I now have everything needed for a thorough, well-illustrated answer. Here it is:
Portal Vein & Portocaval Anastomosis - Complete Clinical Guide
PART 1: Portal Vein - The Basics
What is it?
The portal vein is the main highway that carries nutrient-rich, deoxygenated blood from the gut to the liver for processing. Think of it as the liver's "food delivery pipe."
| Feature | Detail |
|---|
| Length | ~8 cm |
| Formation level | L2 vertebra (behind neck of pancreas) |
| Formed by | Superior Mesenteric Vein (SMV) + Splenic Vein |
| Position | Anterior to IVC, posterior to neck of pancreas |
| Tributaries | Left gastric, right gastric, cystic, paraumbilical veins |
| Drains into | Right and left branches → liver sinusoids → hepatic veins → IVC |
Blood Flow Path (Normal):
Gut / Spleen
↓
Portal Vein (SMV + Splenic v.)
↓
Liver (processes nutrients, drugs, toxins)
↓
Hepatic Veins → IVC → Heart
PART 2: What is Portocaval Anastomosis?
A portocaval (portosystemic) anastomosis is a natural connection point where portal veins and systemic (caval) veins communicate. In normal health, these connections are tiny and carry almost no blood. But when portal pressure rises (portal hypertension), these routes open up as "escape valves."
Easy analogy: Imagine a river (portal vein) blocked by a dam (liver disease). The water backs up and floods through side canals (anastomoses) into the main sea (systemic circulation).
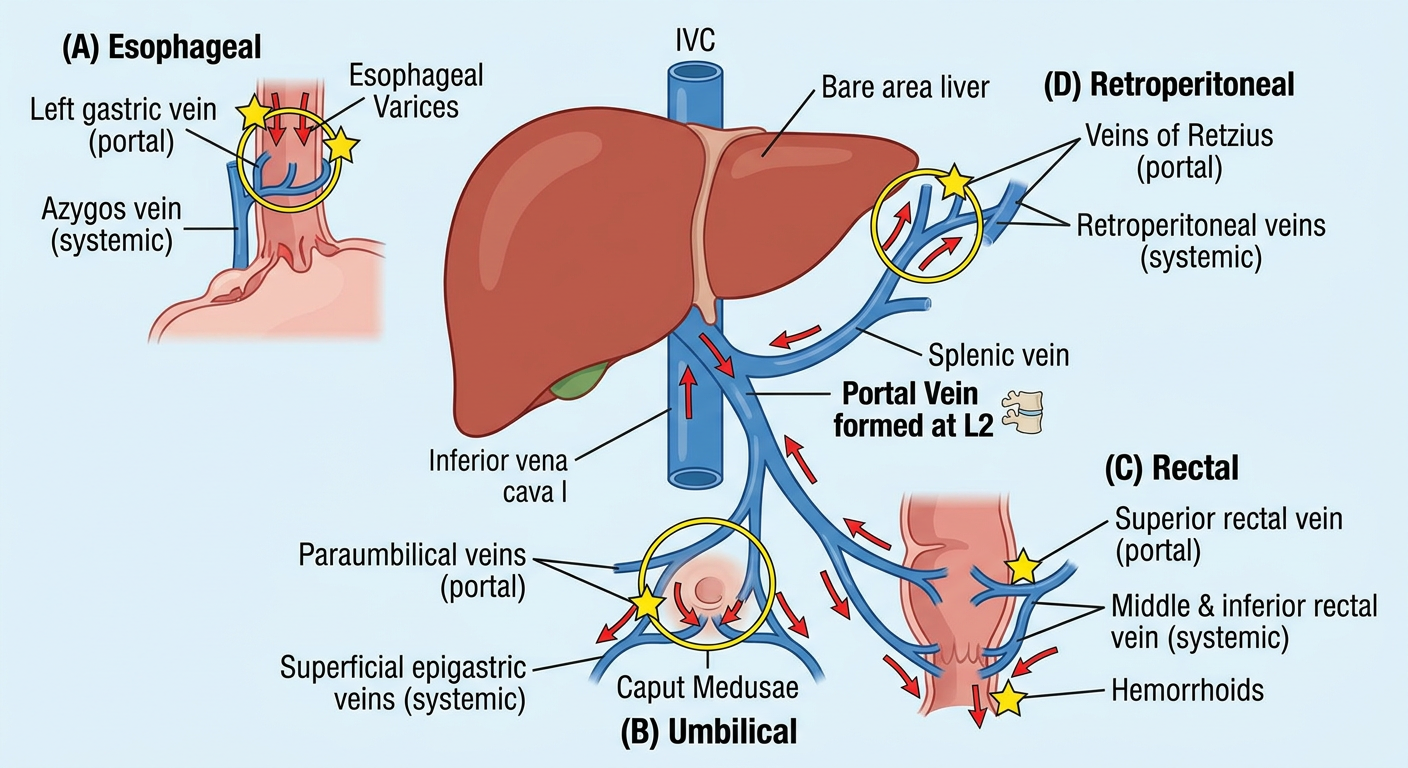
PART 3: The 4 Major Portocaval Anastomosis Sites
Here is the generated overview diagram:
Site 1 - Esophageal (Lower Esophagus)
| |
|---|
| Portal side | Left gastric vein (coronary vein) → esophageal branches |
| Systemic side | Esophageal tributaries of azygos vein |
| Location | Lower 1/3 of esophagus, submucosal plexus |
| Clinical consequence | Esophageal varices - most dangerous! Can rupture and cause massive, life-threatening haemorrhage |
Clinical tip: This is why patients with cirrhosis often present with haematemesis (vomiting blood). Esophageal varices bleed from the submucosal plexus right where the two circulations meet.
