Pulmonary embolism
Reading File
Finding Sources
Searching PubMed
"pulmonary embolism"[MeSH Terms] AND "diagnosis"[MeSH Terms]
Searching the Web
pulmonary embolism 2025 guidelines diagnosis treatment ESC
Reading File
Reading File
Reading Web Page
https://www.jacc.org/doi/10.1016/j.jacc.2025.12.023
Reading File
Loading Image
Finding Sources
Reading File
Finding Sources
I now have comprehensive information to write a detailed, well-organized response on pulmonary embolism. Let me compile everything.
Pulmonary Embolism (PE)
Definition & Overview
Pulmonary embolism is the obstruction of one or more pulmonary arteries by thrombus (most commonly), air, fat, amniotic fluid, or tumor. The vast majority of cases arise from deep vein thrombosis (DVT) of the lower extremities. PE is a leading cause of cardiovascular mortality - approximately 25% of sudden cardiac deaths are attributed to it.
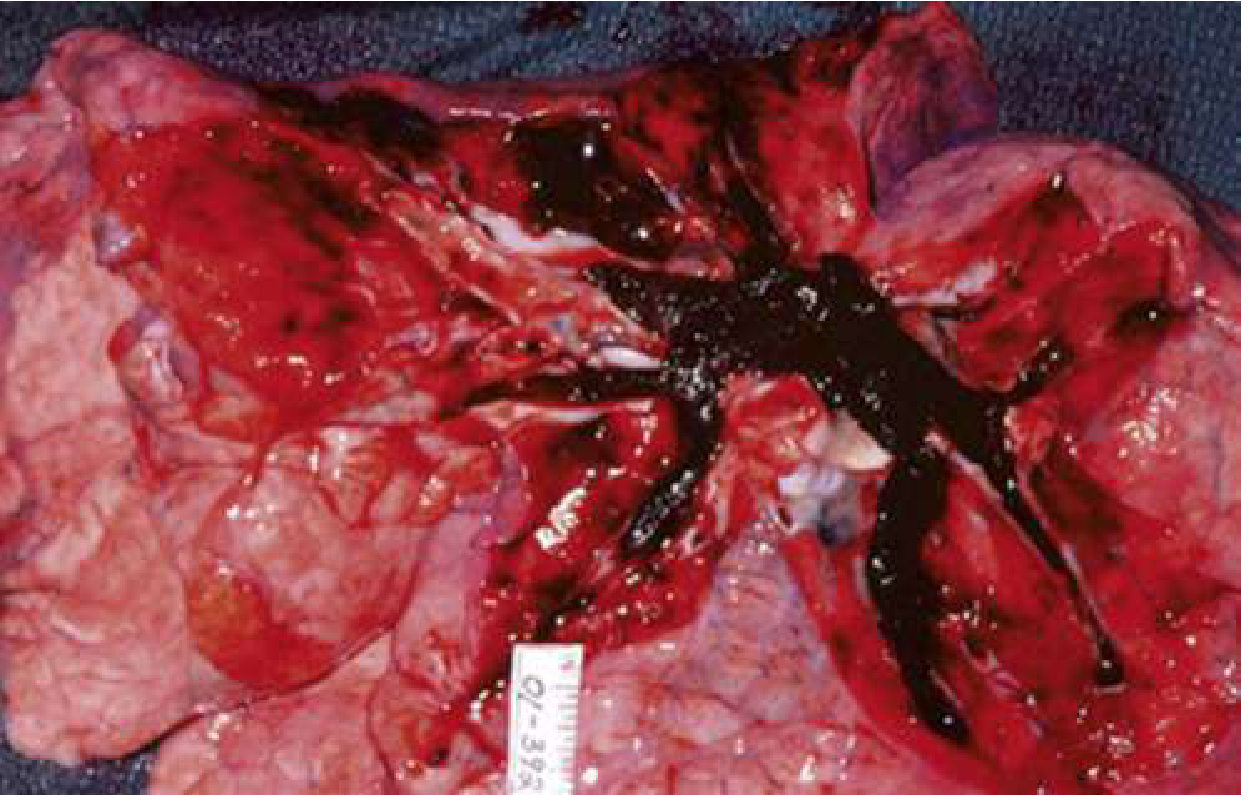
Autopsy specimen: massive PE completely occluding the right ventricular outflow system. Rosen's Emergency Medicine, p. 1202
Pathophysiology
PE causes two major physiologic derangements:
Hemodynamic effects:
- Mechanical obstruction raises pulmonary vascular resistance, increasing right ventricular (RV) afterload
- RV dilation and dysfunction follow, causing septal shift and impairing left ventricular filling
- Decreased cardiac output -> systemic hypotension -> cardiovascular collapse in severe cases
- Neurohormonal mediators (serotonin, histamine, thromboxane A2) cause additional vasoconstriction
Respiratory effects:
- Dead space ventilation increases (perfused but not ventilated alveoli)
- Hypoxemia from V/Q mismatch, shunting, and reduced mixed venous O2 saturation
- Pulmonary infarction occurs in ~10% of cases, typically from peripheral emboli in patients with limited collateral supply
Risk Factors (Virchow's Triad)
| Category | Examples |
|---|---|
| Stasis | Prolonged immobility, long flights, heart failure, stroke |
| Hypercoagulability | Active cancer, pregnancy, oral contraceptives, antiphospholipid syndrome, inherited thrombophilias (Factor V Leiden, prothrombin G20210A, protein C/S/antithrombin deficiency) |
| Endothelial injury | Surgery (especially orthopedic, pelvic), trauma, indwelling catheters |
Clinical Presentation
The presentation ranges from completely asymptomatic to sudden cardiovascular collapse.
Symptoms (in order of frequency):
- Dyspnea - most common (75-80% of patients); notably absent in ~25%, so its absence does not rule out PE
- Chest pain - second most common; may be pleuritic (sharp, worsens with breathing) - only present in ~20% of PE cases and indicates peripheral embolism with pulmonary infarction
- Hemoptysis - associated with pulmonary infarction
- Unilateral leg swelling - present in <30% of patients but relatively specific when accompanying dyspnea/chest pain
- Syncope - seen in <5% of PE presentations; unexplained syncope with risk factors warrants PE workup
- Palpitations, fatigue, nonspecific malaise
Massive PE warning signs:
- Shock index >1 (heart rate > systolic BP)
- Overt respiratory distress
- Syncope or seizure-like activity
