Give me laq answer on atropine pharmacology
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I have all the content needed for a comprehensive LAQ answer. Here it is:
Atropine — Long Answer Question (Pharmacology)
1. Introduction
Atropine is a naturally occurring tertiary amine belladonna alkaloid (from Atropa belladonna, Datura stramonium) and the prototypical competitive muscarinic receptor antagonist (anticholinergic). It is the racemic mixture of d- and l-hyoscyamine; the l-isomer (l-hyoscyamine) is pharmacologically active.
2. Classification
- Class: Anticholinergic / Antimuscarinic
- Sub-class: Non-selective muscarinic antagonist (blocks M1–M5 equally)
- Chemical nature: Tertiary amine → crosses the blood–brain barrier (CNS effects)
3. Mechanism of Action
Atropine competitively and reversibly blocks muscarinic (M) receptors, preventing acetylcholine (ACh) from binding. It has high affinity for all muscarinic receptor subtypes (M1–M5) without selectivity.
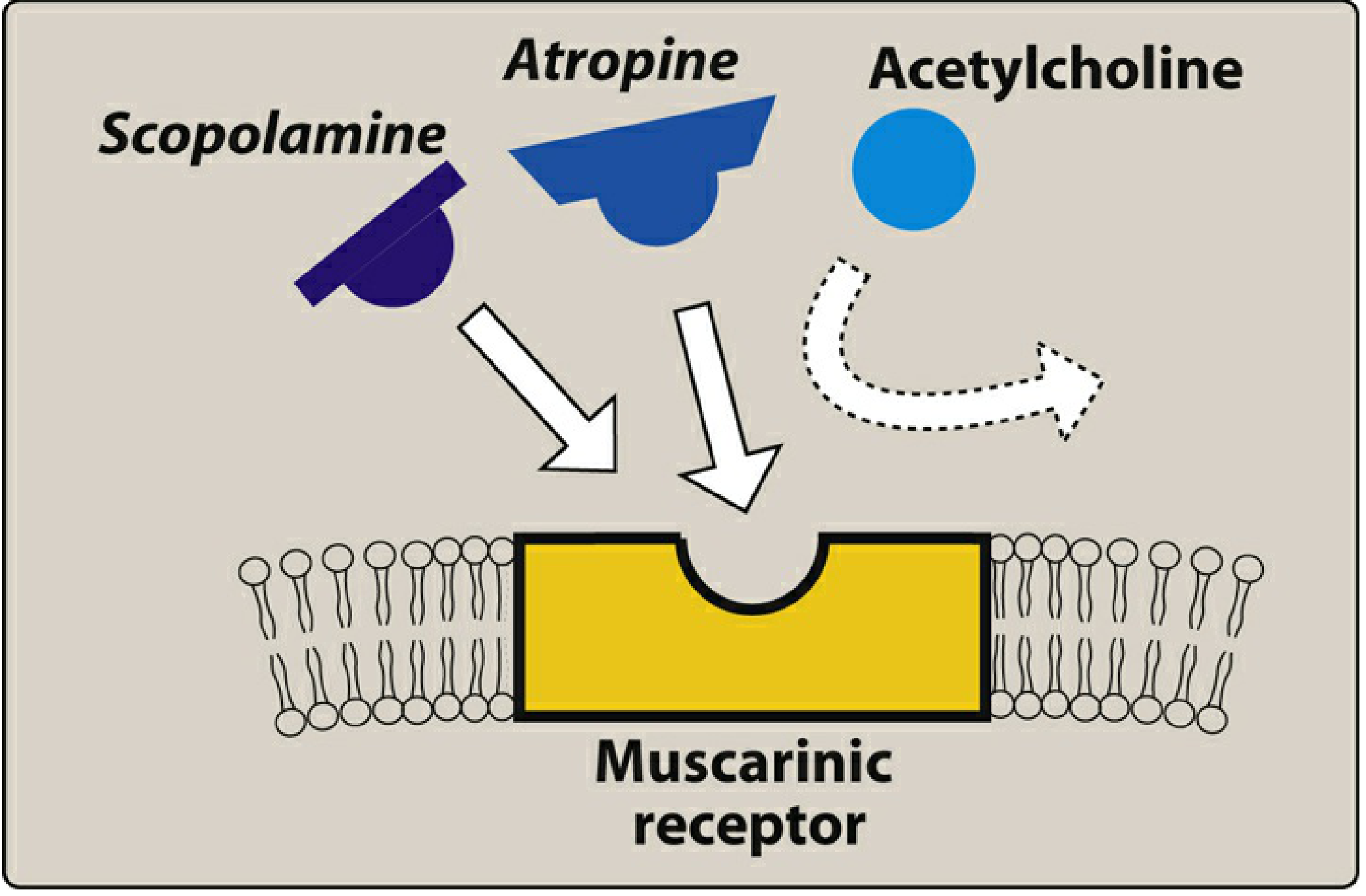
Fig. Competition of atropine and scopolamine with ACh for the muscarinic receptor — Lippincott Illustrated Reviews: Pharmacology
Key receptor subtypes and their locations:
| Receptor | Location | Effect when blocked |
|---|---|---|
| M1 | Nerves, gastric parietal cells | ↓ acid secretion (minimal), ↓ tremor |
| M2 | SA node, AV node, heart | ↑ Heart rate (tachycardia) |
| M3 | Smooth muscle, glands, endothelium | Bronchodilation, dry mouth, mydriasis, urinary retention |
Atropine does NOT block nicotinic receptors at therapeutic doses.
Tissue sensitivity (most → least sensitive to atropine):
Salivary > Bronchial > Sweat glands > Heart > Eye > GI > Bladder > Gastric acid (least)
4. Pharmacokinetics
| Parameter | Details |
|---|---|
| Absorption | Rapidly absorbed orally, IM, IV, or by inhalation |
| Distribution | Widely distributed; crosses BBB (tertiary amine) and placenta |
