Wrist arthrodesis procedure and implants required in detail
Reading File
Finding Sources
Finding Sources
Searching the Web
wrist arthrodesis surgical procedure implants technique detail
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed for a thorough, well-illustrated answer. Here is the complete reference:
Wrist Arthrodesis - Procedure and Implants
Source: Campbell's Operative Orthopaedics, 15th Ed. 2026; Miller's Review of Orthopaedics, 9th Ed.
Definition and Overview
Wrist arthrodesis (wrist fusion) is the surgical elimination of motion at the radiocarpal and, in most cases, the intercarpal and carpometacarpal joints by fusing the distal radius to the carpal bones and the base of the metacarpals. It is considered a salvage procedure but reliably delivers a stable, painless wrist at the cost of motion.
Indications
| Category | Specific Conditions |
|---|---|
| Post-traumatic | Malunited/ununited scaphoid with radiocarpal arthritis; severely comminuted distal radius fractures |
| Inflammatory | Rheumatoid arthritis (end-stage); psoriatic arthritis |
| Degenerative | Advanced primary or secondary osteoarthritis of the radiocarpal and midcarpal joints |
| Neuromuscular | Volkmann ischemic paralysis; poliomyelitis; spastic cerebral palsy |
| Infectious | Tuberculosis of the wrist |
| Salvage | Failed wrist implant arthroplasty; failed proximal row carpectomy |
| Kienbock's disease | Advanced avascular necrosis of the lunate |
Total wrist arthrodesis is the treatment of choice in young patients with strenuous physical demands who have advanced arthritic changes in both the radiocarpal and midcarpal joints of the dominant hand.
Position of Fusion
The position of the wrist determines function - this is one of the most important decisions:
- Standard position: 10-20° of extension (dorsiflexion), with the long axis of the third metacarpal shaft aligned with the long axis of the radial shaft. This is the position naturally assumed when the fist is strongly clenched - it maximizes grasping strength.
- In rheumatoid arthritis: neutral or a mild flexed position is often preferred to counterbalance zigzag collapse and ulnar drift; 5-10° of ulnar deviation is preferred.
- In bilateral fusions: one wrist may be placed in extension and the other in slight flexion to preserve personal hygiene function. Both wrists should never be fused in extension simultaneously.
- In cerebral palsy/neuromuscular conditions: neutral flexion with ulnar deviation, or mild flexion, is well tolerated.
Types of Wrist Arthrodesis
1. Total Wrist Arthrodesis (TWA)
Fusion of the radiocarpal joint + intercarpal joints + 2nd and 3rd carpometacarpal (CMC) joints. Haddad and Riordan recommended including the 2nd and 3rd CMC joints to prevent subsequent painful motion in them, as disease often extends into these joints.
2. Partial (Limited) Wrist Arthrodesis
Selected joint fusions that preserve some wrist motion:
| Type | Joints Fused | Indication |
|---|---|---|
| Radioscapholunate | Radius + scaphoid + lunate | Radiocarpal arthritis with intact midcarpal joints |
| Radiolunate | Radius + lunate | Die-punch lunate fossa fractures; RA ulnar translation |
| Four-corner fusion | Capitate + lunate + hamate + triquetrum (+ scaphoid excision) | SLAC/SNAC wrist |
| Scaphotrapeziotrapezoidal (triscaphe) | Scaphoid + trapezium + trapezoid | Rotary subluxation of scaphoid; STT arthritis |
| Scaphocapitate | Scaphoid + capitate | |
| Capitolunate | Capitate + lunate | Three-corner fusion with scaphoid and triquetrum excision |
Surgical Techniques
Technique A - Haddad and Riordan (Classic Total Wrist Arthrodesis with Iliac Crest Graft)
Approach:
- J-shaped incision starting 2.5-3.8 cm proximal to the radial styloid on the midlateral forearm, extending distally across the styloid, then curving dorsally to end at the base of the 2nd metacarpal.