- Pulseless electrical activity (PEA) arrest
Fever due to PE is typically low-grade; temperature >38.6°C (101.5°F) should suggest infection rather than infarction. - Rosen's Emergency Medicine, p. 1202
Diagnosis
Step 1: Pre-Test Probability (PTP) Assessment
Wells Score (most widely used):
| Criterion | Points |
|---|---|
| Clinical signs/symptoms of DVT | 3 |
| Alternative diagnosis less likely than PE | 3 |
| Heart rate >100 bpm | 1.5 |
| Immobilization or surgery in prior 4 weeks | 1.5 |
| Prior DVT or PE | 1.5 |
| Hemoptysis | 1 |
| Active malignancy | 1 |
- Score ≤4: Low probability (PE unlikely)
- Score >4: High probability (PE likely)
Revised Geneva Score (fully objective, no subjective component):
- Age >65: 1 | Prior PE/DVT: 3 | Recent surgery/immobilization: 2 | Active cancer: 2
- Unilateral leg pain: 3 | Hemoptysis: 2 | HR 75-94: 3, HR ≥95: 5 | Unilateral leg edema + pain on palpation: 4
- Low: 0-3 | Intermediate: 4-10 | High: >10
Both scores perform similarly in clinical practice. - Rosen's Emergency Medicine, p. 1205
Step 2: PERC Rule (for LOW pre-test probability patients)
If clinical gestalt suggests LOW probability AND all 8 criteria are met, PE can be excluded without any testing:
- Age <50
- Pulse <100
- SaO2 >94%
- No unilateral leg swelling
- No hemoptysis
- No recent trauma or surgery
- No prior PE/DVT
- No hormone use
The PERC rule has been validated in large studies in both the US and Europe. - Rosen's Emergency Medicine, p. 1205
Step 3: D-Dimer
- Sensitivity: 95-98%, Specificity: 40-55%
- A negative D-dimer in a patient with low-to-intermediate PTP effectively rules out PE
- Age-adjusted D-dimer cutoff: (Age × 10 µg/L) in patients >50 years - increases specificity without significant loss of sensitivity
- D-dimer is NOT useful in high-PTP patients (proceed directly to imaging)
- Elevated in many conditions: pregnancy, surgery, trauma, infection, malignancy - reducing specificity in hospitalized patients
Step 4: Imaging
CT Pulmonary Angiography (CTPA) - imaging modality of choice
- Sensitivity ~83%, specificity ~96% for PE
- Can visualize thrombus to the segmental level
- Also evaluates for RV dilation (prognostic indicator)
- Preferred in most non-pregnant patients
V/Q Scanning
- Preferred in pregnancy (lower fetal radiation: ~0.011-0.022 cGy vs. CTPA)
- Also preferred in patients with contrast allergy or renal insufficiency
- Interpreted as: Normal (excludes PE), Low/Intermediate/High probability
- Diagnostic when high-probability scan + high clinical probability
Compression Ultrasonography (CUS) of legs
- Can confirm DVT and support PE diagnosis without CT in selected patients
Echocardiography
- RV dilation (RV:LV ratio >0.9), septal flattening ("D sign"), reduced TAPSE
- Not diagnostic but critical for risk stratification and hemodynamic assessment
- A negative bedside echo does not rule out PE
Pulmonary Angiography - gold standard historically; now largely replaced by CTPA
ECG & CXR Findings
ECG (changes in <20% of cases):
- Sinus tachycardia (most common)
- S1Q3T3 pattern (classic but insensitive)
- New right bundle branch block