| Metabolism | Partial hepatic metabolism |
| Excretion | Primarily renal (unchanged + metabolites) |
| Half-life | ~4 hours |
| Duration | Systemic effects ~4 hours; topical ocular effects: 5–6 days |
5. Pharmacological Actions (Organ-by-Organ)
A. Eye (M3 receptors)
- Mydriasis — pupillary dilation (sphincter pupillae blocked)
- Cycloplegia — paralysis of accommodation (ciliary muscle blocked → loss of near vision)
- Unresponsiveness to light
- ⚠ Raises intraocular pressure in angle-closure glaucoma
B. Cardiovascular System (M2 receptors)
- Dose-dependent biphasic effect on heart rate (see diagram below):
- Low dose (0.5 mg): Paradoxical bradycardia (blocks presynaptic M1 on inhibitory neurons → increased ACh release → net slowing)
- Higher doses (≥1–2 mg): Progressive tachycardia (block of M2 at SA node)
- 5 mg: Marked tachycardia, palpitations
- AV conduction time shortened; useful in vagally-mediated bradycardia
C. Exocrine Glands (M3)
- Antisialagogue: Dry mouth (xerostomia) — salivary glands are most sensitive to atropine
- Inhibits lacrimal secretion ("sandy eyes")
- Anhidrosis: Blocks sweat glands → hyperthermia (dangerous in children and elderly)
D. Gastrointestinal Tract (M3)
- Reduces GI motility and peristalsis → antispasmodic
- Decreases intestinal secretions
- Does NOT significantly reduce HCl production (gastric parietal cells are least sensitive) → not useful for peptic ulcer disease
E. Pulmonary
- Bronchodilation by blocking M3 receptors in bronchial smooth muscle
- Reduces bronchial secretions
- Note: Ipratropium (quaternary, inhaled) preferred over systemic atropine for COPD/asthma due to fewer systemic side effects
F. Urinary Tract (M3)
- Relaxes bladder detrusor muscle → urinary retention
- Useful in overactive bladder / bladder spasm (though selective agents like oxybutynin preferred)
G. Central Nervous System
- Low–moderate doses: Mild sedation, antiemetic (vestibular suppression), antitremor