Site 2 - Paraumbilical / Anterior Abdominal Wall
| |
|---|
| Portal side | Paraumbilical veins (travel in the round ligament of liver with the obliterated umbilical vein) |
| Systemic side | Superficial and inferior epigastric veins → thoracoepigastric veins |
| Location | Umbilicus and anterior abdominal wall |
| Clinical consequence | Caput medusae ("head of Medusa") - dilated, tortuous veins radiating from the umbilicus |
Clinical tip: Caput medusae specifically indicates congestion of the left hepatic lobe because the paraumbilical veins drain into the left branch of the portal vein - not the main trunk. This is unlike other anastomoses.
- Color Atlas of Human Anatomy, Vol 1, p. 557-558
Site 3 - Anorectal (Rectum)
| |
|---|
| Portal side | Superior rectal vein (branch of inferior mesenteric vein) |
| Systemic side | Middle rectal vein (internal iliac) + Inferior rectal vein (pudendal) |
| Location | Upper rectum / anorectal junction |
| Clinical consequence | Anorectal varices / Hemorrhoids - painful bleeding per rectum |
Clinical tip: Portal hypertension can cause large, symptomatic internal hemorrhoids. However, not all hemorrhoids are from portal hypertension - common hemorrhoids are very different!
Site 4 - Retroperitoneal (Bare Area / Veins of Retzius)
| |
|---|
| Portal side | Intraparenchymal branches of right portal vein; colonic/omental veins |
| Systemic side | Retroperitoneal veins draining into azygos, hemiazygos, lumbar, renal veins |
| Location | Bare area of liver, posterior abdominal wall |
| Clinical consequence | Usually no dramatic clinical sign, but contributes to overall portal decompression |
PART 4: Summary Table
| Site | Portal Vein | Systemic Vein | Clinical Sign |
|---|
| Lower esophagus | Left gastric v. | Azygos v. | Esophageal varices ⭐ |
| Umbilicus | Paraumbilical v. | Superficial epigastric v. | Caput medusae |
| Rectum | Superior rectal v. | Middle + inferior rectal v. | Anorectal varices / hemorrhoids |
| Retroperitoneal | Right portal branches, colonic v. | Retroperitoneal/lumbar/renal v. | Usually silent |
PART 5: Portal Hypertension - The Clinical Trigger
Normal portal pressure: 5-10 mmHg
Portal hypertension: >12 mmHg (or gradient >5 mmHg above IVC)
Causes:
- Pre-hepatic: Portal vein thrombosis, splenic vein thrombosis
- Intrahepatic: Cirrhosis (most common), schistosomiasis, alcoholic liver disease
- Post-hepatic: Budd-Chiari syndrome, right heart failure
Why do anastomoses open?
When pressure backs up in the portal system, blood is forced through the tiny pre-existing anastomotic channels. These channels dilate under pressure, forming varices (varicosities). The problem: variceal walls are thin and fragile, so they bleed easily and massively.
PART 6: Surgical Portocaval Anastomosis (Treatment)
When varices keep bleeding despite medical management, surgeons can create an artificial portocaval shunt to deliberately redirect portal blood into the systemic circulation and reduce portal pressure.
