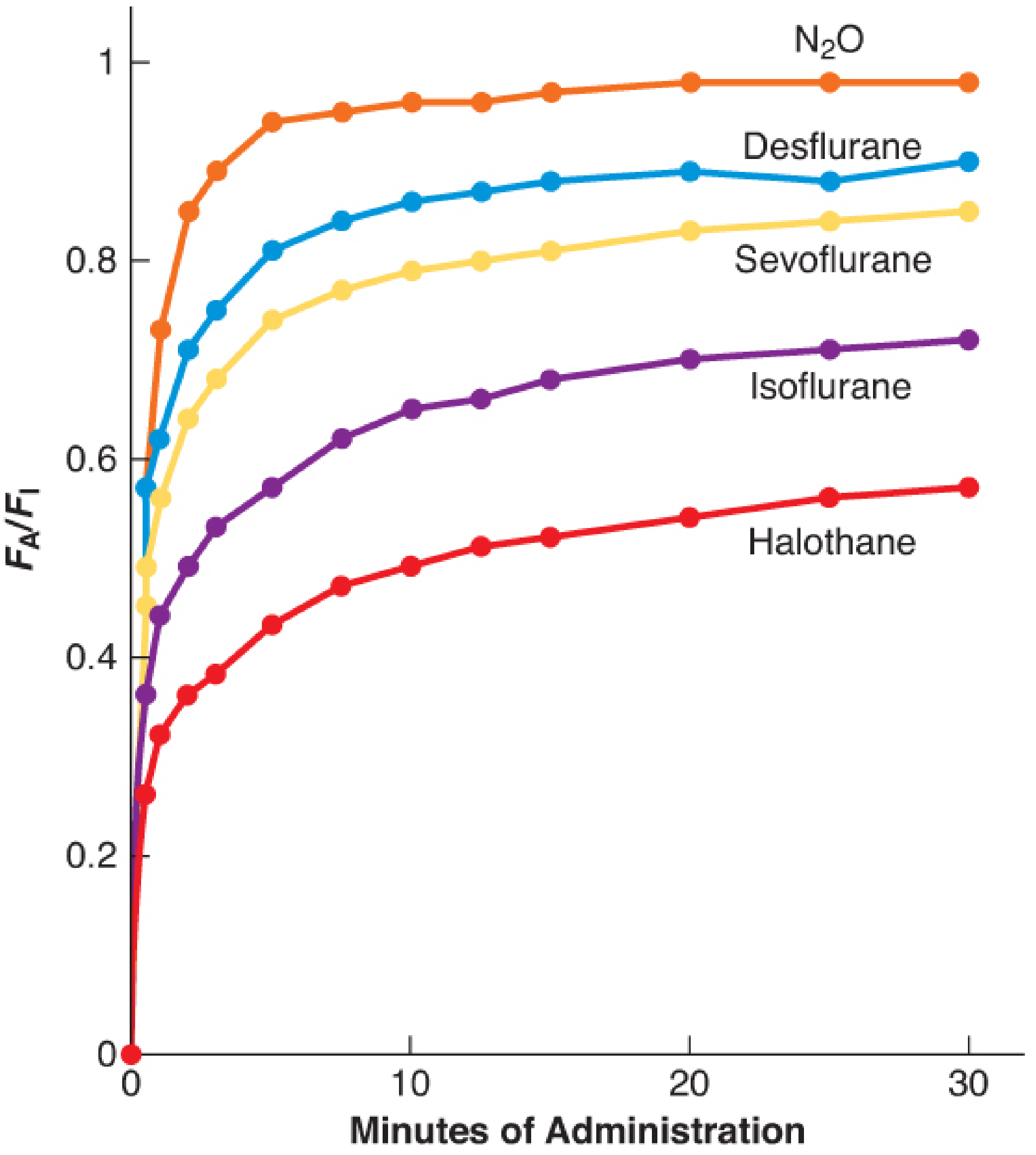
Figure 18-2 (Barash 9e): Rise in alveolar (FA) anesthetic concentration toward inspired (FI) concentration. Data from human studies. N₂O and desflurane rise fastest; halothane slowest - directly reflecting blood:gas solubility.