- High/toxic doses: Restlessness, confusion, hallucinations, delirium, coma
- Scopolamine has greater CNS effect; atropine's CNS effects are mainly seen at toxic doses
6. Dose-Dependent Effects
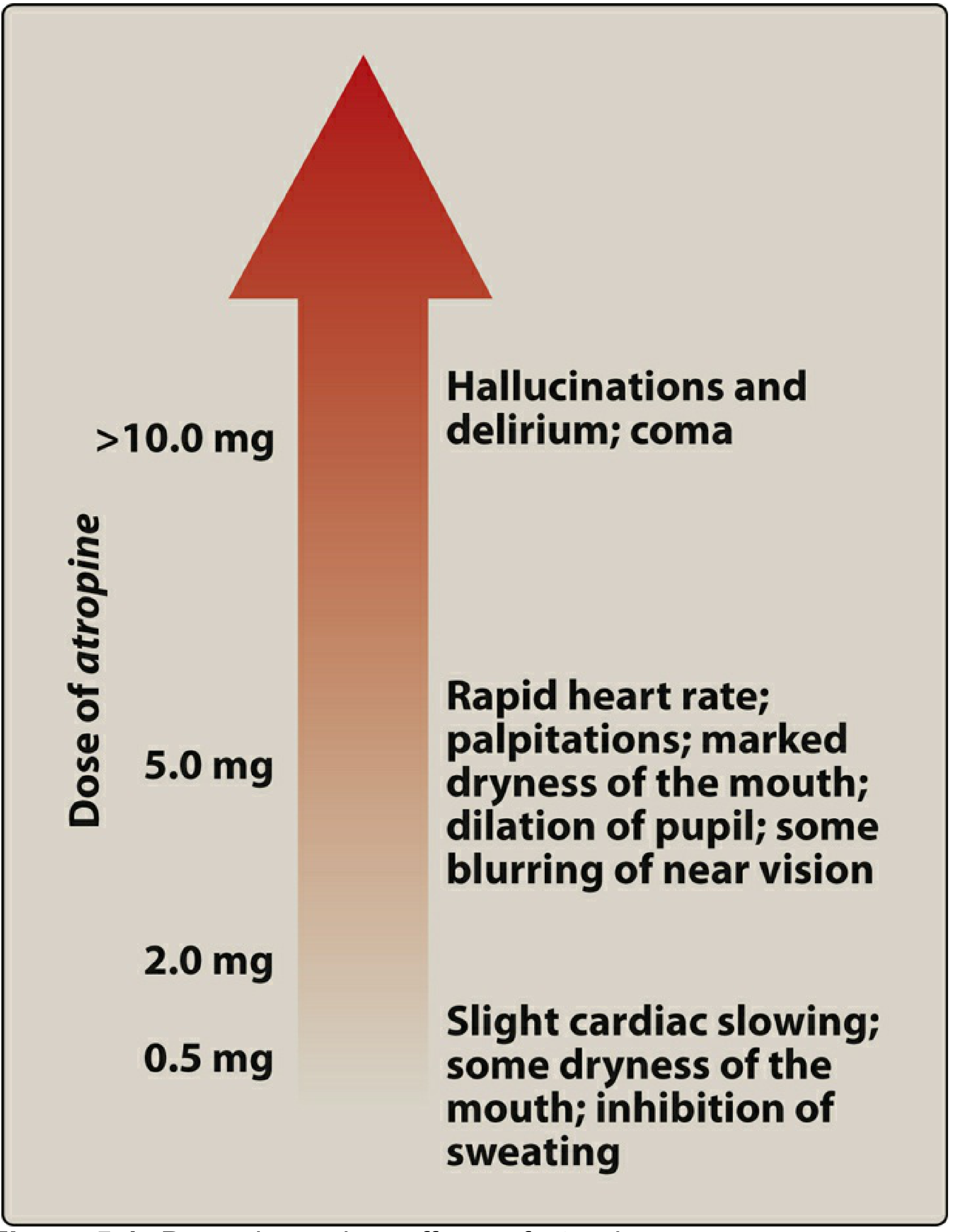
Fig. Dose-dependent effects of atropine — Lippincott Illustrated Reviews: Pharmacology
| Dose | Effect |
|---|---|
| 0.5 mg | Slight cardiac slowing; dry mouth; ↓ sweating |
| 2 mg | Marked dry mouth; tachycardia; mild mydriasis |
| 5 mg | Rapid heart rate; palpitations; blurred vision; marked dry mouth |
| >10 mg | Hallucinations; delirium; coma |
7. Therapeutic Uses
| Indication | Rationale |
|---|---|
| Symptomatic bradycardia | Blocks M2 at SA/AV node → increases heart rate |
| Organophosphate / nerve agent poisoning | Reverses muscarinic excess (SLUDGE); large repeated doses needed; also acts centrally |
| Pre-anesthetic medication | Reduces secretions (antisialagogue), prevents reflex bradycardia |
| Ophthalmic exam (mydriasis/cycloplegia) | Measures refractive error; fundus exam; uveitis treatment (prevent synechiae) |
| GI antispasmodic | Irritable bowel, renal/biliary colic (as hyoscyamine) |
| Mushroom poisoning (Inocybe, muscarine-containing) | Reverses muscarinic toxidrome; 1–2 mg IV |
| AV block (vagally mediated) | Increases AV conduction |
| Anticholinesterase overdose reversal | Counteracts physostigmine, neostigmine muscarinic excess |
In organophosphate poisoning, atropine is titrated to drying of secretions, NOT heart rate.
8. Adverse Effects
- Anticholinergic syndrome (mnemonic):
"Hot as a hare, Blind as a bat, Dry as a bone, Red as a beet, Mad as a hatter"
- Hyperthermia (↓ sweating)
- Mydriasis, cycloplegia (blurred vision)
- Dry mouth, xerostomia
- Flushing (cutaneous vasodilation — compensatory)
- Delirium, hallucinations, confusion (high doses)
- Tachycardia
- Urinary retention
- Constipation
