Pneumonia vs collapse lung xray
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
pneumonia vs lung collapse atelectasis chest xray differences radiology findings
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Loading Image
Reading File
I now have comprehensive information to give a detailed, well-sourced answer. Let me compile it.
Pneumonia vs. Lung Collapse (Atelectasis) on Chest X-ray
Both produce opacification (whiteness) on CXR, but they differ fundamentally in mechanism - pneumonia fills alveoli with exudate, while collapse (atelectasis) results in loss of lung volume. Telling them apart is one of the most common radiological challenges.
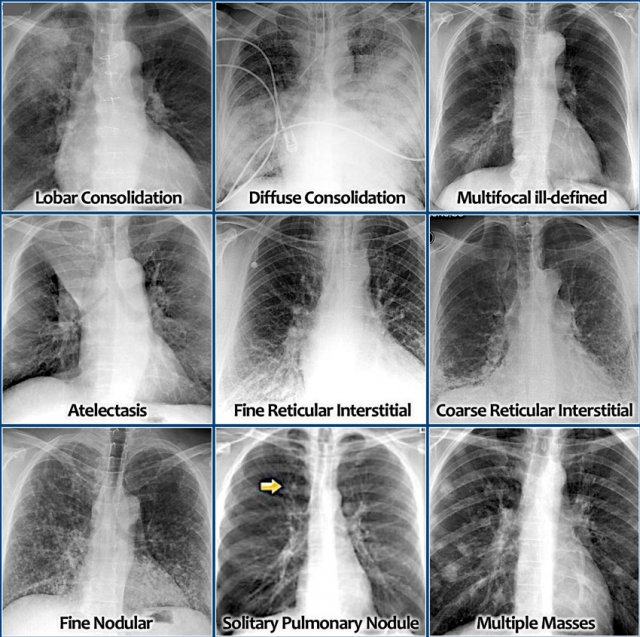
Radiology Pattern Overview
The Key Differentiating Features
1. Volume (THE Most Important Sign)
| Feature | Pneumonia (Consolidation) | Collapse (Atelectasis) |
|---|---|---|
| Lung volume | Preserved or increased (fissure bulging possible) | Reduced - hallmark sign |
| Fissure position | Normal or displaced away (bulging fissure = K. pneumoniae) | Displaced toward the opacity |
| Mediastinum | Stays midline or shifts away | Shifts toward the affected side |
| Diaphragm | Normal or depressed | Elevated on affected side |
| Trachea | Midline | Pulled toward affected side (upper lobe) |
"Plain chest radiography shows loss of lung volume and displacement of the lobar fissure, mediastinum, or diaphragm toward the involved lung unit" in atelectasis.
- Goldman-Cecil Medicine, p. 918