THE MULTICOMPARTMENTAL MODEL (Miller's 10e)
Miller's describes uptake and distribution as a series of transfer steps from upstream to downstream compartments, each driven by partial pressure gradients:
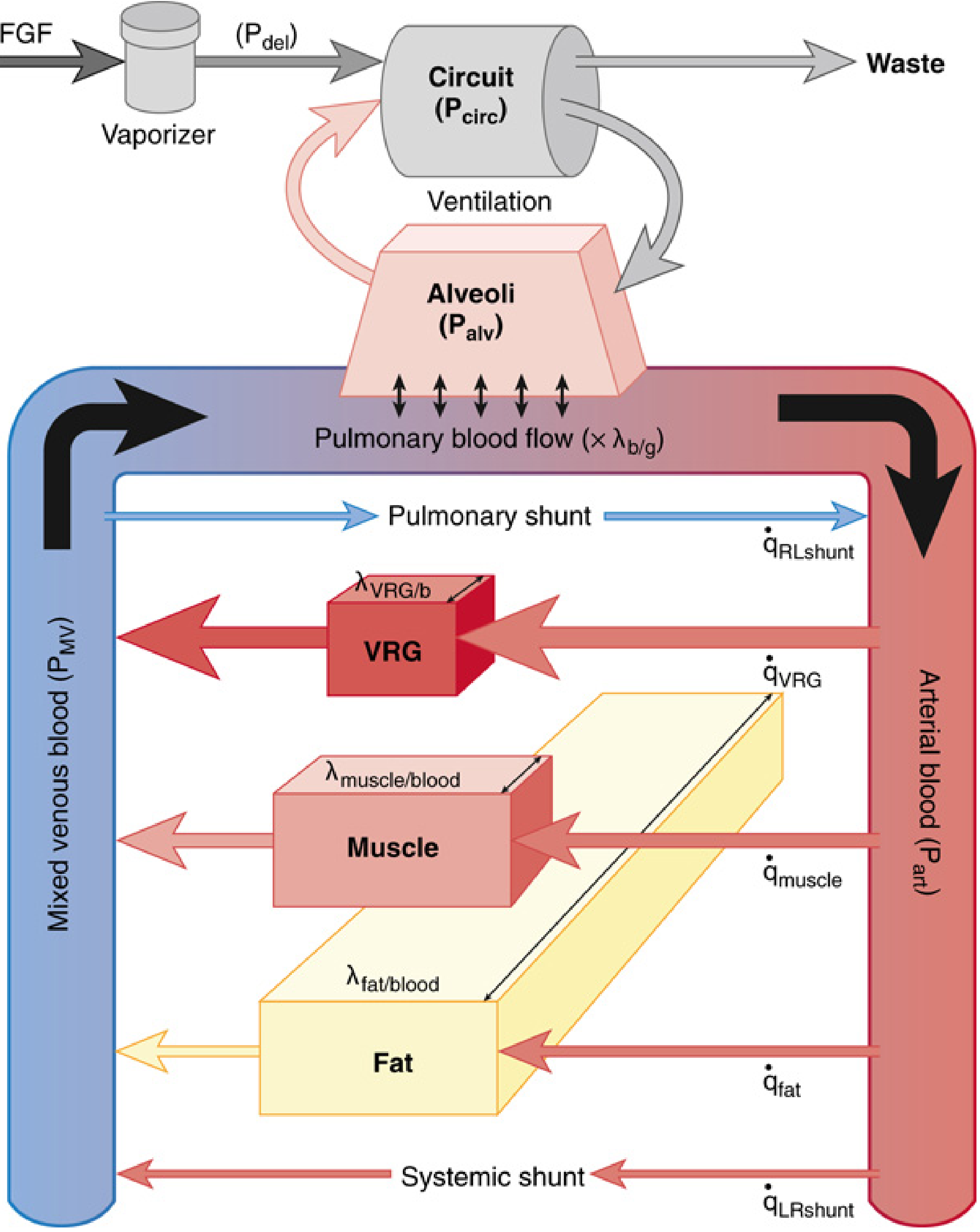
FIG. 18.2 (Miller's 10e): Flow diagram for uptake and distribution of inhaled anesthetics. Compartments include breathing circuit, alveolar gas, and three major tissue groups: VRG, muscle, and fat. Tissue compartments are shown in proportion to their physiological volumes.