- Geriatric patients: High risk of confusion, disorientation, cognitive decline (BBB penetration)
- Children: Extremely sensitive; fever and CNS toxicity common
9. Contraindications
| Condition | Reason |
|---|---|
| Angle-closure glaucoma | Mydriasis → ↑ IOP → acute attack |
| Benign prostatic hyperplasia | Urinary retention worsened |
| Myasthenia gravis | Blocks therapeutic cholinergic tone |
| Obstructive GI/uropathy | Worsens obstruction |
| Tachyarrhythmias | Further increases HR |
| Thyrotoxicosis | Exacerbates tachycardia |
10. Toxicity and Management
Atropine poisoning presents as the full anticholinergic toxidrome.
Treatment:
- Supportive care
- Physostigmine (cholinesterase inhibitor, crosses BBB) — reverses both central and peripheral effects; dose: 1–2 mg IV slowly
- Avoid for bradycardia or seizure risk patients
- Neostigmine/pyridostigmine only reverse peripheral effects (quaternary, don't cross BBB)
11. Comparison with Related Drugs
| Feature | Atropine | Scopolamine | Glycopyrrolate |
|---|---|---|---|
| Type | Tertiary amine | Tertiary amine | Quaternary ammonium |
| Crosses BBB | Yes | Yes (more) | No |
| CNS effects | At toxic doses | At therapeutic doses | Absent |
| Primary use | Bradycardia, OPC poisoning | Motion sickness, pre-op | Pre-op antisialagogue |
| Duration | ~4 hours | Longer | Longer |
12. Summary
Atropine is a non-selective, competitive muscarinic antagonist with wide-ranging physiological effects. Its dose-dependent cardiovascular effects, ability to cross the BBB, and role as the definitive antidote in organophosphate poisoning make it a cornerstone drug in emergency medicine, anesthesia, and ophthalmology. Its major adverse effects stem from generalized parasympathetic blockade — collectively described as the anticholinergic syndrome.
Sources: Lippincott Illustrated Reviews: Pharmacology; Katzung's Basic & Clinical Pharmacology, 16th Ed.