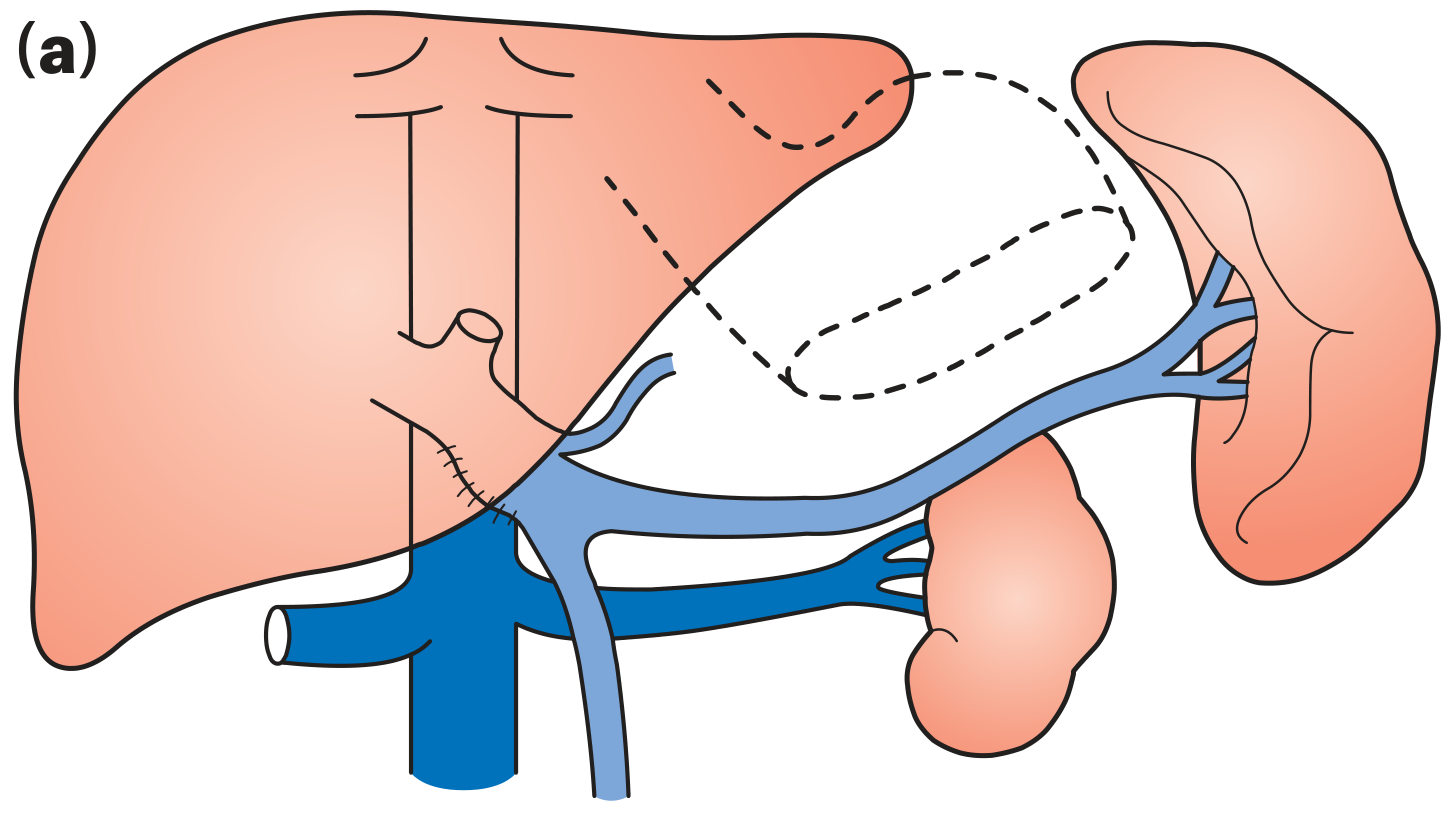
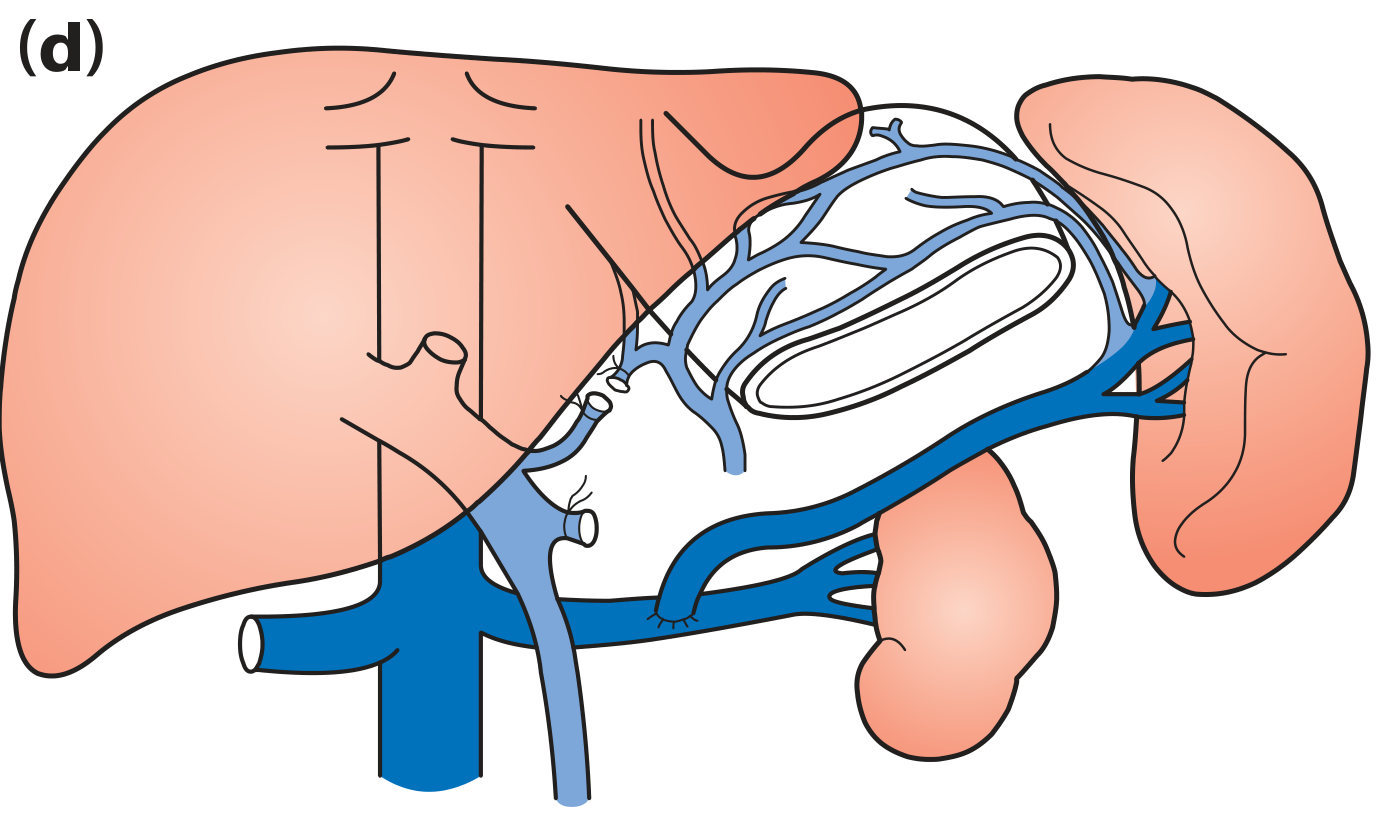
Surgical shunt types (from Bailey & Love's Surgery):
(a) Side-to-side portocaval anastomosis - portal vein joined side-to-side to IVC
(d) Splenorenal (selective) shunt - splenic vein joined to left renal vein (preserves hepatoportal flow better)
| Shunt Type | Description | Advantage |
|---|
| Side-to-side portocaval | Portal v. joined to IVC side-by-side | Complete portal decompression |
| End-to-side portocaval | Portal v. divided and end joined to IVC | Complete decompression |
| Mesocaval H-graft | SMV joined to IVC via interposition graft | Less hepatic dissection |
| Splenorenal (Warren shunt) | Splenic v. to renal v. | Selective - preserves liver perfusion; lower encephalopathy |
Key complication of shunts: Hepatic encephalopathy - because ammonia and other gut toxins now bypass liver detoxification and reach the brain directly.
- Bailey and Love's Short Practice of Surgery, 28th Ed, p. 1227
PART 7: Quick Memory Trick (Mnemonic)
"PURE" for portal hypertension consequences:
- P - Portal hypertension itself
- U - Umbilical veins dilate → caput medusae
- R - Rectal varices / hemorrhoids
- E - Esophageal varices (most dangerous)
Or remember the 4 sites as: "Every Rectum Under Bare skin"
- Esophagus
- Rectum
- Umbilicus
- Bare area (retroperitoneal)
Video Resources
Sources: Color Atlas of Human Anatomy Vol.1 (p. 557-558) | Bailey & Love's Surgery 28th Ed (p. 1227) |
Kenhub - Portosystemic Anastomosis |
Wikipedia - Portacaval Anastomosis