- Mobilize and retract the superficial branch of the radial nerve. Incise the dorsal carpal ligament in the interval between the 1st and 2nd dorsal compartments, leaving it attached volarly.
- Mobilize subperiosteally and retract the abductor pollicis longus (APL), extensor pollicis brevis (EPB), and finger/wrist extensors.
- Divide the extensor carpi radialis longus (ECRL) tendon just proximal to its insertion on the 2nd metacarpal base, leaving a stump for later repair.
- Remove the capsule from the radiocarpal, intercarpal, and 2nd CMC joints.
- Locate and ligate/divide the dorsal branch of the radial artery (dorsal carpal arch branch).
Bone preparation:
7. Denude the radiocarpal joint of articular cartilage and subchondral bone.
8. Harvest a graft ~3.8 cm × 2.5 cm from the inner table of the iliac crest using an oscillating saw and osteotomes.
9. With the wrist in 15° of dorsiflexion, cut a slot using an oscillating saw through the distal radius, carpal bones, and bases of the 2nd and 3rd metacarpals (do not penetrate the medial radius cortex or enter the DRUJ). Place the graft in the prepared slot.
Fixation:
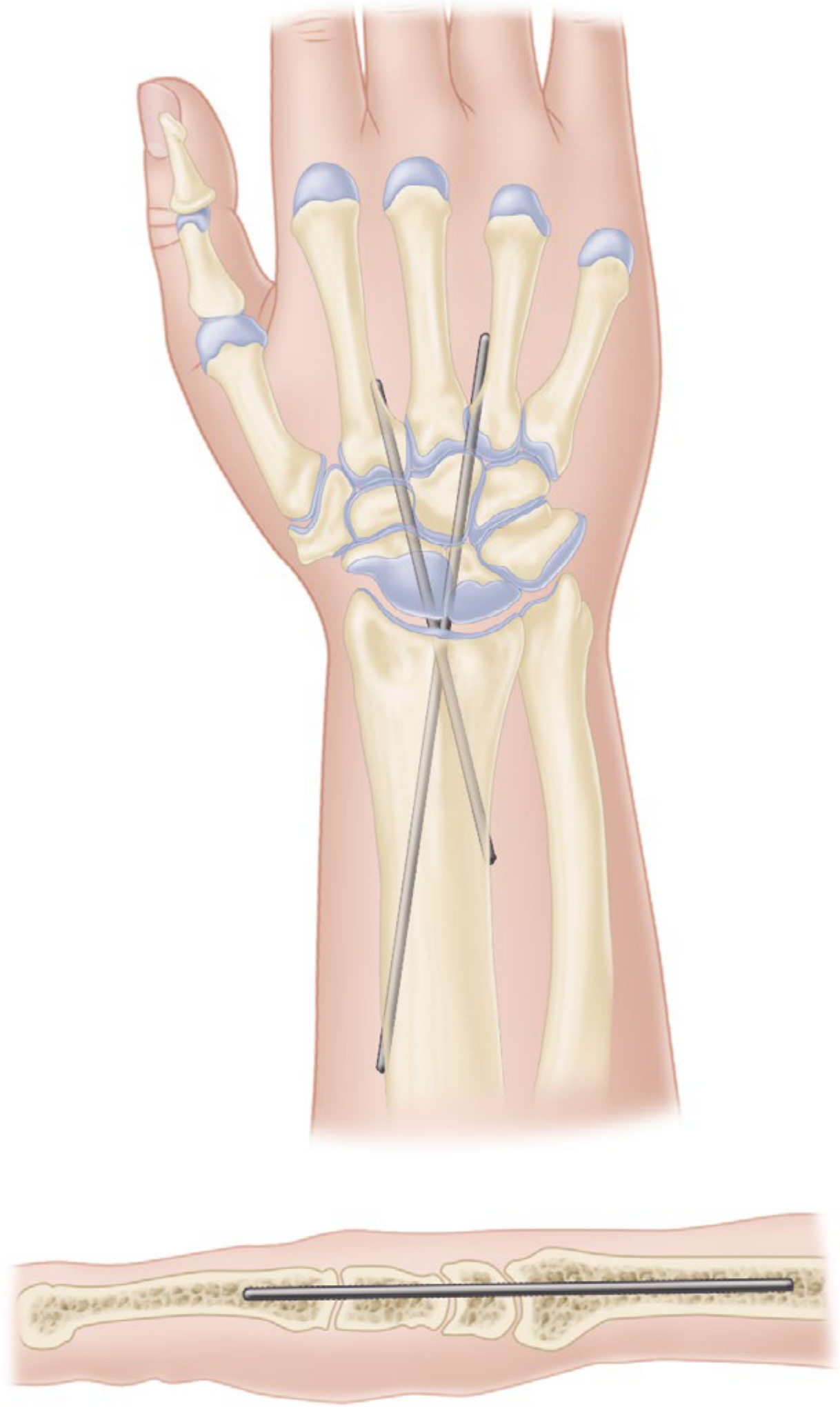
10. If unstable, insert a smooth Kirschner wire obliquely or longitudinally engaging the base of the 2nd metacarpal and distal radius; cut off under the skin at the palm (remove at 6-8 weeks).
11. Close the dorsal carpal ligament deep to the APL and EPB.
12. Suture the ECRL tendon; close the wound.
13. Apply a sugar-tong splint.
Technique B - Millender and Nalebuff (for Rheumatoid Arthritis)
- Dorsal straight longitudinal incision; protect the wrist and finger extensor tendons.
- Curette away remaining cartilage; remove sclerotic bone from carpus and radius down to cancellous bone. Varying amounts of bone may need to be resected to reduce a dislocated wrist.
- Drill a Steinmann pin of appropriate size into the carpus and out distally between the 2nd and 3rd metacarpals; then drill proximally into the medullary canal of the radius and cut off its end beneath the skin.