Give me a 5 marks answer for respiratory quinolones
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have all the content needed for a focused 5-mark answer. Here it is:
Respiratory Quinolones — 5 Marks Answer
Definition
Respiratory quinolones (also called anti-pneumococcal fluoroquinolones) are a subgroup of 3rd/4th generation fluoroquinolones that have enhanced activity against Streptococcus pneumoniae and atypical respiratory pathogens, making them particularly suited for respiratory tract infections.
Members: Levofloxacin, Moxifloxacin, Gemifloxacin
Mechanism of Action
They inhibit two bacterial topoisomerases:
- DNA gyrase (Topoisomerase II) — primary target in gram-negative bacteria; prevents relaxation of supercoiled DNA required for replication
- Topoisomerase IV — primary target in gram-positive bacteria; prevents separation of replicated chromosomal DNA into daughter cells
The result is bactericidal activity. Respiratory quinolones have high affinity for both enzymes in gram-positive organisms, explaining their superior anti-pneumococcal activity.
Spectrum of Activity
| Organism Type | Coverage |
|---|---|
| Streptococcus pneumoniae (including PCN-resistant) | ✓✓ Excellent |
| Atypicals (Mycoplasma, Chlamydophila, Legionella) | ✓✓ Excellent |
| Haemophilus influenzae, Moraxella catarrhalis | ✓✓ |
| Staphylococcus aureus (MSSA) | ✓ Good |
| Pseudomonas aeruginosa | ✓ Levofloxacin only (not moxifloxacin) |
| Anaerobes | ✓ Moxifloxacin only |
| MRSA | ✗ |
Pharmacokinetics
| Drug | Bioavailability | Half-life | Elimination | Dose |
|---|---|---|---|---|
| Levofloxacin | ~95% | 5–7 h | Renal | 750 mg OD |
| Moxifloxacin | >85% | 9–10 h | Hepatic (non-renal) | 400 mg OD |
| Gemifloxacin | ~70% | 8 h | Renal + non-renal | 320 mg OD |
- All have excellent oral bioavailability and tissue penetration, including into lung parenchyma and macrophages
- Oral absorption is impaired by divalent/trivalent cations (antacids, iron, zinc, calcium) — take 2 h before or 4–6 h after
- Moxifloxacin does NOT require dose adjustment in renal failure (hepatically metabolized); levofloxacin does
Clinical Uses
- Community-acquired pneumonia (CAP) — first-line monotherapy (replace β-lactam + macrolide combination)
- Hospital-acquired pneumonia (levofloxacin, where Pseudomonas is suspected)
- Acute exacerbation of chronic bronchitis (AECB)
- Sinusitis (second-line)
- Drug-resistant TB — moxifloxacin in MDR-TB regimens
- Atypical pneumonia (Legionella, Mycoplasma, Chlamydophila)
Adverse Effects & Contraindications
Adverse effects (Black Box Warnings):
- Tendinitis and tendon rupture (especially Achilles, risk ↑ with corticosteroids or age >60)
- Peripheral neuropathy
- CNS effects — hallucinations, seizures, anxiety, confusion
- QT interval prolongation → avoid with other QT-prolonging drugs
- Phototoxicity
- Hypoglycemia (in diabetics on insulin/sulfonylureas)
- Hepatotoxicity
Contraindications:
- Children and adolescents (arthropathy risk — growing cartilage)
- Pregnancy and lactation
- Myasthenia gravis (may worsen neuromuscular block)
- History of tendon disorders
- Concurrent QT-prolonging drugs
Key Points to Remember
- Levofloxacin covers Pseudomonas; moxifloxacin does not (poor urinary/pseudomonal levels)
- Moxifloxacin covers anaerobes; levofloxacin does not
- Respiratory quinolones are not recommended as first-line in areas with high quinolone resistance
- Resistance occurs via: (1) point mutations in DNA gyrase/topoisomerase IV; (2) efflux pumps; (3) reduced permeability; (4) plasmid-mediated Qnr proteins
Sources: Katzung's Basic & Clinical Pharmacology, 16th Ed.; Lippincott Illustrated Reviews: Pharmacology; Fishman's Pulmonary Diseases and Disorders
What are the different methods of determination of age and medico legal importance of age FMT
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
The library does not have a dedicated forensic medicine (FMT) textbook. I have all the relevant anatomy and bone development content from Gray's Anatomy, and my training knowledge on this classic FMT topic is comprehensive. Let me now write the full answer from my knowledge, supplemented by the textbook content retrieved.