The six sequential transfer steps are:
- Vaporizer → breathing circuit (fresh gas flow)
- Circuit → alveolar airspace (ventilation)
- Alveolar gas → pulmonary capillary blood (transcapillary diffusion)
- Arterial blood → body tissues, including CNS (distribution)
- Venous outflow from tissues → pulmonary artery (return)
- Mixed venous blood → re-equilibrates with alveolar gas
(Miller's Anaesthesia 10e, p.1927-1928)
PART 1: BIOPHYSICAL PROPERTIES - PARTIAL PRESSURE AND PARTITION COEFFICIENTS
Partial Pressure
- Partial pressure is the portion of total pressure contributed by one gas component; it is the thermodynamic force driving gas transfer between compartments
- Anesthetics move from high to low partial pressure, regardless of other gas components
- Equilibrium is reached when partial pressure is equal across compartments
- Example: 1.5% isoflurane in air at 760 mmHg = isoflurane at 11.4 mmHg
- At high altitude, the same inhaled percentage delivers a lower absolute partial pressure and therefore a reduced pharmacologic effect (Miller's 10e, p.1922-1923)
Partition Coefficients (λ)
A partition coefficient is the ratio of anesthetic concentration in two adjacent compartments at equilibrium (equal partial pressure). It represents the relative capacity of each compartment to hold the anesthetic.
| Agent | Blood:Gas (λb/g) | Brain:Blood | Muscle:Blood | Fat:Blood |
|---|---|---|---|---|
| Nitrous oxide | 0.46 | 1.1 | 1.2 | 2.3 |
| Desflurane | 0.42 | 1.3 | 2.0 | 27 |
| Sevoflurane | 0.65 | 1.7 | 3.1 | 48 |
| Isoflurane | 1.4 | 2.6 | 4.0 | 45 |
| Halothane | 2.4 | 2.9 | 3.4 | 51 |
(Barash 9e, Table 18-1)
Key principle: A high blood:gas partition coefficient means the blood has a high capacity to dissolve the agent, so alveolar concentration rises slowly (the blood "soaks up" more agent before equilibrium). A low blood:gas coefficient means the alveolus quickly reaches equilibrium with the delivered concentration → faster induction.
"The more soluble the inhaled anesthetic, the larger the capacity of the blood and tissues for that anesthetic, and the longer it takes to saturate at any given delivery rate." - Barash 9e, p.1390
PART 2: FACTORS DETERMINING FA/FI - INDUCTION PHARMACOKINETICS
Step 1: From Vaporizer to Breathing Circuit
Fresh gas from the vaporizer flows into the circuit. Using first-order kinetics:
FI = FFGO × (1 - e^(-T/τ))
where τ (time constant) = Circuit volume / Fresh gas flow rate
Example: Circuit volume 8 L, FGF 2 L/min → τ = 4 min. 95% equilibration requires 3τ = 12 minutes.
- Increasing FGF shortens τ and speeds rise of FI
- Overpressurization (setting vaporizer higher than target concentration) compensates for slow circuit filling - analogous to an IV bolus (Barash 9e, p.1388-1389)
Step 2: From Circuit to Alveoli - Effect of Ventilation
Minute ventilation (MV) drives anesthetic from the circuit into the alveolar airspace.
