COPD According to medicine
Reading File
Finding Sources
Finding Sources
Searching PubMed
"chronic obstructive pulmonary disease"[MeSH Terms] AND "management"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
I now have very rich data from Harrison's, Robbins, and Goldman-Cecil. I have comprehensive content on definition, epidemiology, pathogenesis, pathology, classification, clinical features, investigations, and treatment. Let me now compile the full answer.
Chronic Obstructive Pulmonary Disease (COPD)
Sources: Harrison's Principles of Internal Medicine 22E (2025), Robbins & Kumar Basic Pathology, Goldman-Cecil Medicine, Murray & Nadel's Textbook of Respiratory Medicine
Definition
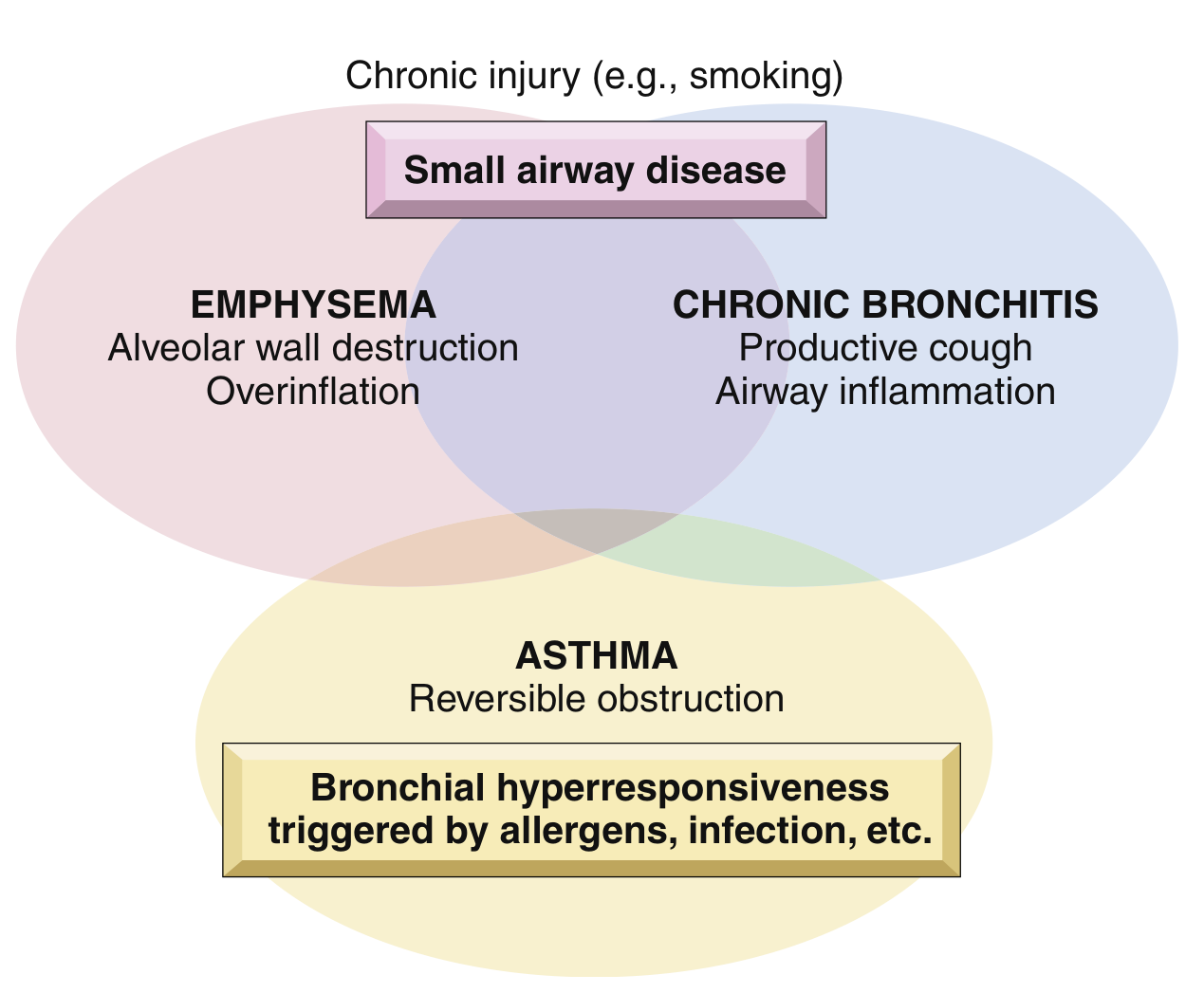
COPD is defined as a disease state characterized by persistent respiratory symptoms and airflow obstruction due to airway and/or alveolar abnormalities caused by exposure to noxious particles or gases. It is an umbrella term encompassing:
- Emphysema - anatomically defined by alveolar destruction and air space enlargement
- Chronic bronchitis - clinically defined by productive cough for ≥3 months in each of 2 consecutive years
- Small airway disease - narrowed and reduced small bronchioles
Airflow obstruction is confirmed by spirometry: post-bronchodilator FEV1/FVC < 0.7 (GOLD criteria).
