For example, I am working in the emergency department and a patient comes with hypernatremia. How do I diagnose that it is hypernatremia and I-- how am I efficient enough to just see by the look that it is going to be hypernatremia and how to treat it?
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have everything I need from the top emergency medicine textbooks. Let me compose a thorough, clinically practical answer.
Hypernatremia in the Emergency Department
Definition: Serum sodium > 145 mEq/L (with serum osmolality > 295 mOsm/kg).
1. How to Spot It at the Bedside - "See It at a Glance"
Before any lab result comes back, certain patient profiles and bedside findings should immediately raise your index of suspicion:
High-risk patient profile (who to think of first):
- Elderly or debilitated patient who cannot get up to drink
- Infant (especially if formula is improperly mixed)
- Altered/unconscious patient or anyone intubated and sedated
- Diabetic patient with poor control
- Patient with known diabetes insipidus
- Anyone with a history of prolonged vomiting, diarrhea, burns, or high fever
What you see at the bedside:
| Sign | What it tells you |
|---|---|
| Dry mucous membranes, sunken eyes, poor skin turgor | Free water loss (dehydration) |
| Altered mental status, confusion, lethargy | Brain cell shrinkage from hyperosmolality |
| Irritability, high-pitched cry (in infants) | Early neurological effect |
| Ataxia, tremors, hyperreflexia, muscle weakness | CNS and neuromuscular effects |
| Seizures, unresponsiveness | Severe/rapid-onset hypernatremia |
| Polyuria + polydipsia | Points toward diabetes insipidus |
| Edema, hypertension | Hypervolemic type (Na overload, e.g., Cushing's, iatrogenic saline) |
| Moon facies, dorsal fat pad, thin skin | Consider Cushing's syndrome as underlying cause |
| BUN/Cr ratio > 40 | Hyperosmolar dehydration pattern |
The mental status change is the most consistent sign. Any confused, obtunded elderly patient or infant brought to your ED should get a serum sodium checked immediately. - Rosen's Emergency Medicine, Concepts and Clinical Practice
2. The Three Types - Classification by Volume Status
The first thing you do after confirming the number is assess volume status. This drives your entire management approach.
| Type | Total Body Na+ | Total Body Water | Common Causes |
|---|---|---|---|
| Hypovolemic (most common) | Decreased | Decreased more | Diarrhea, vomiting, sweating, burns, GI fistulas, loop diuretics, osmotic diuresis (glucose, mannitol) |
| Normovolemic | Near normal | Decreased | Diabetes insipidus (central or nephrogenic), hypodipsia, drugs (amphotericin, lithium, phenytoin, aminoglycosides) |
| Hypervolemic | Increased | Normal/Increased | Cushing's syndrome, primary hyperaldosteronism, hypertonic saline infusion, NaHCO3 infusion, salt tablet ingestion, poorly diluted enteral feeds |
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide
3. Diagnostic Work-Up
Order these immediately alongside routine chemistry:
- Serum electrolytes + serum osmolality - confirms hypernatremia and hyperosmolar state
- Urine osmolality - the key discriminator:
- Urine osmolality > 800 mOsm/kg = concentrated urine = extrarenal loss (kidneys working normally - vomiting, diarrhea, burns)
- Urine osmolality < 300 mOsm/kg = dilute urine = central DI (kidneys cannot concentrate)
- Urine osmolality 300-800 mOsm/kg = partial DI
- Urine osmolality > 100, urine Na > 20 = renal causes (osmotic diuresis, loop diuretics)
- Urine sodium - helps distinguish renal vs. extrarenal:
- Urine Na < 10 mEq/L = extrarenal hypovolemic (kidneys retaining Na appropriately)
- Urine Na > 20 mEq/L = renal loss or Na overload
- BUN/creatinine ratio - ratio > 40 indicates hyperosmolar dehydration
- Blood glucose - osmotic diuresis from hyperglycemia is a common cause
- Cortisol level if Cushing's is suspected
Calculate free water deficit:
TBW (L) = body weight (kg) × correction factor (0.6 for young male; 0.5 for elderly male or young female; 0.45 for elderly female)Free water deficit (L) = TBW × [(Measured Na - 140) / 140]
Example: Elderly man, 70 kg, Na = 165 mEq/L:
- TBW = 0.6 × 70 = 42 L
- Deficit = 42 × [(165-140)/140] = 7.5 L
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
4. Emergency Treatment - Step by Step
Step 1: Stabilize Hemodynamics First
If the patient is in shock or has significant hypoperfusion, give isotonic (0.9%) normal saline immediately, regardless of sodium level. Do not wait. Volume resuscitation takes priority.