"Loss of volume is absent or minimal during the acute stage of consolidation [pneumonia]"
- Fishman's Pulmonary Diseases and Disorders, p. 2136
2. Air Bronchogram Sign
| Feature | Pneumonia | Collapse |
|---|---|---|
| Air bronchogram | Present - classic finding | Absent in obstructive collapse (the bronchus is blocked) - may be present in non-obstructive/compressive atelectasis |
An air bronchogram is the outline of an airway made visible because surrounding alveoli are filled with fluid/exudate - this is characteristic of lobar pneumonia but absent when a bronchus is obstructed (as in obstructive atelectasis).
3. Shape and Margins
| Feature | Pneumonia | Collapse |
|---|---|---|
| Shape | Segmental or lobar, fluffy borders, non-geometric | Wedge-shaped, triangular, or band-like; sharper borders |
| Density | Homogeneous opacification with air bronchograms | Dense, uniform, often wedge-shaped opacity |
| Plate-like (discoid) | Not typical | Horizontal/curvilinear lines = subsegmental atelectasis |
4. Clinical Context Aids Interpretation
| Feature | Pneumonia | Collapse |
|---|---|---|
| Fever, cough, sputum | Typically present | Often absent (may have mild fever post-op) |
| Typical setting | Community-acquired, infection | Post-op, ICU, mucus plug, central mass, foreign body |
| Leukocytosis | Common | Absent (unless secondary infection) |
| Onset | Gradual or subacute | Can be sudden (foreign body) or gradual |
Visual Examples
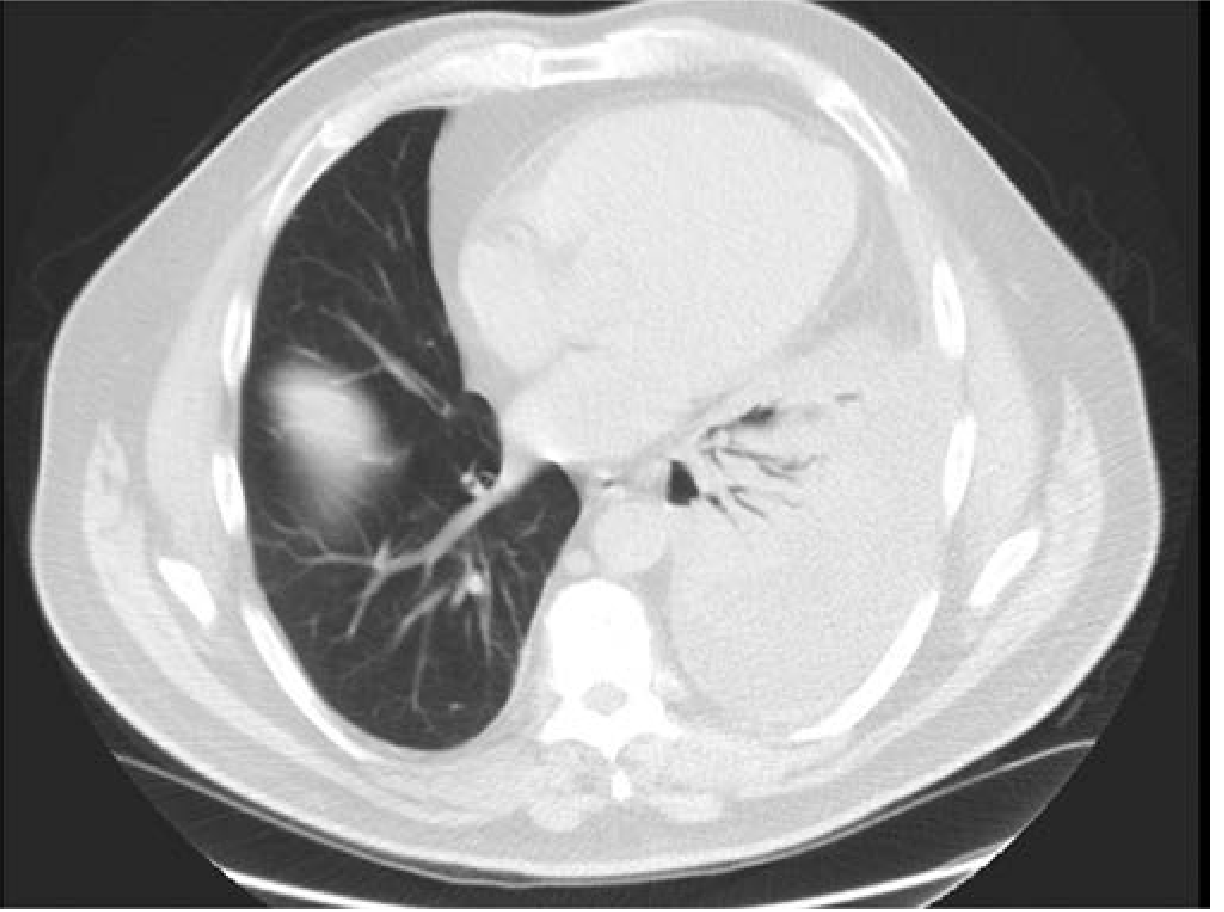