Epidemiology
- Estimated 480 million individuals with COPD worldwide (projected 592 million by 2050) - Harrison's 22E
- Third leading cause of death worldwide; ~3.2 million deaths annually
- Fourth leading cause in the United States, affecting >15 million persons
- Typically presents in the sixth decade or later
- Annual cost in the U.S.: ~$50 billion ($30B direct + $20B indirect)
- 35-50% of heavy smokers develop COPD; ~80% of COPD is attributable to smoking
- Women appear more susceptible than men to developing COPD
Risk Factors
| Factor | Details |
|---|---|
| Cigarette smoking | Major risk factor; dose measured in pack-years; inversely related to FEV1 |
| Biomass fuel combustion | Cooking/heating in poorly ventilated spaces (major in developing world) |
| Occupational dust | Mines, grain-handling, cotton mills |
| Environmental air pollution | Associated with increased mortality in established COPD |
| Abnormal lung development | Childhood respiratory infections impair lung growth |
| Genetics | α1-antitrypsin deficiency; ~1% of emphysema patients |
| Vaping/cannabis | Increasing concern, especially in adolescents (Harrison's 22E) |
Pathogenesis
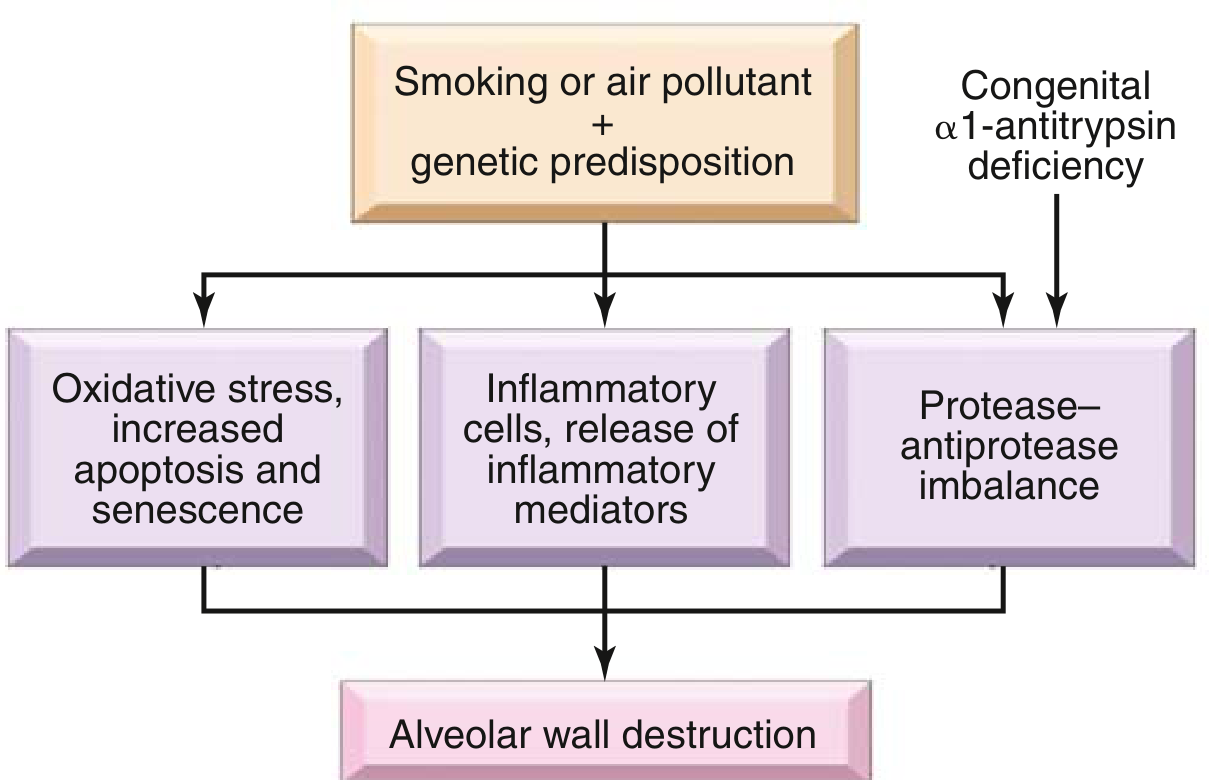
Three key mechanisms drive tissue destruction in COPD:
1. Protease-Antiprotease Imbalance
- Inflammatory cells release proteases (especially elastase) that break down connective tissue
- α1-antitrypsin is the major inhibitor of neutrophil elastase - its deficiency (Pi ZZ genotype, chromosome 14) causes panacinar emphysema, earlier and more severe in smokers