For children: 20 mL/kg NS boluses, reassess after each.
Step 2: Treat the Underlying Cause
- Vomiting → antiemetics
- Fever → antipyretics
- Central DI → desmopressin (DDAVP)
- Nephrogenic DI → remove offending drug (lithium, amphotericin), low-sodium diet, hydrochlorothiazide
- Hyperglycemia → insulin + appropriate fluids
Step 3: Correct the Free Water Deficit - SLOWLY
This is where most errors happen. Overcorrecting too fast causes cerebral edema.
| Situation | Correction rate | Fluid of choice |
|---|---|---|
| Chronic hypernatremia (>48h or unknown duration) | No faster than 0.5 mEq/L/hour or 10-12 mEq/24h | D5W or oral free water over 48-72 hours |
| Mild-moderate (Na 145-160) | Gradual correction over 24-48h | 0.45% NaCl at ~100 mL/h |
| Acute/known onset < 6h, lethal salt load | Can correct rapidly | D5W over 1-2h |
| Severe/refractory or Na > 180 | Consider hemodialysis | - |
Maximum safe correction: no faster than 1 mEq/L/hour and no more than 15 mEq/L in the first 24 hours.
Monitor serum sodium every 1-2 hours initially until stable.
Step 4: Monitor
- Urine output closely (risk of acute tubular necrosis)
- Neurological status (watch for signs of cerebral edema - headache, confusion worsening, seizures)
- Repeat serum sodium frequently
5. Special Warnings
- Severity: Serum Na > 150-160 mEq/L carries ~75% mortality if untreated. Na > 160 mEq/L in children requires immediate attention - risk of permanent neurologic damage.
- Do not over-correct: Brain cells adapt to hypernatremia by accumulating organic osmolytes. Rapid correction causes osmotic swelling and cerebral edema - potentially causing central pontine myelinolysis.
- Acute vs chronic matters: If you do not know when it started, assume chronic and correct slowly.
- Acute lethal salt ingestion (< 6h): Rare exception - can correct fast without harm; consider hemodialysis.
Quick Mental Algorithm at the Bedside
Patient with AMS / dehydration / polyuria / high-risk profile
↓
Check serum Na → > 145? → Hypernatremia confirmed
↓
Assess volume status (exam: skin turgor, JVD, BP, HR, edema)
↓
Hypovolemic? Normovolemic? Hypervolemic?
(dehydrated) (DI likely) (Na overloaded)
↓ ↓ ↓
Uosm > 800 Uosm < 300 Uosm > 100
→ GI/sweat loss → Central DI → Cushing's/
Uosm > 100 Uosm 300-800 → iatrogenic
→ Renal loss → Partial DI
↓
Calculate free water deficit
Step 1: NS if shock
Step 2: Treat cause
Step 3: Correct deficit over 48-72h (0.5 mEq/L/h max)
Sources: Tintinalli's Emergency Medicine: A Comprehensive Study Guide | Rosen's Emergency Medicine: Concepts and Clinical Practice | Roberts and Hedges' Clinical Procedures in Emergency Medicine | Tintinalli's (Pediatric section)
To understand all this, first, basically, I need to know about osmolality and all that basic stuff, I guess. Maybe teach me that.
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
Loading Image
I now have everything needed for a thorough, foundational explanation. Let me build this from the ground up.
The Basics: Body Fluids, Osmolality, and Tonicity
Think of this as the foundation under everything in fluid management. Once you get it, hypernatremia, hyponatremia, and IV fluid choice will all click into place.