- Alternative: resect the 3rd metacarpal base and insert pins down the 2nd and 3rd metacarpals - this is used when simultaneous MCP joint arthroplasties are planned.
Technique C - For Cerebral Palsy / Neuromuscular Conditions (Technique 77.7)
- After lengthening or releasing the flexor tendons as necessary, make a dorsal longitudinal incision.
- Excise the proximal carpal row (if needed for correction). Denude all remaining cartilage from the radiocarpal, intercarpal joints, and 2nd/3rd CMC joints.
- Use corticocancellous portions of the excised carpal bones or iliac crest grafts.
- Transfix with two Steinmann pins (7/64 to 9/64 inch) or a 3.5 mm dorsal plate.
- Apply a long arm cast with the elbow at 90°, forearm in neutral rotation.
Implants Required
1. Dedicated Wrist Fusion Plates (Most Common in Modern Practice)
AO/Synthes Wrist Fusion Plate (most widely used):
- Placed on the dorsal surface of the wrist
- Extends from the distal radius to the base of the 3rd metacarpal
- Pre-contoured with a dorsal bend/angulation of ~15° to match the dorsal wrist contour and achieve the functional fusion position
- Can be bent further intraoperatively; avoid bending at hole level or multiple opposing bends (weakens the plate)
- Material: stainless steel or titanium alloy
- Fixed to the bone with cortical/locking screws: typically 3-4 screws into the distal radius + 2 screws into the metacarpal + at least 1 screw into the capitate if possible
Other named plates used in clinical practice:
- LCP Wrist Fusion Plate (Synthes) - locking compression plate variant
- VariAx 2 (Stryker) - titanium alloy, low-profile locking
- Circular plate (for four-corner arthrodesis) - high fusion rates reported (Bedford and Yang, 2010)
- 3.5 mm reconstruction plate - used in some centres; technique involves placing the extensor retinaculum beneath the extensor tendons, with 3-4 screws in the distal radius and 2 screws in the metacarpal
Important surgical note: The dorsal prominences of the distal radius, lunate, capitate, and proximal 3rd metacarpal often must be resected to allow the plate to lie flat against the carpal bones. Failure to do this causes distraction of the carpal bones when the plate is applied.