-
80% of Pi ZZ homozygotes develop symptomatic emphysema
2. Inflammatory Cells and Mediators
- Key cells: neutrophils, macrophages, CD4+ and CD8+ T cells
- Mediators: leukotriene B4, IL-8, TNF-α
- Serve to recruit more inflammatory cells, amplify inflammation, and induce structural changes
3. Oxidative Stress
- Reactive oxygen species from cigarette smoke + release from macrophages/neutrophils
- Cause tissue damage and amplify inflammation
Airway Levels Affected
- Large airways: mucus gland enlargement, goblet cell hyperplasia → chronic bronchitis
- Small airways (≤2 mm): major site of airflow resistance; narrowed by cells, mucus, fibrosis
- Alveoli: progressive destruction → emphysema; loss of elastic recoil → air trapping
Pathology
Emphysema Patterns
| Type | Location | Association |
|---|---|---|
| Centriacinar (centrilobular) | Central/proximal acinus; upper lobes predominant | Cigarette smoking - 20x more common |
| Panacinar (panlobular) | Entire acinus uniformly enlarged; lower lobes | α1-antitrypsin deficiency |
| Distal acinar (paraseptal) | Near pleura/septa; upper half | Young adults, spontaneous pneumothorax |
| Irregular | Irregular acinar involvement with scarring | Usually clinically insignificant |

Mechanistically: loss of elastic tissue in alveolar walls reduces radial traction on respiratory bronchioles → collapse during expiration → functional airflow obstruction.
