Coronary artery of anatomy
Reading File
Finding Sources
Searching the Web
coronary artery anatomy overview branches territories
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a thorough overview of coronary artery anatomy, sourced from the Textbook of Clinical Echocardiography and Sabiston Textbook of Surgery.
Coronary Artery Anatomy
Origins
The two coronary arteries are the first arterial branches of the aorta, each arising from its respective sinus of Valsalva just above the aortic valve:
- Left Main Coronary Artery (LMCA / LCA) - originates from the left coronary sinus (left sinus of Valsalva). It courses posterolateral to the main pulmonary trunk for about 1 cm before dividing.
- Right Coronary Artery (RCA) - originates from the right coronary sinus (right sinus of Valsalva). Its ostium averages 2-3 mm in diameter.
CT Reconstruction: Normal Coronary Anatomy
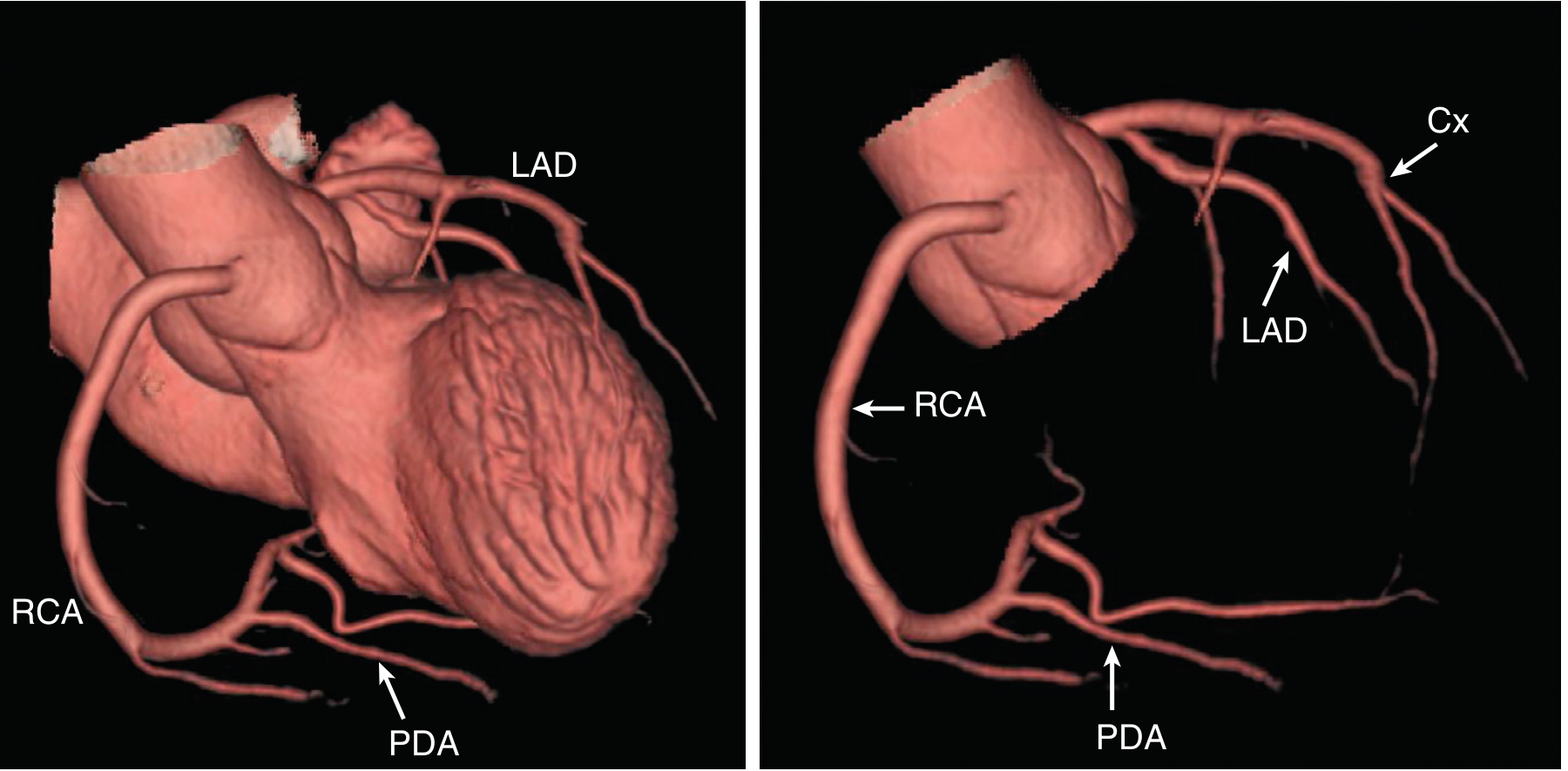
CT reconstruction showing the RCA giving rise to the PDA (left image), and the left main bifurcating into LAD and circumflex (Cx) with septal and obtuse marginal branches (right image).