The plate remains in the body permanently and is not removed unless causing problems.
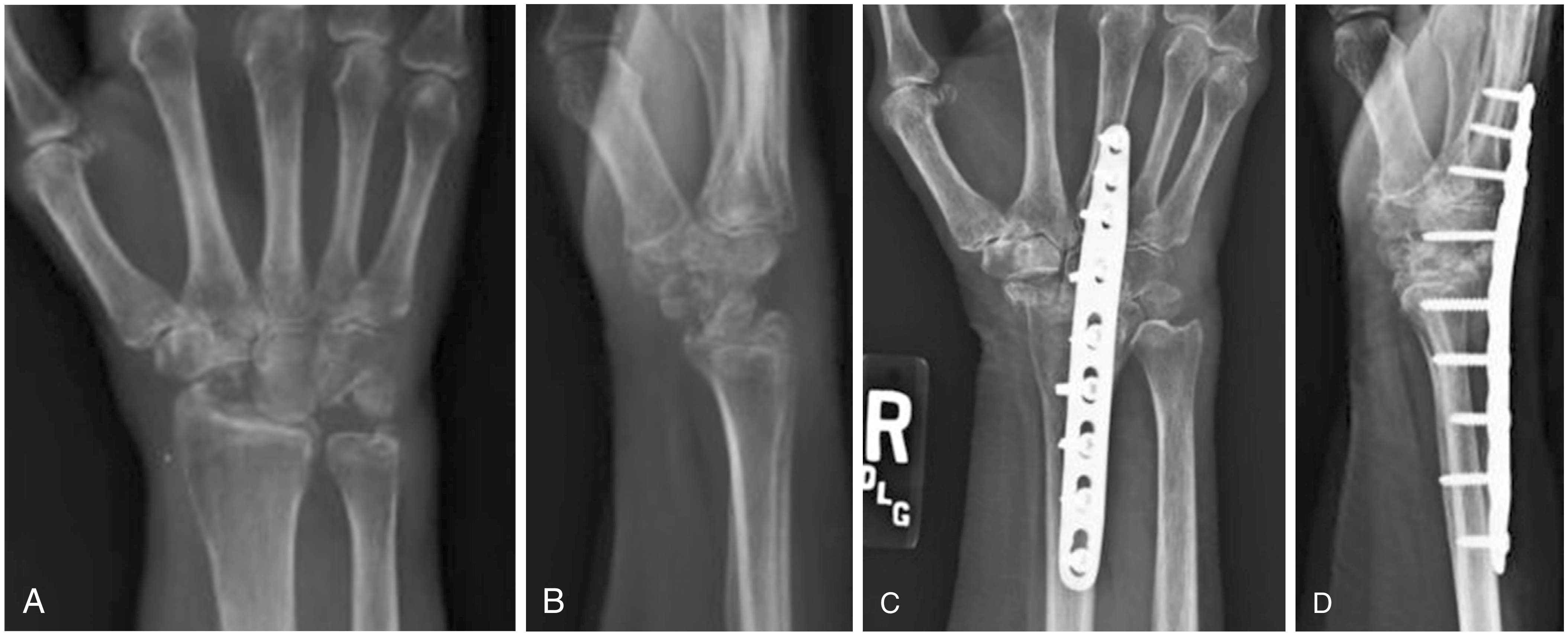
Total wrist arthrodesis with Synthes wrist fusion plate in a 65-year-old woman after failed proximal row carpectomy - Campbell's Operative Orthopaedics, 15th Ed.