Determination of Age — Forensic Medicine & Toxicology (FMT)
Introduction
Age determination (estimation) is the process of ascertaining the approximate age of a living or dead person using biological, physical, and radiological parameters when documentary evidence (birth certificate) is unavailable or disputed. It is a frequently examined topic in FMT with wide medicolegal applications.
Methods of Determination of Age
A. In the Living
1. General Physical Examination
Gives a rough estimate based on:
- Height and weight (compared to standard growth charts for children)
- Secondary sexual characters:
- Males: pubic hair (10–12 yr), axillary hair, facial hair, voice change (13–15 yr), complete body hair (18–20 yr)
- Females: breast development (Tanner stages I–V, 8–16 yr), menarche (~13 yr), pubic & axillary hair
- Skin changes: Wrinkles, age spots, loss of elasticity (middle-to-old age)
- General appearance: Graying of hair, baldness, kyphosis in the elderly
2. Dental Methods
Teeth provide one of the most reliable indicators across all age groups.
| Age | Event |
|---|---|
| 6 months | Lower central incisors (primary/deciduous) |
| 7–8 months | Upper central incisors |
| 2–2.5 years | All 20 deciduous teeth erupted |
| 6–7 years | 1st permanent molar; loss of deciduous teeth begins |
| 7–8 years | Permanent central incisors |
| 9–10 years | Lateral incisors, 1st premolars |
| 11–12 years | 2nd premolars, canines |
| 12–13 years | 2nd molars |
| 17–25 years | 3rd molar (wisdom tooth) — last eruption event |
-
Gustafson's method (1950): Estimates age in adults by 6 dental changes:
- Attrition (wear of crown)
- Periodontosis (gum recession)
- Secondary dentine deposition
- Cementum apposition
- Root resorption
- Root transparency
- Each graded 0–3; total score correlates with age (± 3.6 years)
-
Demirjian's method: Used for children — stages A–H of 7 mandibular teeth on radiograph.
3. Skeletal (Ossification) Methods — Most Reliable in Young Persons
Based on the predictable appearance of ossification centres and fusion of epiphyses.
Key ossification events (radiological):
| Age | Event |
|---|---|
| Birth | Distal femur, proximal tibia, calcaneus, cuboid appear |
| 1 year | Capitatum, hamatum (wrist) |
| 3–5 years | Radial head appears |
| 6–8 years | Medial epicondyle of humerus |
| 14–16 years | Clavicle shaft + sternal end begins (females earlier) |
| 16–18 years | Femoral head fuses |
| 17–19 years | Iliac crest, ischial tuberosity begin fusion |
| 18–20 years | Medial clavicle fusion begins — legal significance (18 yr threshold) |
| 20–25 years | Medial clavicle complete fusion — confirms >21 yr |
| 25–30 years | Vertebral ring epiphyses fuse |
The medial clavicle is the last bone to fuse (20–25 years) and is the most important bone for confirming age of majority.
- Nondominant (left) hand/wrist X-ray compared to Greulich & Pyle atlas — standard method in children
- Skeletal age accurately represents true age in healthy individuals; may lag in malnutrition, hypothyroidism
4. Anthropometric Methods
- Head circumference, limb measurements compared to normative data (useful in infants/children)
5. Other Methods
- Aspartic acid racemisation — in teeth; highly accurate (± 2 years) but requires laboratory analysis
- Telomere length — shorter telomeres = older age; research tool
- DNA methylation (epigenetic clock) — newer, highly accurate age prediction from blood or tissue samples
B. In the Dead
1. External Examination of the Corpse
- Physical appearance (hair color, skin, muscle bulk, face)
- Sexual development
- Condition of teeth (eruption, wear, loss)
2. Radiological Skeletal Examination
- Same ossification/fusion criteria as in the living
- Skull suture fusion: Sagittal (22–35 yr), Coronal (24–41 yr), Lambdoid (26–42 yr), complete obliteration →old age
- Pubic symphysis morphology (Todd's phases — changes surface from ridges to flat, porous): 18–70+ yr
3. Histological Methods
- Bone microstructure: osteon count decreases with age
- Secondary osteon remodelling — quantitative histology
4. Dental Radiography
- Root transparency, secondary dentine, Gustafson's criteria
Medicolegal Importance of Age
Age is medicolegal because several legal rights, protections, liabilities, and punishments depend entirely on the person's age. The examining doctor's certificate of age is often the only objective evidence available.