Left Coronary System
The LMCA bifurcates into two major branches:
1. Left Anterior Descending Artery (LAD)
- Takes an anterolateral course relative to the pulmonary trunk
- Runs along the anterior interventricular groove toward (and sometimes around) the LV apex
- Key branches:
- Septal perforating branches - supply the anterior 2/3 of the interventricular septum
- Diagonal branches - supply the anterior wall of the left ventricle
- Forms an anastomosis with the PDA at the cardiac apex in many individuals
2. Circumflex Artery (Cx)
- Continues laterally in the atrioventricular groove
- Branches into obtuse marginal (OM) branches that travel toward the apex
- Terminates as the left posterolateral branch
- Supplies the lateral wall of the LV
In ~15% of individuals, the LMCA trifurcates rather than bifurcates, producing a third branch called the ramus intermedius (ramus intermediary), which arises between the LAD and Cx.
Right Coronary Artery (RCA)
- Runs rightward and obliquely in the right atrioventricular sulcus (groove)
- Provides the principal blood supply to the free wall of the right ventricle
- Key branches:
- Posterior Descending Artery (PDA) - also called the inferior interventricular artery; supplies the inferior ventricular septum and adjacent walls, and the septal papillary muscle of the mitral valve
- Right Posterolateral Artery
- Acute Marginal Artery (AMA) - runs along the acute margin of the heart toward the apex, supplying the lateral aspect of the RV
- AV Nodal Artery (AVNA) - descends to supply the atrioventricular node; occlusion can cause heart block or arrhythmias
Coronary Dominance
Dominance is determined by which vessel gives rise to the PDA (posterior descending artery) and the AV nodal artery:
| Dominance | Frequency | PDA Origin |
