Menstrual cycle
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
I now have everything needed for a thorough, well-illustrated response. Here is the complete overview:
The Menstrual Cycle
The menstrual cycle is a series of recurring hormonal and structural changes in the female reproductive system that prepare the uterus for pregnancy every ~28 days. If pregnancy does not occur, the endometrium is shed and the cycle begins again.
Overview
The cycle is driven by a precisely timed axis: hypothalamus → anterior pituitary → ovary → uterus. All four organs must function appropriately for a normal ovulatory cycle. The cycle is counted from Day 1 = onset of menstrual bleeding and is divided into two major phases separated by ovulation at midcycle (~Day 14 in a 28-day cycle).
- Berek & Novak's Gynecology, p. 264
Hormonal Overview Diagram
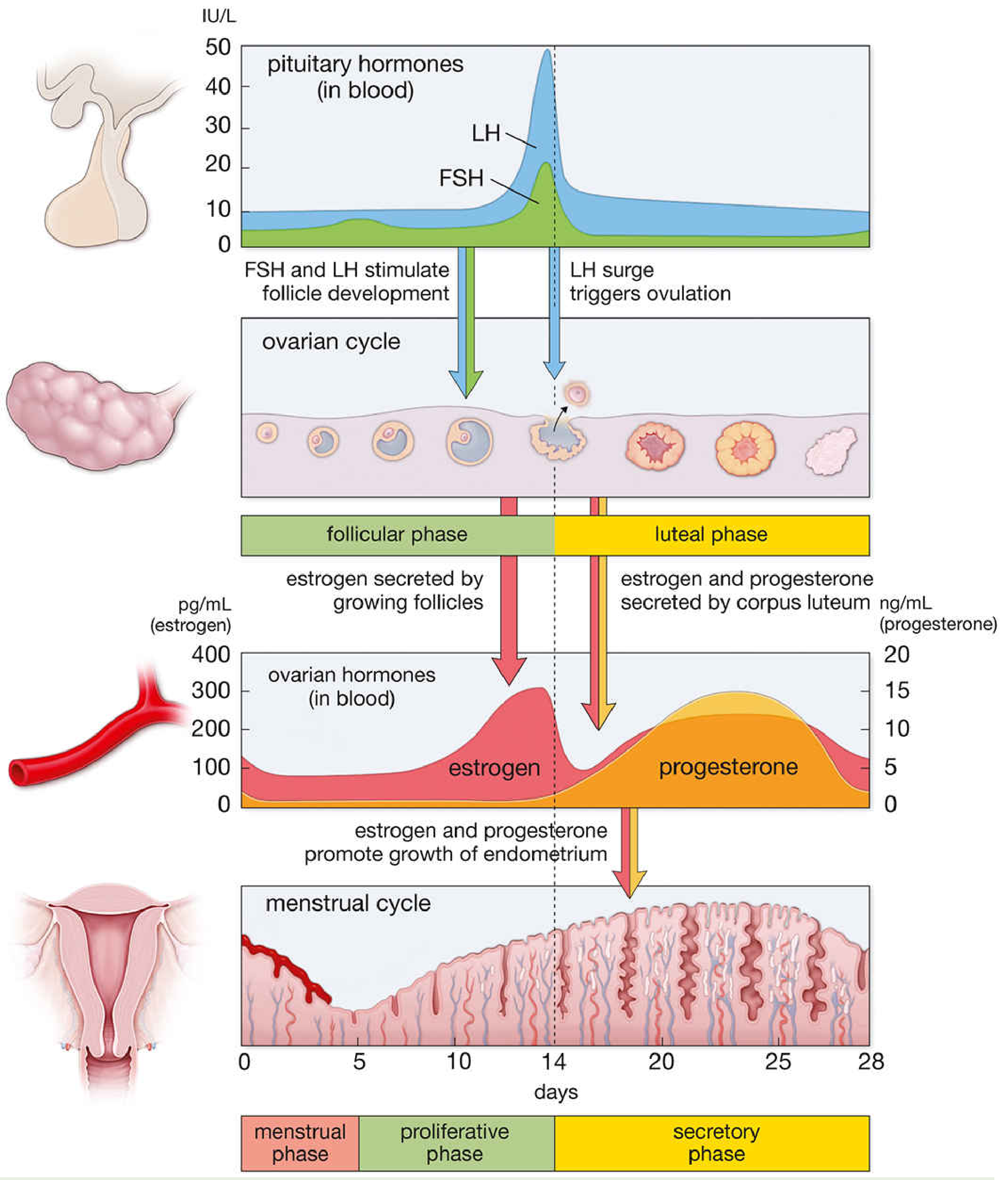
Relationship of morphologic and physiologic events across the menstrual cycle. FSH = follicle-stimulating hormone; LH = luteinizing hormone. - Histology: A Text and Atlas with Correlated Cell and Molecular Biology
The Hypothalamic-Pituitary Axis
GnRH - the master signal
Gonadotropin-releasing hormone (GnRH) is a decapeptide produced by neurons in the arcuate nucleus of the hypothalamus. It must be secreted in a pulsatile fashion to be effective. Continuous infusion causes downregulation of GnRH receptors on pituitary gonadotrophs and abolishes gonadotropin secretion, while pulsatile release upregulates receptors and drives normal FSH and LH secretion. GnRH has a half-life of only 2-4 minutes due to rapid proteolytic cleavage.