Chronic Bronchitis Morphology
- Hypertrophy of mucous glands in trachea/large bronchi
- Reid index (mucous gland thickness : bronchial wall thickness) elevated above the normal 0.4
- Goblet cell metaplasia, mucus plugging, inflammation (lymphocytes, macrophages - NOT eosinophils)
- Small airway disease: bronchiolitis with submucosal fibrosis → luminal narrowing
Clinical Features
Symptoms
- Dyspnea - usually the first symptom; insidious onset, steadily progressive
- Chronic cough with sputum production
- Wheezing
- Exacerbations (acute worsening of respiratory symptoms)
- Weight loss/cachexia in advanced disease (elevated TNF-α)
Physical Examination
| Finding | Significance |
|---|---|
| Prolonged expiratory phase | Airflow obstruction |
| Expiratory wheezing | Airway narrowing |
| Barrel chest | Hyperinflation |
| Hyperresonant percussion | Increased lung volumes |
| Poor diaphragmatic excursion | Flattened diaphragm |
| Use of accessory muscles | Severe obstruction |
| Tripod position (sitting forward, hands on knees) | Severe obstruction |
| Cyanosis (lips, nail beds) | Hypoxemia |
| Cor pulmonale (right heart failure) | Advanced disease, pulmonary hypertension |
| No clubbing - if present, investigate for lung cancer |
Classic Phenotypes
- "Pink Puffer" (emphysema dominant): thin, tachypneic, relatively preserved PaO2, hyperinflated
- "Blue Bloater" (chronic bronchitis dominant): cyanotic, edematous, hypercapnic, higher BMI, OSA risk
Investigations
Spirometry (Diagnostic Gold Standard)
- FEV1/FVC < 0.7 (post-bronchodilator) confirms airflow obstruction
- Obstruction is not fully reversible (differentiates from asthma)
GOLD Spirometric Grading (based on FEV1 % predicted, when FEV1/FVC <0.7):
| GOLD Grade | Severity | FEV1 % Predicted |
|---|---|---|
| 1 | Mild | ≥80% |
| 2 | Moderate | 50-79% |
| 3 | Severe | 30-49% |
| 4 | Very Severe | <30% |
GOLD ABE Assessment (combines symptoms + exacerbations to guide treatment):
- Uses CAT score (COPD Assessment Test) and modified MRC (mMRC) dyspnea scale
- Exacerbation history: 0-1 = low risk; ≥2 or ≥1 hospitalization = high risk
Other Investigations
| Test | Finding |
|---|---|
| Chest X-ray | Hyperinflation, flattened diaphragm, hyperlucency, bullae |
| HRCT chest | Definitive for emphysema type/distribution; detects bronchiectasis, lung cancer |
| Arterial Blood Gas | Hypoxemia, hypercapnia (PaCO2 >45 = type 2 respiratory failure), assess pH |
| Oximetry | SpO2; if ≤88% at rest → consider home oxygen |
| Diffusing capacity (DLCO) | Reduced in emphysema |
| Blood eosinophil count | Guides ICS use; higher eosinophils → better ICS response |
| α1-antitrypsin level | Check in young patients or non-smokers |
| 6-Minute Walk Test | Exercise capacity; component of BODE index |
BODE Index (Body mass index, airflow Obstruction, Dyspnea, Exercise tolerance) - better predictor of mortality than FEV1 alone.
Management
A. Smoking Cessation
The single most effective intervention to slow disease progression. Pharmacotherapy: nicotine replacement therapy, varenicline, bupropion.
B. Pharmacological Treatment
Bronchodilators are the cornerstone of stable COPD management:
| Drug Class | Examples | Notes |
|---|---|---|
| SABA (Short-Acting β2-Agonist) | Salbutamol (albuterol), terbutaline | PRN rescue; onset in minutes |
| SAMA (Short-Acting Muscarinic Antagonist) | Ipratropium | PRN or regular |
| LABA (Long-Acting β2-Agonist) | Salmeterol, formoterol, indacaterol | Twice or once daily |
| LAMA (Long-Acting Muscarinic Antagonist) | Tiotropium, aclidinium, umeclidinium | Once daily; preferred maintenance |
| ICS (Inhaled Corticosteroid) | Fluticasone, budesonide | Add-on; guided by blood eosinophils ≥300 cells/μL or frequent exacerbations |
| LABA + LAMA combination | Umeclidinium/vilanterol, tiotropium/olodaterol | Superior to either alone |