- Right axis deviation
- T-wave inversions in V1-V4
Chest X-ray (often normal or nonspecific):
- Hampton's hump - wedge-shaped pleural-based opacity (pulmonary infarct)
- Westermark sign - oligemia distal to obstructed vessel
- Fleischner sign - dilated central pulmonary artery
Risk Stratification
The 2026 AHA/ACC Multisociety Guideline (the first ever from AHA/ACC on this topic) introduces a new 5-category classification (A-E):
| Category | Description |
|---|---|
| A | Low risk, low clot burden |
| B | Low-intermediate risk |
| C | Intermediate risk, RV dysfunction without hemodynamic compromise |
| D1-D2 | Intermediate-high risk, borderline hemodynamic status |
| E | High risk - hemodynamic instability/shock |
This replaces the older massive/submassive/low-risk terminology and is designed to guide evidence-based therapeutic decisions. The 2019 ESC guidelines use a simpler high/intermediate-high/intermediate-low/low stratification based on hemodynamic instability and PESI score.
Treatment
Anticoagulation (cornerstone of therapy)
Initiate immediately when PE is suspected and bleeding risk is acceptable - do not wait for confirmatory imaging in high-PTP patients.
Preferred agents:
| Setting | Preferred Drug |
|---|---|
| Most patients (acute) | DOAC (apixaban or rivaroxaban) - monotherapy without parenteral bridging |
| Cancer-associated PE | LMWH or DOAC (rivaroxaban, apixaban, edoxaban) |
| If thrombolysis/surgery planned | IV unfractionated heparin (short half-life, easily reversible) |
| HIT | Fondaparinux, argatroban, apixaban, or rivaroxaban |
| Pregnancy | LMWH (DOACs and warfarin are contraindicated) |
- Apixaban (10 mg BID x7 days, then 5 mg BID) and rivaroxaban (15 mg BID x21 days, then 20 mg OD) are now first-line for most patients
- DOACs are preferred over warfarin for VTE treatment (equal or better efficacy, less bleeding)
- For IV UFH: weight-based dosing; many patients remain subtherapeutic in the first 24-48 hours
- Note on subsegmental PE: anticoagulation may be withheld if no DVT on bilateral leg ultrasound, no RV dysfunction, and no ongoing major thrombotic risk
Duration of anticoagulation:
- Provoked PE (reversible risk factor): minimum 3 months
- Unprovoked PE: at least 3-6 months; extended therapy considered based on bleeding risk
- Cancer-associated PE: indefinitely while cancer active
Reversal agents:
- UFH: protamine sulfate (near-complete reversal)
- LMWH: protamine (partial, ~50%)
- Apixaban/rivaroxaban: andexanet alfa (recombinant factor Xa decoy)
- Dabigatran: idarucizumab
Thrombolytic (Fibrinolytic) Therapy
Indications:
- Clear indication: Hemodynamic instability (SBP <90 mmHg or >40 mmHg drop from baseline) - "massive PE"
- Controversial: Intermediate-high risk (submassive PE with RV dysfunction but stable BP)
Regimens:
- Alteplase (rtPA): 100 mg IV over 2 hours (preferred), or 0.6 mg/kg over 15 min for cardiac arrest
- Reteplase: 10 units IV x2 doses, 30 min apart
- Tenecteplase: single weight-based IV bolus
Systemic thrombolysis carries a ~2% risk of intracranial hemorrhage - this is the primary reason it is reserved for life-threatening PE.