|---|---|---|
| Right dominant | ~80-85% | RCA |
| Left dominant | ~8-10% | Circumflex (Cx) |
| Codominant | ~7% | Both RCA and LCA |
Myocardial Territory Supply
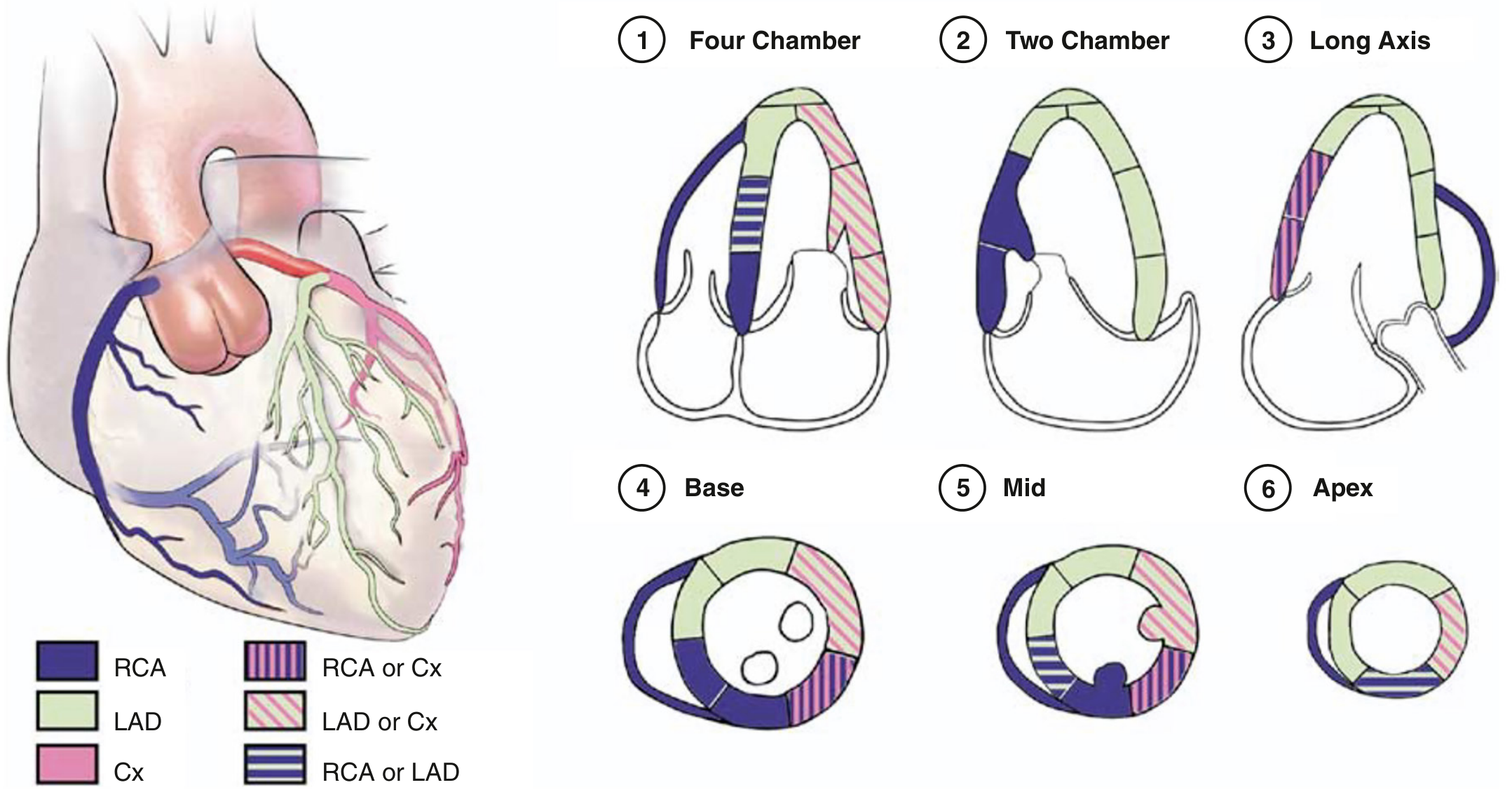
The diagram shows the myocardial territories supplied by RCA (blue), LAD (green), and Cx (pink) across four-chamber, two-chamber, long-axis, and short-axis (base, mid, apex) echocardiographic views.
| Territory | Supplying Artery |
|---|---|
| Anterior wall + anterior septum | LAD (via diagonals and septal perforators) |
| Lateral wall | Cx (via obtuse marginal branches) |
| Inferior septum + inferior wall | PDA (usually from RCA) |
| Inferolateral / posterior LV wall | RCA extensions or Cx obtuse marginals (variable) |
| RV free wall | RCA (acute marginal branches) |
| AV node | RCA (in ~90%) |
| SA node | RCA (in ~55%), Cx (in ~45%) |
| LV apex | Variable - LAD, PDA, or both |
The 17-Segment Model (Clinical Standard)
The LV is divided into three levels from base to apex - basal, mid-cavity, and apical - yielding 17 myocardial segments (a 16-segment model is commonly used in clinical echocardiography since the apical cap is difficult to visualize). Wall motion abnormalities in these segments help localize the culprit coronary artery in ischemia or infarction.
Sources:
- Textbook of Clinical Echocardiography, Chapter 8: Coronary Artery Anatomy
- Sabiston Textbook of Surgery: Coronary Artery Anatomy and Physiology
Thoracic duck anatomy
Asking for Preferences
Finding Sources
Searching the Web
thoracic duct anatomy course branches tributaries
Reading File
Finding Sources
Loading Image
Finding Sources
Reading Web Page
https://www.earthslab.com/anatomy/thoracic-duct-formation-co…
Here is a comprehensive overview of thoracic duct anatomy.