| Triple therapy (ICS + LABA + LAMA) | Fluticasone furoate/vilanterol/umeclidinium | For high exacerbation risk patients |
| PDE4 inhibitor | Roflumilast | Chronic bronchitis with frequent exacerbations; not a bronchodilator |
| Azithromycin | Macrolide | Reduce exacerbations (daily dosing); monitor for hearing and cardiac toxicity |
| Theophylline | Xanthine | Modest benefit; narrow therapeutic window; third-line |
GOLD 2024 Treatment Recommendations:
- Group A (few symptoms, low risk): SABA or SAMA PRN; escalate to LAMA or LABA if needed
- Group B (more symptoms, low risk): LAMA + LABA combination (preferred for moderate-severe dyspnea)
- Group E (high exacerbation risk): LAMA + LABA ± ICS (based on eosinophil count)
C. Non-Pharmacological Treatment
| Intervention | Details |
|---|---|
| Pulmonary Rehabilitation | Exercise training + education; improves dyspnea, exercise capacity, and quality of life |
| Long-Term Oxygen Therapy (LTOT) | PaO2 ≤55 mmHg or SpO2 ≤88% at rest; ≥15 hrs/day; reduces mortality in severe COPD |
| Vaccination | Influenza (annual), pneumococcal, COVID-19, RSV (in older patients) |
| Nutritional support | For cachexia/weight loss |
| Positive Airway Pressure (CPAP/NIV) | For COPD-OSA overlap; NIV for chronic hypercapnic respiratory failure |
D. Surgical / Bronchoscopic Interventions
| Procedure | Indication |
|---|---|
| Lung Volume Reduction Surgery (LVRS) | Upper-lobe predominant emphysema; improves survival in selected patients |
| Bronchoscopic lung volume reduction (valves, coils) | Less invasive alternative to LVRS |
| Bullectomy | Single giant bulla compressing adjacent lung |
| Lung transplantation | Very severe COPD; end-stage disease |
COPD Exacerbations
An acute exacerbation (AECOPD) is a sustained worsening of respiratory symptoms beyond normal day-to-day variation that requires a change in management.
Common Triggers:
- Respiratory infections (viral most common; bacterial: H. influenzae, S. pneumoniae, M. catarrhalis)
- Air pollution
- Non-adherence to medications
Management of AECOPD:
| Treatment | Details |
|---|---|
| Short-acting bronchodilators | Increase dose/frequency of SABA ± SAMA |
| Systemic corticosteroids | Prednisolone 40 mg/day × 5 days (reduces recovery time, treatment failure risk) |
| Antibiotics | If purulent sputum, clinical signs of infection; amoxicillin/azithromycin/doxycycline |
| Controlled oxygen | Target SpO2 88-92% (avoid hyperoxygenation and worsening hypercapnia) |
| NIV (Non-invasive ventilation) | pH <7.35 with PaCO2 >45 mmHg; reduces intubation and mortality |
| Invasive ventilation | Failure of NIV or contraindications |
Comorbidities
COPD rarely occurs in isolation. Key comorbidities to screen for:
- Cardiovascular disease (most common cause of death in mild-moderate COPD)
- Lung cancer (highest risk in smokers; clubbing = investigate for malignancy)
- OSA-COPD Overlap Syndrome - hypercapnia, pulmonary hypertension, higher mortality
- Depression and anxiety
- Osteoporosis (from ICS use and physical inactivity)
- Gastroesophageal reflux
- Frailty and sarcopenia
Prognosis
- BODE index is the best composite prognostic tool (BMI, Obstruction, Dyspnea, Exercise)
- Frequent exacerbations accelerate lung function decline
- Mortality predictors: severe FEV1, hypercapnia, cor pulmonale, low BMI, low 6MWT distance
- Smoking cessation + LTOT (when indicated) are the only interventions proven to reduce mortality in stable COPD
- Lung volume reduction surgery improves survival in a carefully selected subset
Sources: Harrison's Principles of Internal Medicine 22E (2025, McGraw Hill) - Chapter 303; Robbins & Kumar Basic Pathology - Chapter 11; Goldman-Cecil Medicine International Edition - Chapter 76; Murray & Nadel's Textbook of Respiratory Medicine
This is a shared conversation. Sign in to Orris to start your own chat.