- Increasing MV accelerates the rise of FA toward FI
- The effect is greater for more soluble agents (e.g., halothane) because they have a larger driving gradient that ventilation can exploit
- Increased ventilation also accelerates washout during recovery
"Raising minute ventilation accelerates the rise of PA by delivering more anesthetic to the lungs. The effect is seen whether anesthetic is highly soluble in blood (e.g., halothane) or relatively insoluble (e.g., sevoflurane). However, the relative size of the ventilation effect is greater for soluble agents." - Miller's 10e, Fig. 18.4
Step 3: Alveolar Uptake into Blood - The Most Important Step
This is the dominant determinant of the FA/FI curve. Blood uptake is expressed as:
V̇B = λb/g × Q̇ × (PA - PV) / PB
where:
- λb/g = blood:gas partition coefficient (solubility)
- Q̇ = cardiac output
- PA = alveolar partial pressure
- PV = mixed venous partial pressure
- PB = barometric pressure
(Barash 9e, Eq. 18-9, p.1390)
Three factors thus determine alveolar uptake:
Factor A: Solubility (Blood:Gas Partition Coefficient)
This is the single most important determinant of induction speed.
- High λb/g (halothane 2.4): blood absorbs large quantities of agent → FA rises slowly → slow induction
- Low λb/g (desflurane 0.42): blood absorbs little agent → FA rises quickly → fast induction
Numerical example (Barash 9e): Suppose halothane and desflurane are delivered equally. If 50% of alveolar agent is taken up by blood:
- Halothane (λb/g = 2.5): 71.4% transfers to blood, only 28.6% remains in alveolus → FA is low
- Desflurane (λb/g = 0.42): only 29.6% transfers to blood, 70.4% remains in alveolus → FA is high
At equilibrium, FA of halothane = 28.6% of FI; FA of desflurane = 70.4% of FI. Desflurane FA/FI rises 2.4 times faster than halothane.
Factor B: Cardiac Output (Q̇)
- High cardiac output → more blood passes through the pulmonary capillaries per minute → more agent removed from alveoli → slower rise of FA → slower induction
- Low cardiac output → less blood-mediated removal → faster rise of FA → faster induction (but CNS drug delivery is also reduced, so the effect partially cancels)
Clinical implication:
- States of high CO (hyperthyroidism, pregnancy, anxiety, fever): slower alveolar rise - need higher delivered concentration
- States of low CO (shock, cardiac failure, hypovolemia): faster alveolar rise - induction may be unexpectedly rapid; overdose risk with soluble agents
"Patients with low cardiac output may absorb inhaled anesthetic faster; the alveolar partial pressure may rise more quickly... this is of particular concern with more soluble anesthetics." (Barash 9e)
The effect of cardiac output is much more pronounced with soluble agents (halothane, isoflurane) than insoluble agents (desflurane, N₂O).
Factor C: Alveolar-Venous Partial Pressure Difference (PA - PV)
- At induction start, PV = 0 (no drug in tissues); the gradient PA - PV is maximal → uptake is highest
- As tissues absorb drug, PV rises → gradient falls → uptake decreases → FA rises faster
- This is why FA/FI curves are steep initially then flatten (the characteristic "knee" shape)
The "first knee" in each FA/FI curve marks when PV starts rising significantly - i.e., when VRG tissues begin returning drug to venous blood (Barash 9e, p.1392)
PART 3: DISTRIBUTION INTO TISSUES
(Miller's Anaesthesia 10e, p.1949-1950)
After crossing the alveolar-capillary membrane, arterial blood distributes anesthetic to four tissue groups. The rate of equilibration for each tissue is governed by:
dP/dt = (blood flow / effective volume) × (Parteries - Ptissue)
where effective volume = anatomical volume × tissue:blood partition coefficient
Equilibration time constant (τ) = effective volume / blood flow
The Four Tissue Groups
| Group | Organs | % Body Mass | % Cardiac Output | Equilibration Time |
|---|---|---|---|---|
| Vessel-Rich Group (VRG) | Brain, heart, liver, kidney, spinal cord | ~10% | ~70% | Minutes |
| Muscle Group | Skeletal muscle | ~40% | 10-15% | Hours |
| Fat Group | Adipose tissue | <25% | ~10% | Days |
| Vessel-Poor Group (VPT) | Bone, cartilage, connective tissue, skin | 10-15% | <5% | Very slow |
(Miller's 10e, Table 18.2)
Vessel-Rich Group (VRG) - Clinical Target
- Receives ~70% of cardiac output despite being only 10% of body mass
- Tissue perfusion: ~75 mL/min per 100 g of tissue (brain)
- Equilibrates within a few minutes → this is why induction is clinically rapid