Thoracic Duct Anatomy
Overview
The thoracic duct is the largest lymphatic vessel in the body, measuring 38-45 cm long and 2-5 mm in diameter. Its lymph has a milky white appearance because it carries chyle (fat digestion products) from the intestines. The duct has numerous internal valves, giving it a beaded appearance.
Area of Drainage
The thoracic duct drains lymph from most of the body - everything EXCEPT:
- Right side of the head and neck
- Right side of the chest wall
- Right lung and right side of the heart
- Right surface of the liver
- Right upper extremity
These excluded regions drain into the right lymphatic duct, which empties into the right subclavian and internal jugular veins.
Formation and Origin
The duct begins at the lower border of T12, as a continuation of the cisterna chyli - a sac-like lymphatic reservoir lying anterior to the bodies of L1 and L2 vertebrae in the retrocrural abdomen.
Course
The thoracic duct travels through three regions:
1. Abdomen
- Begins as a continuation of the cisterna chyli at L1-L2
- Enters the thorax through the aortic hiatus of the diaphragm at T12
2. Thorax (Posterior and Superior Mediastinum)
- Ascends in the posterior mediastinum, running to the right of midline along the front of the vertebral bodies
- At T5, it crosses the midline from right to left
- Enters the superior mediastinum, running along the left border of the esophagus
- Proceeds toward the root of the neck
3. Neck (Root of Neck / Cervical Part)
- Arches laterally at the level of C7, in front of the vertebral system (vertebral artery and vein) and the left cervical sympathetic trunk
- Passes behind the carotid system (left common carotid artery, left internal jugular vein, left vagus nerve)
- The summit of the arch is 3-4 cm above the clavicle
- Descends in front of the first part of the left subclavian artery
- Terminates by opening into the junction of the left subclavian vein and left internal jugular vein (the left venous angle)
Anatomy and Course: Illustrated
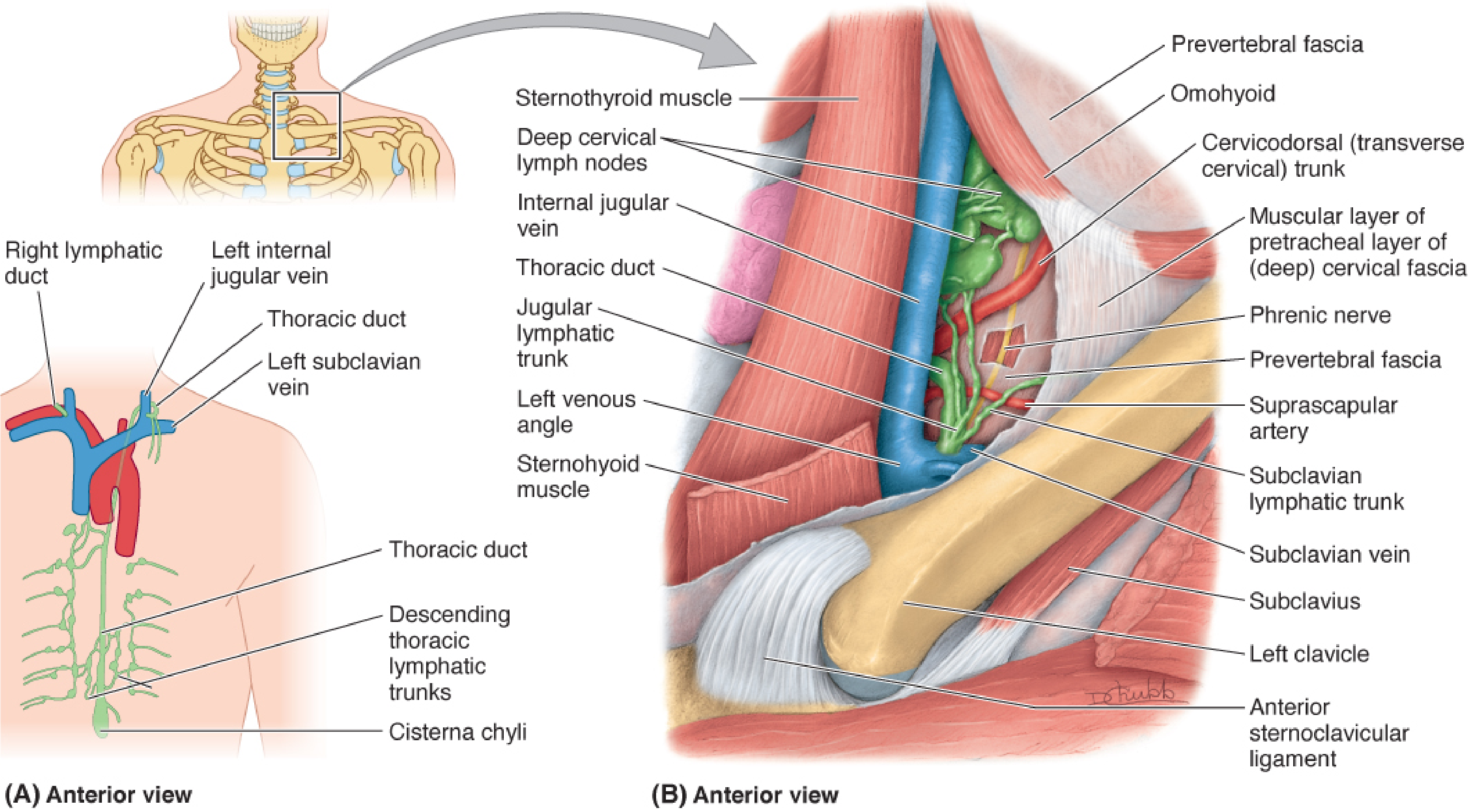
Fig. 91.11 - Fischer's Mastery of Surgery: (A) Anterior overview showing the thoracic duct rising from the cisterna chyli and terminating at the left venous angle. (B) Detail of the deep cervical lymph nodes and the termination of the duct, with the jugular lymphatic trunk, subclavian lymphatic trunk, and the left venous angle labeled.