1. Where Is the Water in Your Body?
A 70-kg adult male is about 60% water - that is roughly 42 liters of fluid distributed across three compartments:
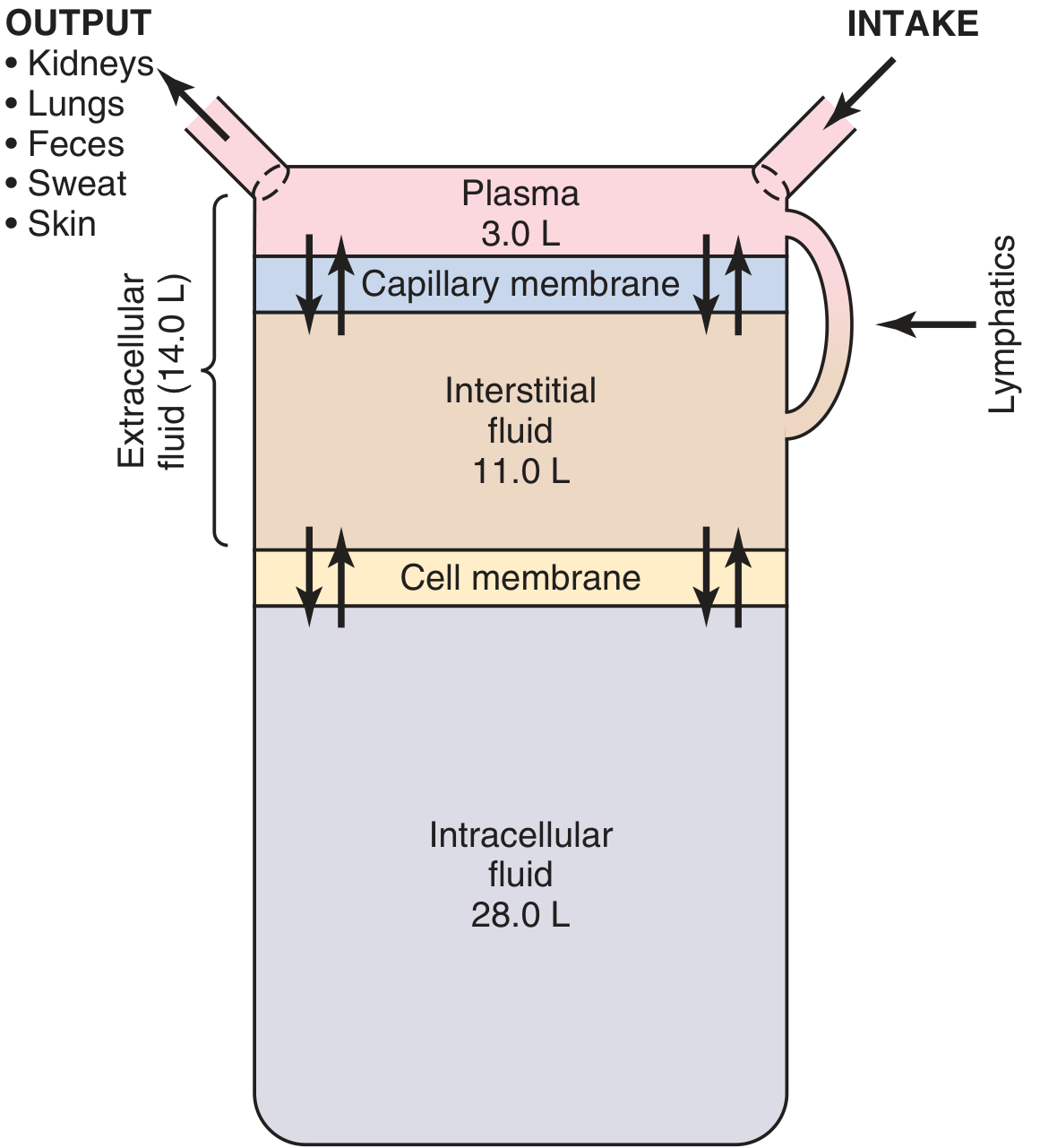
| Compartment | % Body Weight | Volume (70 kg man) |
|---|---|---|
| Intracellular fluid (ICF) | 40% | 28 L (two-thirds of all body water) |
| Interstitial fluid (ECF) | 15% | 10.5 L |
| Plasma (ECF) | 5% | 3.5 L |
| Total | 60% | 42 L |
Two key barriers separate these:
- Cell membrane - separates ICF from ECF (highly selective, water moves freely but ions like Na+ mostly cannot)
- Capillary membrane - separates plasma from interstitial fluid (allows most things through except large proteins)
Women average 50% body water (more fat, less muscle). Newborns are 70-75% water.
- Morgan and Mikhail's Clinical Anesthesiology, 7e
2. What Is Osmolality?
Here is the core concept:
Osmolality = the number of dissolved particles per kilogram of water (mOsm/kg H₂O)
Think of it like this: imagine a cup of water. If you dissolve sugar in it, the water gets "crowded" with particles. The more crowded it is, the higher the osmolality.
- Normal serum osmolality = 275-295 mOsm/kg
- > 295 mOsm/kg = hyperosmolar (too many particles in the blood)
vs. Osmolarity (they sound similar but are slightly different):
- Osmolarity = osmoles per liter of solution (mOsm/L)
- Osmolality = osmoles per kilogram of water (mOsm/kg)
- In clinical practice, these numbers are nearly identical, and the terms are used interchangeably.
