Mobitz 1
Reading File
Finding Sources
Searching PubMed
"Mobitz type I" OR "Wenckebach" AND "AV block"
Reading File
Reading File
Loading Image
Reading File
Here is a complete summary of Mobitz Type I (Wenckebach) Second-Degree AV Block:
Mobitz Type I (Wenckebach) - Second-Degree AV Block
Definition
Second-degree AV block is characterized by both conducted beats (P wave followed by a QRS) and non-conducted (dropped) beats (P wave not followed by a QRS). In Mobitz I specifically, the non-conducted beats are preceded by progressively lengthening PR intervals on the ECG. After the dropped beat, the PR interval resets to its baseline - shorter than the last conducted PR interval. This cycle then repeats.
ECG Features
| Feature | Finding |
|---|---|
| PR interval | Progressively lengthens with each beat |
| Dropped beat | P wave occurs without a following QRS |
| After the drop | PR interval resets to baseline (shorter) |
| Rhythm pattern | "Grouped beating" |
| QRS complex | Usually narrow (block is at the AV node) |
| Conduction ratio | Described as X:Y (e.g., 4:3 means 4 P waves, 3 QRS complexes) |
ECG example (Mobitz I):
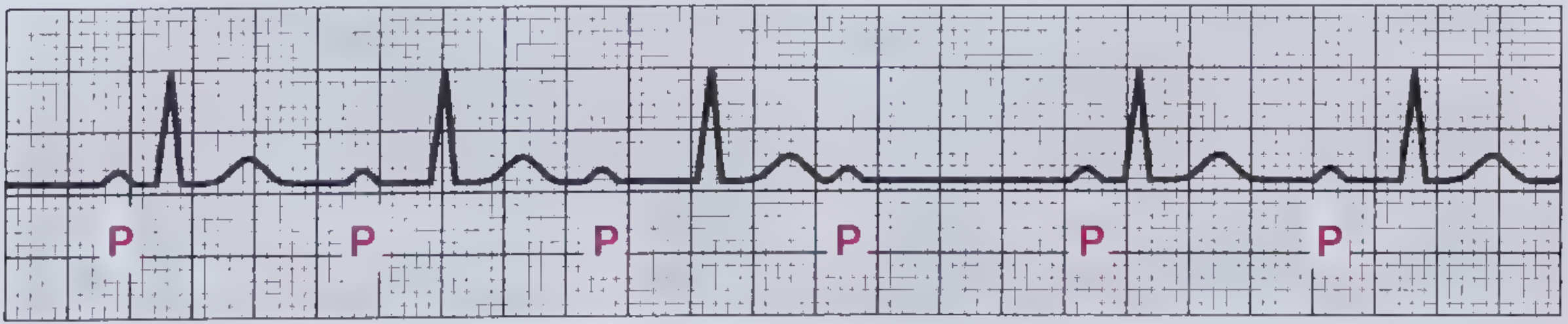
P-wave rate is constant, PR interval progressively lengthens until a QRS is completely blocked (after the 4th P wave), then the cycle resets.
Mechanism
Each successive depolarization prolongs the refractory period of the AV node. The next atrial impulse arrives earlier in the relative refractory period and conducts more slowly. This progressively worsens until an atrial impulse arrives during the absolute refractory period and is blocked entirely. The pause allows the AV node to recover, and the cycle repeats.
- Block location: AV node (nodal, suprahisian)
Causes
| Category | Examples |
|---|---|
| Ischemia | Inferior MI (RCA supplies the AV node in most patients); look for ST elevation in II, III, aVF |
| Medications | Beta-blockers, calcium channel blockers, digoxin toxicity |
| Increased vagal tone | Athletes, vasovagal episodes |
| Inflammation | Myocarditis, cardiac surgery |
| Normal variant | Can occur in structurally normal hearts |
Symptoms
Generally asymptomatic. Symptoms such as dyspnea, palpitations, and lightheadedness are rare.
Prognosis
Generally good prognosis. Progression to higher-degree AV block is uncommon. An infranodal location of block (atypical for Mobitz I) may carry a higher risk.
Treatment
- Usually no treatment needed in asymptomatic, hemodynamically stable patients.
- Address reversible causes (stop offending medications, treat ischemia/myocarditis).
- If symptomatic or hemodynamically unstable: atropine (first-line pharmacologic agent) or temporary cardiac pacing.
- Permanent pacemaker may be necessary in rare cases of symptomatic, refractory Mobitz I.
Comparison with Mobitz Type II (Key Distinction)
| Feature | Mobitz I (Wenckebach) | Mobitz II |
|---|---|---|
| PR interval | Progressively lengthens | Fixed/constant before the drop |
| QRS width | Narrow (usually) | Wide (often, due to infranodal block) |
| Block location | AV node | Below the AV node (His-Purkinje) |
| Prognosis | Benign | More serious; risk of complete heart block |
| Pacemaker need | Rarely | More commonly indicated |
Sources: Frameworks for Internal Medicine, p. 48; Tintinalli's Emergency Medicine (Table 18-18, p. 1860)
This is a shared conversation. Sign in to Orris to start your own chat.