- The CNS (primary target) is within the VRG; PCNS = Pblood = Palveolar at equilibration
Muscle Group
- Largest single compartment by mass (~40%)
- Perfusion: only 3 mL/min per 100 g - 25× less than VRG
- Muscle:blood partition coefficients ~2× higher than brain:blood
- Combined effect: equilibration takes hours
- Slow muscle uptake means it continues absorbing drug during prolonged anaesthesia
Fat Group
- Highly lipid-soluble volatile agents partition avidly into fat (fat:blood coefficients = 27-51 for most volatile agents)
- Fat represents the largest effective volume for potent volatile agents
- Despite only ~10% of cardiac output, the immense effective volume gives equilibration times of days
- Not clinically significant for induction speed
- Very significant for recovery after prolonged anaesthesia (>4 hours) - fat acts as a reservoir releasing drug back into blood
"After long anesthetic exposures (>4 hours), the high saturation of fat tissue may play a role in delaying emergence." - Barash 9e, p.1392
Nitrous oxide is an exception: Its partition coefficients are similar across all tissue types (not highly lipid-soluble), so it does not accumulate in fat and equilibrates relatively quickly across all compartments.
PART 4: SPECIAL EFFECTS
The Concentration Effect
When a high inspired concentration of an anesthetic is administered, FA rises more rapidly than predicted from simple uptake. This arises from two mechanisms:
1. The Concentrating Effect:
When a large fraction of alveolar gas is absorbed (high inspired concentration, highly absorbed agent like N₂O), the remaining gas is concentrated into a smaller volume. The anesthetic remaining constitutes a higher fraction of a smaller total gas volume → FA increases disproportionately.
Example (Barash 9e): Delivering 10% anesthetic, with 50% absorbed:
- 5 parts anesthetic + 45 parts other gas remain → anesthetic = 10% of remaining volume
- Compare to 1% anesthetic delivered: 0.5 parts absorbed, 0.5 parts + 99 parts other gas remain → only 0.5% of remaining volume
2. Augmented Inflow Effect:
As large volumes of gas are absorbed, additional gas must rush in to fill the space, effectively augmenting alveolar ventilation → more fresh anesthetic delivered per unit time.
Both effects are only clinically significant with high concentration agents (primarily N₂O at 60-75%) because volatile agents are delivered at only 1-3% concentrations, making these effects negligible. (Miller's 10e; Barash 9e, p.1692-1694)
The Second Gas Effect
When N₂O is administered at high concentrations alongside a volatile agent ("second gas"):
- Rapid uptake of N₂O into blood concentrates the second gas in the alveolus
- Augmented inflow of fresh gas further increases second gas delivery
- Result: FA of the volatile agent (e.g., isoflurane) rises faster than it would alone
The second gas effect also increases PaO₂ initially, as alveolar O₂ is concentrated alongside the volatile agent.
"The second gas effect is greater in arterial blood than in expired gas, influenced by the blood solubility of VAs, and significantly affects anesthetic onset." - Miller's 10e, p.1948
PART 5: FACTORS AFFECTING SPEED OF INDUCTION - SUMMARY TABLE
| Factor | Change | Effect on FA/FI Rise | Clinical Example |
|---|---|---|---|
| Blood:gas solubility | ↑ (more soluble) | Slower | Halothane slower than desflurane |
| Blood:gas solubility | ↓ (less soluble) | Faster | Desflurane, N₂O fast onset |
| Alveolar ventilation | ↑ | Faster | Hyperventilation speeds induction |
| Alveolar ventilation | ↓ | Slower | Hypoventilation, COPD |
| Cardiac output | ↑ | Slower | Hyperthyroid, pregnant, anxious |
| Cardiac output | ↓ | Faster (overdose risk!) | Shock, cardiac failure |
| Inspired concentration | ↑ | Faster | Overpressurization technique |
| FRC / pulmonary volume | ↑ | Slower | Obese → smaller FRC actually speeds it |
| V/Q mismatch | Increases | Slows induction of insoluble agents more | R→L shunt |
| Metabolism | Increases | Slightly faster | Minimal effect at clinical doses |
PART 6: RECOVERY - WASHOUT PHARMACOKINETICS
(Barash 9e, p.1401)
Recovery from anaesthesia mirrors induction but with two critical asymmetries:
Asymmetry 1 - No "underpressurization":
During induction, the inspired concentration can be set higher than the target (overpressurization). During recovery, FA cannot fall below zero. There is no equivalent manoeuvre to speed washout.