- Costanzo Physiology, 7th Edition
3. What Makes Up Serum Osmolality?
You can estimate serum osmolality at the bedside with a simple formula:
Posm (mOsm/L) = 2 × [Na⁺] + Glucose/18 + BUN/2.8
Breaking this down:
- Sodium (×2) - Na⁺ is the dominant extracellular cation; you multiply by 2 to account for its accompanying anion (Cl⁻, HCO₃⁻). This is the biggest contributor.
- Glucose/18 - glucose is normally a minor contributor, but in diabetic patients with high glucose, it matters a lot
- BUN/2.8 - urea contributes to osmolality but not tonicity (explained below)
Example: Patient with Na = 145, Glucose = 90, BUN = 14:
- Estimated Posm = (2 × 145) + 90/18 + 14/2.8
- = 290 + 5 + 5 = 300 mOsm/kg - slightly elevated
- Mulholland and Greenfield's Surgery: Scientific Principles and Practice, 7e
4. Osmolality vs. Tonicity - The Crucial Difference
This trips up a lot of people. They are not the same thing.
| Osmolality | Tonicity | |
|---|---|---|
| Definition | Total dissolved particles per kg water | Effect of a solution on cell volume |
| Includes | All solutes (permeable + impermeable) | Only impermeable solutes |
| Clinically | Lab measurement | Drives water into/out of cells |
The key question for tonicity: Can the solute cross the cell membrane?
- Sodium (Na⁺) - cannot cross freely → affects BOTH osmolality AND tonicity → causes cells to shrink/swell
- Urea (BUN) - crosses cell membranes freely → contributes to osmolality but NOT tonicity → does NOT shift water between compartments
- Glucose - normally impermeable (needs insulin/transporters) → affects both → but with insulin it becomes permeable
Why this matters clinically:
- A patient with a very high BUN (renal failure) may have high osmolality but NOT hypertonicity - their cells are fine
- A patient with high Na⁺ has both high osmolality AND high tonicity - water is being pulled OUT of cells, which is what causes all the brain symptoms in hypernatremia
- Morgan and Mikhail's Clinical Anesthesiology, 7e; Mulholland and Greenfield's Surgery
5. Osmosis - Why Water Moves
Osmosis = water moves across a semipermeable membrane from the side with fewer particles to the side with more particles (from low concentration to high concentration of solutes).
Water always chases solute. It moves to dilute the more concentrated side.
The pressure that would be needed to stop that movement = osmotic pressure.