2. Kirschner Wires (K-wires)
- Used as supplementary fixation to prevent rotation when a bone graft is the primary construct
- Inserted obliquely or longitudinally, engaging the base of the 2nd metacarpal through the carpus into the distal radius
- Cut off beneath the skin at the palm
- Typically removed at 6-8 weeks
- Also used in paediatric cases where plates are not appropriate
3. Steinmann Pins (Intramedullary)
- Sizes: 7/64 to 9/64 inch (approximately 2.8-3.6 mm); or 3.2-3.5 mm
- Inserted from between the 2nd and 3rd metacarpal shafts, through the carpus, and proximally into the medullary canal of the radius
- A supplementary staple or oblique pin is added to prevent rotation
- Used especially when simultaneous MCP arthroplasties are planned (K-wires allow operations at the finger level without plate obstruction)
- One or two pins depending on technique
4. Bone Graft
An integral part of almost all wrist fusion techniques:
| Graft Source | Description | Usage |
|---|---|---|
| Iliac crest (autograft) | Corticocancellous; ~3.8 × 2.5 cm block | Haddad-Riordan technique; large defects |
| Distal radius (local autograft) | Cancellous bone from the resected distal radial prominence | Harvested during joint preparation |
| Proximal row carpus | Corticocancellous from excised scaphoid, lunate, triquetrum | In cases with proximal row carpectomy |
| Allograft | Cancellous chips | Supplementary fill |
The graft bridges from the radius to the proximal carpal bones; in total arthrodesis it extends distally to the 3rd metacarpal base. It replaces lost cartilage and promotes bony union.
5. Supplementary Fixation
- Staples: Used with Steinmann pin fixation to prevent rotational instability
- Interosseous wires: Used in limited/partial fusions
- Lag screws: Used in subtotal arthrodesis (e.g., radioscapholunate); 3.5 mm or 4.0 mm cancellous screws
- Headless compression screws (e.g., Herbert screws): Used in limited carpal fusions (four-corner, scaphoid-capitate)
DRUJ Management
- Because of discrepancy in length between the radius and ulna, or because of traumatic arthritis in the DRUJ, the distal ulna is usually resected (Darrach procedure) at the time of total wrist arthrodesis.
- This prevents DRUJ impingement after fusion.
Postoperative Care
| Phase | Management |
|---|---|
| 0-2 weeks | Bulky dressing or sugar-tong/volar plaster splint; avoid cast due to swelling |
| 2-6 weeks | Short or long arm cast depending on technique |
| 6-8 weeks | K-wires/Steinmann pins removed (if used); transition to removable splint |
| 10-12 weeks | Bony union expected on radiograph; plate and screws are left permanently |
| Ongoing | Activity restriction based on patient demands; intrinsic tightness of index and long fingers is a recognized complication and should be monitored |
Complications
- Non-union (most common with pin fixation; lower rates with plate fixation)
- Implant failure / plate irritation (extensor tendon attrition over dorsal plate)
- Painful DRUJ (if not addressed at index procedure)
- Intrinsic muscle tightness of the index and middle finger (occult compartment syndrome-related)
- Pisotriquetral dysfunction following limited or total wrist arthrodesis
- Radial physeal arrest in patients under 17 years if physis is violated (epiphyseal-sparing technique recommended for patients under 12)
- Persistent pain from unfused or newly arthritic adjacent joints (CMC joints if not included in fusion)
Summary: Implant Selection Guide
| Clinical Scenario | Preferred Implant |
|---|---|
| Standard total wrist arthrodesis | AO/Synthes wrist fusion plate + bone graft |
| RA with planned MCP arthroplasty | Steinmann intramedullary pin(s) + supplementary staple |
| Neuromuscular (CP, polio) | Steinmann pins or 3.5 mm dorsal plate |
| Limited/partial arthrodesis (four-corner, STT) | Headless compression screws, circular plate, or K-wires |
| Paediatric | K-wires (physeal-sparing); avoid plates until skeletal maturity |
| Poor bone quality / salvage | Plate + supplementary bone graft from iliac crest |
- Campbell's Operative Orthopaedics 15th Ed. 2026, Techniques 74.40, 77.7, 78.36; Miller's Review of Orthopaedics 9th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.