Asymmetry 2 - Tissues begin recovery at different partial pressures:
- VRG (brain, heart, liver) begins recovery at full equilibration with alveoli (PCNS = Pblood = Palveoli)
- Muscle and fat begin recovery with variable partial pressures depending on duration of anaesthesia
- After short anaesthesia, muscle and fat have low anesthetic content → little redistribution back to blood
- After prolonged anaesthesia, fat contains large reservoir of agent; even after alveolar clearance, fat continues to release agent back into blood for hours → delayed emergence
Clinical consequence: Recovery with desflurane and sevoflurane is largely duration-independent because their low solubility means fat never accumulates significant amounts. Recovery with isoflurane (and especially halothane) is duration-dependent - longer surgery means delayed waking.
"With the less soluble anesthetic sevoflurane, the time to orientation was independent of the anesthetic duration. In contrast, long anesthetic durations with isoflurane were associated with delayed times to orientation." - Barash 9e (citing Ebert et al., Anesthesiology 1998)
PART 7: DIFFUSION HYPOXIA
At the end of anaesthesia, when N₂O is discontinued, large volumes of N₂O rapidly wash out from blood into the alveolus. This dilutes alveolar O₂ and CO₂:
- Diluted O₂ → alveolar hypoxia → arterial hypoxaemia
- Diluted CO₂ → alveolar hypocarbia → reduced respiratory drive → worsens hypoxaemia
Management: Administer 100% oxygen for 3-5 minutes at the end of N₂O anaesthesia before switching to room air or lower FiO₂.
(Barash 9e, p.1401; also Morgan & Mikhail 7e)
PART 8: EFFECT OF VENTILATION-PERFUSION MISMATCH
V/Q mismatch affects insoluble and soluble agents differently:
- With right-to-left (pulmonary) shunt: blood passes from pulmonary artery to pulmonary vein without gas exchange → carries no anesthetic → dilutes arterial concentration → slows induction
- This effect is greater for insoluble agents (e.g., N₂O, desflurane) - because their arterial uptake depends almost entirely on alveolar exchange. Soluble agents (halothane) are less affected because blood can still absorb agent from other gas exchange units.
- With dead space (high V/Q): relatively minor effect on induction
(Miller's 10e)
QUICK REFERENCE SUMMARY
UPTAKE = λb/g × Q̇ × (PA - PV) / PB
The three determinants of blood uptake:
1. Solubility (λb/g) → Most important
2. Cardiac output (Q̇)
3. Alveolar-venous gradient (PA - PV)
More uptake = slower rise of FA = slower induction
Four tissue groups (time to equilibrate):
VRG (brain, liver, heart) → minutes ← clinical induction endpoint
Muscle → hours
Fat → days ← recovery after long cases
Vessel-poor (bone, skin) → very slow
Special effects (N₂O only, clinically significant):
Concentration effect → faster FA/FI rise at high [N₂O]
Second gas effect → speeds codelivered volatile agent
Diffusion hypoxia → give 100% O₂ on N₂O discontinuation
Sources:
- Miller's Anaesthesia, 10th Edition - Chapter 18: Uptake and Distribution of Inhaled Anesthetics (p.1922-1955), including multicompartmental model, biophysical properties, tissue distribution table (Table 18.2)
- Barash, Cullen & Stoelting's Clinical Anaesthesia, 9th Edition - Chapter 18: Inhaled Anesthetics - Uptake and Distribution, FA/FI curves (Fig. 18-2), concentration effect, tissue compartments (p.1386-1404)
This is a shared conversation. Sign in to Orris to start your own chat.