One practical number: a difference of just 1 mOsm/L between two solutions creates an osmotic pressure of 19.3 mmHg. That is a powerful driving force.
- Morgan and Mikhail's Clinical Anesthesiology, 7e; Costanzo Physiology
6. Isotonic, Hypotonic, Hypertonic - What They Do to Cells
This Guyton & Hall diagram shows it perfectly:
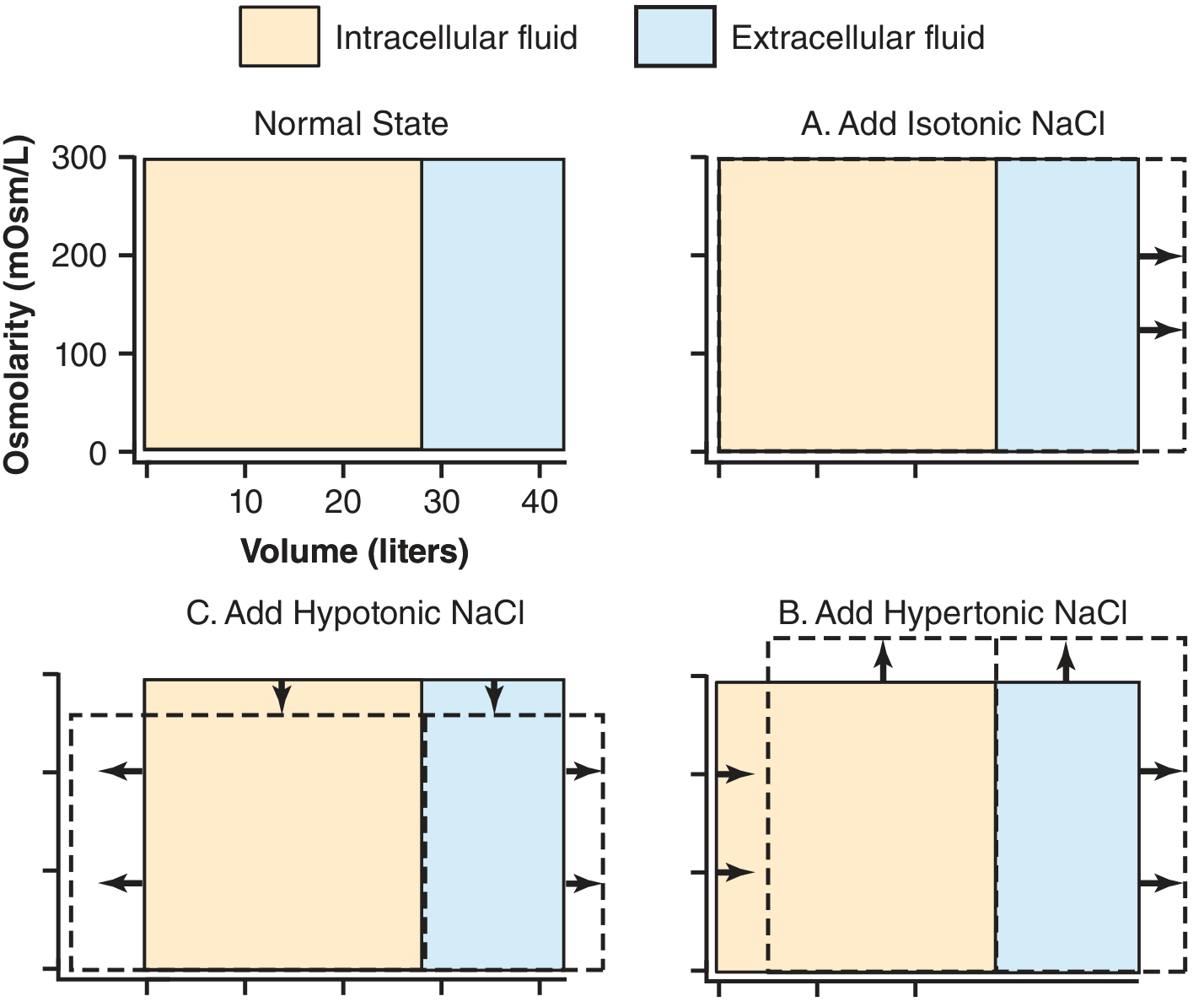
| Solution | Osmolality vs. plasma | What happens to cells | Example |
|---|---|---|---|
| Isotonic | Equal (~290 mOsm/kg) | No change in cell volume | Normal saline (0.9%), Ringer's lactate |
| Hypotonic | Lower than plasma | Water moves INTO cells → cells swell | 0.45% saline, D5W (acts hypotonic once glucose metabolized) |
| Hypertonic | Higher than plasma | Water moves OUT of cells → cells shrink | 3% saline, hypertonic glucose |
7. Now Connect It Back to Hypernatremia
With this foundation, hypernatremia makes perfect sense:
High Na⁺ in the blood = high osmolality = high tonicity
Water is pulled out of every cell in the body, including brain cells. The brain shrinks. That is why you get:
- Confusion, restlessness (mild)
- Lethargy, stupor (moderate)
- Seizures, coma, intracranial hemorrhage (severe/rapid)
The body's normal defense: osmoreceptors in the hypothalamus detect this, trigger thirst (drink water) and release ADH/vasopressin (kidneys keep water). When either of these fails - or the patient cannot drink - sodium climbs.
Why you correct slowly: Brain cells adapt to being shrunk by accumulating organic osmolytes (taurine, sorbitol, etc.) over 48-72 hours. If you now flood the body with free water too fast, the outside becomes suddenly hypotonic but the inside is still loaded with those osmolytes - water rushes into brain cells, causing cerebral edema. This is why the max correction rate is 0.5 mEq/L/hour.
Summary in One Mental Map
Body water → 3 compartments (ICF 28L | Interstitial 10.5L | Plasma 3.5L)
↓
Osmolality = particle concentration in plasma (normal 275-295 mOsm/kg)
↓
Estimated by: 2×Na + Glucose/18 + BUN/2.8
↓
Tonicity = only the impermeable particles (mainly Na⁺)
↓
High tonicity → water leaves cells → cells shrink
Low tonicity → water enters cells → cells swell
↓
Hypernatremia = ↑ Na⁺ = ↑ tonicity = brain cells shrink = neurological symptoms
Sources: Guyton and Hall Textbook of Medical Physiology | Costanzo Physiology 7e | Morgan and Mikhail's Clinical Anesthesiology 7e | Mulholland and Greenfield's Surgery 7e
This is a shared conversation. Sign in to Orris to start your own chat.