Lobar Pneumonia (CT - left side): Note the dense left-sided consolidation with visible air bronchograms (the bright branching airways running through the white opacity). Volume is maintained.
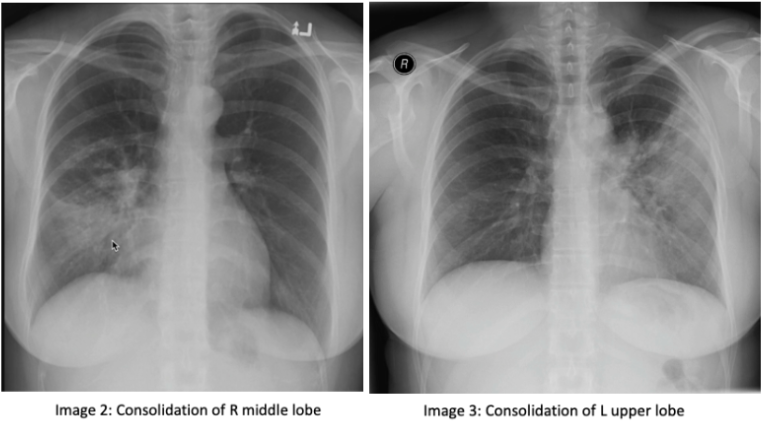
Consolidation patterns (pneumonia):
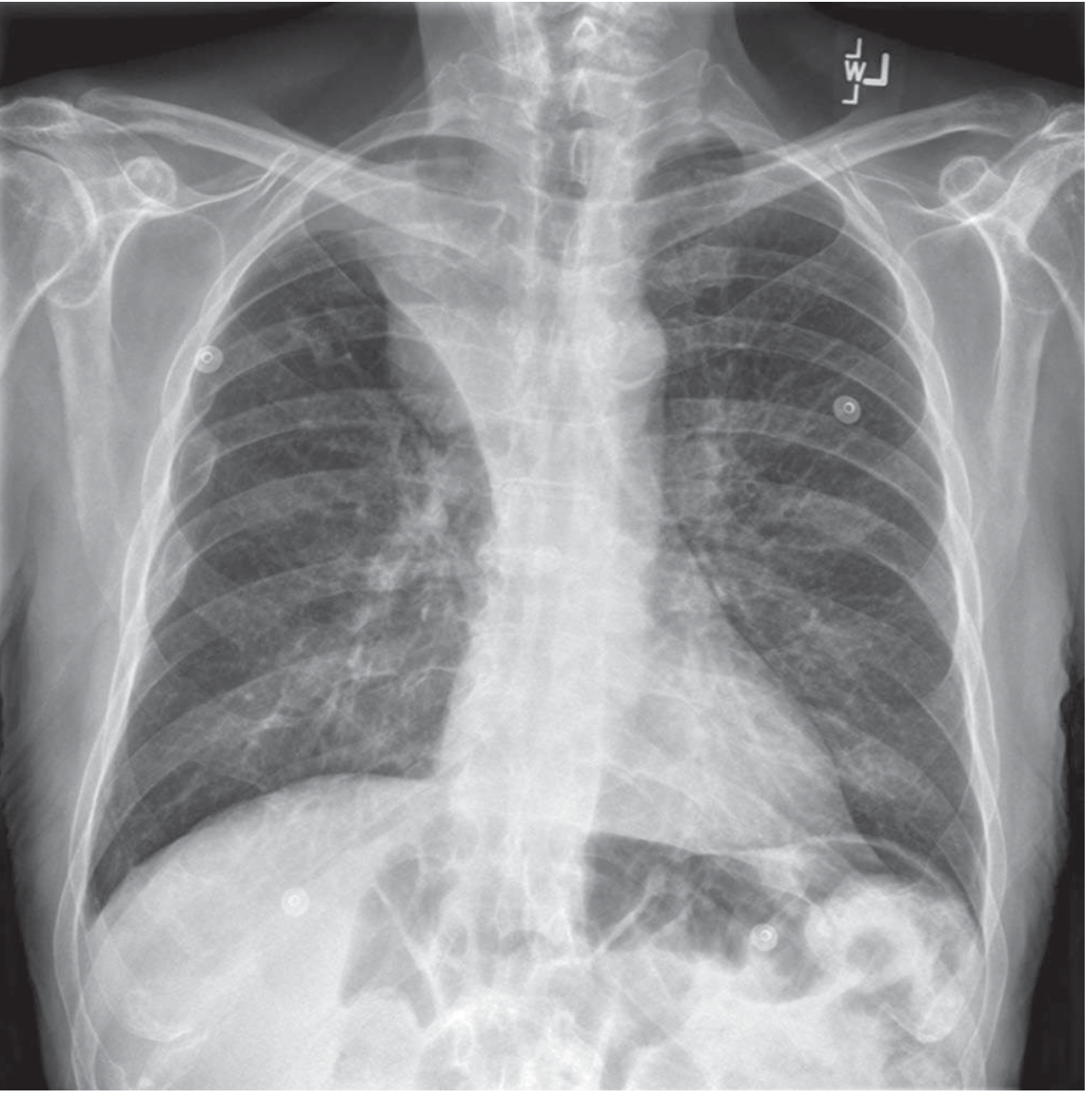
Right upper lobe atelectasis (CXR - caused by endobronchial tumor):
Types of Collapse (Atelectasis) and Their CXR Patterns
Per Goldman-Cecil Medicine and Fishman's:
| Type | Mechanism | CXR Clue |
|---|---|---|
| Obstructive/Resorptive | Bronchial obstruction (mucus plug, tumour, foreign body) | Lobar collapse with ipsilateral mediastinal shift; no air bronchogram |
| Compressive/Passive | Pleural effusion or pneumothorax pushes lung away | Associated with pleural opacity or air |
| Plate-like/Discoid | Hypoventilation (post-op, immobility) | Horizontal linear bands at bases |
| Rounded | Pleural disease traps adjacent lung (asbestos) | Ovoid pleural-based mass (can mimic tumour) |
Quick Summary - The "Volume Rule"
- Pneumonia: white opacity + normal or expanded volume + air bronchograms + clinical infection signs
- Collapse: white opacity + reduced volume + structures pulled toward the opacity + often no air bronchogram
When in doubt, CT resolves the question by showing bronchial obstruction, lung necrosis, or air bronchograms definitively.
Sources: Goldman-Cecil Medicine (p. 918); Fishman's Pulmonary Diseases and Disorders (p. 2136-2137); Radiology Assistant chest patterns
This is a shared conversation. Sign in to Orris to start your own chat.