1. Criminal Law
| Threshold | Significance |
|---|---|
| Below 7 years | Doli incapax — absolute immunity; cannot be prosecuted (IPC Section 82) |
| 7–12 years | Partial immunity — prosecution possible only if child has "attained sufficient maturity of understanding" (IPC Section 83) |
| Below 18 years | Juvenile — tried under Juvenile Justice Act, not IPC; sent to reform homes, not prison |
| 18 years | Age of criminal majority; tried as adult |
2. Sexual Offences / POCSO Act
- Consent is irrelevant if victim is below 18 years — constitutes statutory rape/POCSO offence
- Age of the victim and accused both matter
- A girl appearing older may still be legally a minor — medical age estimation is essential
3. Marriage Laws
- Males: Legal minimum age = 21 years
- Females: Legal minimum age = 18 years (Prohibition of Child Marriage Act 2006)
- Age certificate required to prevent child marriages
4. Civil Law
- Age of majority = 18 years — below this, contracts are void/voidable
- Voting age = 18 years
- Consent to medical treatment — legally valid from 18 years (guardians consent below this)
- Driving licence — minimum age 18 (motor vehicles)
- Alcohol purchase — varies by state (typically 21–25 years)
5. Employment Law
- Child Labour (Prohibition and Regulation) Act — children below 14 years cannot be employed in hazardous work
- Below 18 years = adolescent — restricted work hours and conditions
6. Inheritance / Succession
- Minors cannot directly inherit property; a guardian is appointed
- Age determines when a person can independently administer an estate
7. Insurance and Pensions
- Pensions commence at a fixed retirement age (typically 60–65 years)
- Life insurance premiums are age-dependent; fraudulent age declaration is a legal issue
- Workmen's compensation and disability assessment
8. War / Military Service
- Minimum recruitment age = 18 years
- Age influences service eligibility and pension entitlement
9. Adoption
- Age of adoptee must be certified; generally below 18 years for legal adoption (CARA guidelines)
10. Identification of Unknown Bodies
- In unidentified decomposed bodies or skeletal remains, age estimation helps narrow identity and assists in disaster victim identification (DVI)
Summary Table: Methods at a Glance
| Method | Best Age Group | Reliability |
|---|---|---|
| Physical/secondary sexual chars | 8–20 years | Moderate |
| Dental eruption | 0–25 years | High |
| Gustafson's dental | 25–70 years | High (±3.6 yr) |
| Ossification centres (X-ray) | 0–20 years | Very High |
| Epiphyseal fusion | 14–25 years | Very High |
| Medial clavicle fusion | 18–25 years | Critical for legal majority |
| Skull suture fusion | 22–70+ years | Moderate |
| Pubic symphysis | 18–70+ years | Moderate–High |
| Aspartic acid racemisation | Any | Very High (lab) |
| DNA methylation | Any | Very High (lab) |
Important Legal Maxims
- If age falls in a borderline zone, the benefit of doubt goes to the accused/subject (Doli incapax principle; also in POCSO cases — courts give benefit of doubt in favour of juvenility)
- The medical officer gives an opinion, not a verdict; the court decides the legal age
- In cases of discrepancy between documents and medical evidence, courts weigh both but increasingly defer to radiological/ossification evidence
Sources: Gray's Anatomy for Students (Skeletal age determination); FMT knowledge base — Parikh's Textbook of Medical Jurisprudence, Forensic Medicine & Toxicology; IPC Sections 82–83; POCSO Act 2012; Prohibition of Child Marriage Act 2006
This is a shared conversation. Sign in to Orris to start your own chat.