Advanced/Interventional Therapies
Per the 2026 AHA/ACC guideline, advanced therapies are:
- Reasonable for Category E (high-risk, hemodynamically unstable)
- Can be considered for Category D1-D2 (intermediate-high risk)
- A Class 1 recommendation is given for Pulmonary Embolism Response Teams (PERTs) - multidisciplinary teams for complex cases
Options include:
- Catheter-directed thrombolysis (CDT) - local low-dose tPA infusion; lower bleeding risk than systemic thrombolysis; recent meta-analysis (2025) vs. mechanical thrombectomy showed comparable outcomes
- Mechanical thrombectomy - catheter-based clot aspiration or fragmentation; growing evidence base
- Surgical embolectomy - for patients with massive PE when thrombolysis is contraindicated or failed
- IVC filter - reserved for PE with absolute contraindication to anticoagulation; not used instead of anticoagulation if anticoagulation is possible
Low-Risk PE: Outpatient Management
Validated criteria (PESI score, Hestia criteria) identify patients safe for discharge:
- Hemodynamically stable with normal vital signs
- No RV dysfunction on imaging or echocardiography
- No major comorbidities contraindicating home treatment
- Reliable access to anticoagulants and follow-up
Special Populations
PE in Pregnancy
- PE is the leading cause of maternal mortality in the US (~15% of maternal deaths)
- Risk is 5x higher than age-matched non-pregnant women
- Diagnosis complicated by: physiologic dyspnea of pregnancy, elevated baseline D-dimer, validated prediction rule limitations
- Imaging: V/Q preferred (lower fetal radiation); if CTPA used, halving the perfusion dose is standard
- Treatment: LMWH throughout pregnancy; DOACs and warfarin are contraindicated
- Murray & Nadel's Respiratory Medicine, p. 3029
PE with Cancer
- Highest recurrence and mortality risk
- Preferred anticoagulants: LMWH or DOACs (rivaroxaban, apixaban, edoxaban)
Chronic Complications
Chronic Thromboembolic Pulmonary Hypertension (CTEPH)
- Occurs in ~3-4% of patients after acute PE
- Persistent organized thrombus obstructs pulmonary vasculature -> progressive pulmonary hypertension
- Presents with exertional dyspnea, RV failure
- Diagnosed by V/Q scan + right heart catheterization
- Treatment: pulmonary endarterectomy (surgery of choice), balloon pulmonary angioplasty, or riociguat (medical therapy)
Post-PE Syndrome
- Dyspnea, exercise intolerance, quality-of-life impairment persisting after acute PE
- Distinct from CTEPH (no pulmonary hypertension at rest)
- Managed with supervised rehabilitation
Key Recent Updates (2026 AHA/ACC Guideline)
- New 5-category A-E classification replaces massive/submassive terminology
- Class 1 recommendation for PERTs (Pulmonary Embolism Response Teams)
- DOACs firmly established as first-line for most patients
- Mechanical thrombectomy and CDT recognized as equivalent options for high-risk patients
- This is the first-ever PE guideline from AHA/ACC, referenced as: Creager et al., J Am Coll Cardiol 2026
Sources:
- Rosen's Emergency Medicine, 9e (Chapters 74)
- Murray & Nadel's Textbook of Respiratory Medicine (Chapters 18, 81)
- 2026 AHA/ACC/Multisociety Guideline for Acute PE - JACC 2026;87:1626-1710
- Recent meta-analysis: Mechanical thrombectomy vs CDT for PE, PMID 40269600
This is a shared conversation. Sign in to Orris to start your own chat.