Relations
| Region | Anterior | Posterior | Right | Left |
|---|---|---|---|---|
| Aortic hiatus (T12) | Median arcuate ligament | T12 vertebra | Azygos vein | Aorta |
| Posterior mediastinum | - | Vertebral bodies | Azygos vein | Descending thoracic aorta |
| Superior mediastinum | - | Vertebral column | Edge of esophagus | Lung and pleura |
| Root of neck | Carotid sheath (L. common carotid, L. IJV, L. vagus) | - | - | - |
Tributaries
The thoracic duct receives lymph from:
In the abdomen:
- Cisterna chyli (which itself receives efferents from the intestinal trunk, lumbar trunks, and lower intercostal lymph nodes)
- Efferents from lower 6 intercostal lymph nodes (both sides)
In the thorax:
- Intercostal lymphatic trunks (posterior intercostal nodes)
- Mediastinal lymphatic trunks
- Bronchomediastinal trunks (from lungs, bronchi, mediastinal nodes)
In the neck:
- Jugular lymphatic trunk (from deep cervical nodes)
- Subclavian lymphatic trunk (from left upper limb)
- Left bronchomediastinal trunk (in some individuals)
Right Lymphatic Duct (Counterpart)
The right lymphatic duct is much shorter (~1.25 cm) and drains the regions excluded by the thoracic duct (right head, neck, arm, and thorax). It empties into the right venous angle (junction of right subclavian and internal jugular veins).
Clinical Relevance
- Chylothorax - leakage of chyle into the pleural space; can result from trauma, surgery (especially esophagectomy or thoracic surgery), or malignancy at any point along the duct's long course. Triglycerides >110 mg/dL in pleural fluid is pathognomonic.
- The duct's crossing at T5 is a surgically important landmark - injuries above T5 tend to cause left-sided chylothorax, while injuries below T5 tend to cause right-sided chylothorax.
- Ligation for chylothorax is typically performed just above the diaphragm (supradia-phragmatic approach) to capture the main duct before it branches.
Sources:
- Fischer's Mastery of Surgery, 8th ed. - Chapter 91: Anatomy of the Thoracic Duct
- Murray & Nadel's Textbook of Respiratory Medicine - Chylothorax section
- Earthslab - Thoracic Duct Formation, Course & Tributaries
This is a shared conversation. Sign in to Orris to start your own chat.