Portal pyemia
Reading File
Finding Sources
Finding Sources
Searching PubMed
portal pyemia pylephlebitis
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a thorough answer. Here is the complete overview:
Portal Pyemia
Definition
Portal pyemia (also called pylephlebitis) is septic/suppurative thrombophlebitis of the portal vein or its tributaries. It arises when an infectious process within the territory drained by the portal venous system seeds the portal vein with bacteria, leading to infected thrombus formation and, if unchecked, bacteremic seeding of the liver with resultant pyogenic liver abscesses (PLAs).
- Sabiston Textbook of Surgery, p. 1884
- Goldman-Cecil Medicine, p. 2990
Pathophysiology
The portal venous system drains the entire gastrointestinal tract. Any infectious disorder within this drainage territory can trigger ascending portal vein infection. The sequence is:
- Intra-abdominal infection (e.g., appendicitis, diverticulitis) leads to bacterial entry into mesenteric veins
- Infection propagates proximally - portal vein becomes inflamed and thrombosed (pylephlebitis)
- Septic emboli or bacteremic seeding reaches the liver via the portal vein
- Multiple pyogenic liver abscesses form, typically in the right lobe (most portal flow goes there)
Portal pyemia accounts for approximately 20% of all pyogenic liver abscesses. Biliary obstruction (from malignancy or benign disease) accounts for 50-60%, making it the most frequent cause today.
- Goldman-Cecil Medicine, p. 2990
- Current Surgical Therapy, p. 103
Causes / Precipitating Conditions
| Category | Examples |
|---|---|
| Colorectal/appendiceal | Appendicitis (historically #1), diverticulitis, perforated colon |
| Anorectal | Strangulated/gangrenous hemorrhoids with anorectal sepsis |
| Inflammatory bowel disease | Crohn's disease, ulcerative colitis with perforation |
| Pancreatic/biliary | Pancreatitis |
| Pelvic | Pelvic inflammatory disease |
| Neonatal | Omphalitis (infection of umbilical stump) |
| Iatrogenic | Prior biliary-enteric anastomosis |
Historically, untreated appendicitis was the single most common cause. With the advent of prompt antibiotic therapy and early surgical treatment of intra-abdominal infections, portal pyemia has become less frequent - biliary disease has replaced it as the leading cause of pyogenic liver abscess. - Sabiston Textbook of Surgery, p. 1883
Clinical Features
Symptoms of portal pyemia overlap with those of pyogenic liver abscess:
- Fever (90%) - often high with rigors and sweating; abnormally rapid pulse is a constant finding regardless of temperature
- Right upper quadrant pain (60%)
- Jaundice - if present, suggests suppurative pylephlebitis with bile duct involvement, not just subphrenic abscess
- Tachycardia - a more reliable indicator than temperature
- Tachypnoea
- Non-specific: malaise, weight loss, anorexia
In acute portal vein thrombosis with pylephlebitis: fever, chills, and right upper quadrant pain are the triad that must be ruled out.
- S. Das Manual of Clinical Surgery, p. 530
- Yamada's Textbook of Gastroenterology, p. 437
Microbiology
The organisms reflect the source of infection:
- Enteric/portal origin: Bacteroides fragilis and other anaerobes; E. coli, Klebsiella spp., Streptococcus spp.
- Most infections are polymicrobial
- Klebsiella pneumoniae - prominent in Asia, often monomicrobial and linked to cryptogenic abscesses and colorectal neoplasms
- Gram-negative organisms predominate in Europe and Asia; in the USA, Streptococcus spp. are most commonly isolated
Blood cultures are positive in over 50% of cases.
- Current Surgical Therapy, p. 105
Investigations
Laboratory:
- Leukocytosis (90%)
- Elevated alkaline phosphatase (80%)
- Hyperbilirubinaemia (50%)
- Transaminase elevation (50%)
- Blood cultures (positive >50%)
Imaging:
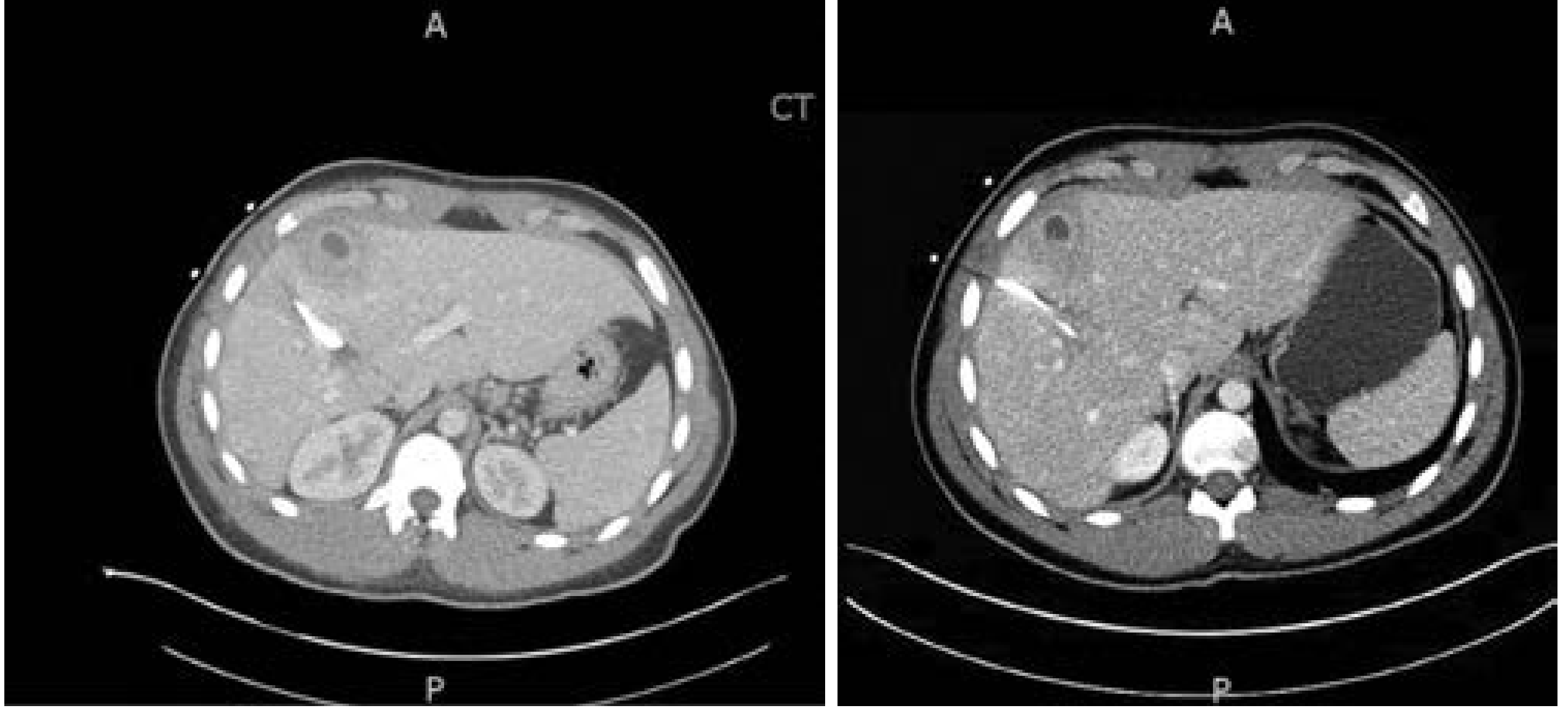
- CT abdomen with IV contrast - most sensitive; liver abscesses appear hypoattenuated, may show loculations and peripheral rim enhancement; portal venous gas may be visible if pylephlebitis is the source
- Ultrasound - 80-95% sensitive; less sensitive than CT; preferred initial test in paediatrics; shows absence of portal flow
- Doppler US - demonstrates solid hyperechoic material within portal vein lumen and absence of flow
- MRI - useful for confirmation and assessing thrombosis extent
- Plain X-ray - may show hepatomegaly, air-fluid levels, portal venous gas
CT images showing liver abscess with rim enhancement (from pyogenic liver abscess secondary to portal pyemia):
- Maingot's Abdominal Operations, p. 232
- Current Surgical Therapy, p. 118
Treatment
1. Antibiotics
Empiric therapy must cover streptococci, gram-negative bacilli, and anaerobes:
- Piperacillin/tazobactam (monotherapy) - first-line
- Ceftriaxone + metronidazole - alternative
- Carbapenems - for patients with prior biliary instrumentation or history of liver transplant (ESBL coverage)
Duration is guided by clinical response and resolution on follow-up imaging at 4-6 weeks. All patients with concomitant abdominal infection or septic pylephlebitis should receive antibiotics.
2. Source Control
- Treat the precipitating intra-abdominal infection (appendicectomy, colectomy segment resection, drainage of pelvic abscess, etc.)
- Early local control is essential - e.g., in anorectal sepsis, prompt antibiotics and control of the anal source prevent progression to portal pyemia and hepatic abscesses
3. Drainage of Liver Abscesses
- Percutaneous catheter drainage (PCD) - standard of care for abscesses >5 cm; superior to needle aspiration alone
- PCD is recommended as first-line for all PLAs without evidence of rupture or concurrent intraabdominal abscess requiring surgery
- Very large abscesses (>10 cm) may require multiple catheters
- Abscesses <3 cm may be managed with antibiotics alone
4. Anticoagulation
-
For portal vein thrombosis, anticoagulation to achieve recanalization is a treatment goal in acute PVT, in addition to treating the infection
-
Current Surgical Therapy, pp. 127-162
-
Yamada's Textbook of Gastroenterology, p. 455
Complications
| Complication | Notes |
|---|---|
| Multiple pyogenic liver abscesses | Classic complication; often right lobe; may be large |
| Septicaemia/septic shock | From bacteraemia |
| Portal vein thrombosis | Can lead to portal hypertension |
| Gastro-oesophageal varices | Develop within 1-12 months of PVT |
| Intestinal ischaemia/infarction | If thrombus extends into superior mesenteric vein (4-10%) |
| Subphrenic abscess | From local extension |
| Jaundice | From bile duct involvement |
- Sleisenger & Fordtran, p. 1409
- Yamada's Textbook of Gastroenterology, p. 435
Historical Note
The landmark 1938 study by Ochsner and DeBakey (reviewing 286 cases plus 47 new cases) established the classical description of pyogenic liver abscess, with appendicitis as the dominant cause via portal pyemia. This was before the antibiotic era, when untreated appendicitis would frequently progress to this lethal complication. - Sabiston Textbook of Surgery, p. 1884
Summary
Portal pyemia = septic thrombophlebitis of the portal vein from intra-abdominal infection → bacteremic seeding of the liver → pyogenic liver abscesses. It accounts for ~20% of PLAs today (down from being the historic leading cause). The clinical triad is fever/rigors + tachycardia + right upper quadrant pain in the context of an intra-abdominal infective focus. Management requires broad-spectrum antibiotics covering anaerobes and gram-negatives, source control, and percutaneous or surgical drainage of resulting liver abscesses.
This is a shared conversation. Sign in to Orris to start your own chat.