Pulse frequency varies across the cycle:
- Follicular phase: frequent, small-amplitude pulses
- Late follicular phase: increased frequency and amplitude
- Luteal phase: progressively longer intervals between pulses, higher but declining amplitude
This variation matters because decreasing GnRH pulse frequency reduces LH but increases FSH, which is important for recruiting follicles in the late luteal/early follicular transition.
- Berek & Novak's Gynecology, p. 270
FSH and LH
| Hormone | Target Cells | Key Action |
|---|---|---|
| FSH | Granulosa cells (only ovarian cells with FSH receptors) | Stimulates follicular growth and estradiol synthesis |
| LH | Theca and granulosa cells | Triggers ovulation (LH surge), forms corpus luteum, maintains luteal steroidogenesis |
- Costanzo Physiology 7th Edition, p. 477
Phase 1: Follicular Phase (Days 1-14) - also called the Proliferative Phase
Ovarian Events
- FSH and LH drive development of 10-20 primary follicles; selection of the dominant follicle occurs by days 5-7
- For the first 8-10 days, FSH is the principal hormone; it stimulates granulosa and thecal cells to secrete estrogens into the follicular lumen
- As estrogen production from the dominant follicle rises, it negatively feeds back on the pituitary to suppress FSH - the dominant follicle becomes FSH-independent while smaller follicles regress (atresia)
- Locally produced estradiol within the follicle mutually reinforces FSH's trophic effect: more granulosa cells → more estradiol → more cells
Endometrial Events (Proliferative Phase)
Estradiol drives growth and proliferation of the endometrium:
- Growth of endometrial glands and stroma
- Elongation of spiral arteries
- Cervical mucus becomes copious, watery, elastic - when spread on a slide it produces a "ferning" pattern, which creates channels that allow sperm penetration
Feedback Switch: Negative → Positive
In the early follicular phase, estradiol exerts negative feedback on the hypothalamus and pituitary, suppressing GnRH, FSH, and LH.
At midcycle, estradiol levels rise sharply. When estradiol reaches a critical level of ≥200 pg/mL plasma, the feedback reverses to positive: estradiol now up-regulates GnRH receptors on anterior pituitary gonadotrophs, causing a massive burst of FSH and LH secretion - the ovulatory surge.
- Costanzo Physiology 7th Edition, p. 477-478
Ovulation (Day ~14)
The LH surge induces rupture of the dominant follicle and release of the oocyte. Ovulation occurs approximately 34-36 hours after the start of the LH surge, or about 10-12 hours after the LH peak. Late in the follicular phase, just before ovulation, progesterone levels also begin to rise under LH influence.
- Histology: A Text and Atlas, p. 2242
Phase 2: Luteal Phase (Days 14-28) - also called the Secretory Phase
Ovarian Events
After ovulation, the granulosa and thecal cells of the ruptured follicle rapidly transform into the corpus luteum. The corpus luteum secretes estrogen and large amounts of progesterone. Both hormones now exert negative feedback on the hypothalamus/pituitary to suppress further FSH and LH secretion. Late in the luteal phase, GnRH pulse frequency slows further, which actually favors FSH over LH - beginning to recruit the next cohort of follicles.
If fertilization does not occur, the corpus luteum degenerates (~Day 26-28), estradiol and progesterone fall abruptly, and this withdrawal triggers menstruation.
Endometrial Events (Secretory Phase)
Under progesterone's dominance:
-
Endometrial proliferation slows; thickness decreases
-
Uterine glands become tortuous and accumulate glycogen in vacuoles
-
Stroma becomes edematous
-
Spiral arteries elongate and become coiled
-
Cervical mucus becomes thick, scant, non-elastic and does not fern (sperm penetration is no longer needed)
-
Costanzo Physiology 7th Edition, p. 479
Phase 3: Menstruation (Days 1-5 of the next cycle)
Regression of the corpus luteum causes an abrupt withdrawal of estradiol and progesterone. The distal portions of the spiral arteries vasoconstrict, causing ischemia and necrosis of the superficial endometrium. The tissue and blood are sloughed as menstrual flow, typically lasting 3-5 days. The straight arteries and proximal segments of the spiral arteries do not participate in these changes - they supply the basal layer which regenerates the endometrium in the next cycle.
- Histology: A Text and Atlas, p. 2240
Hormone-Level Diagram
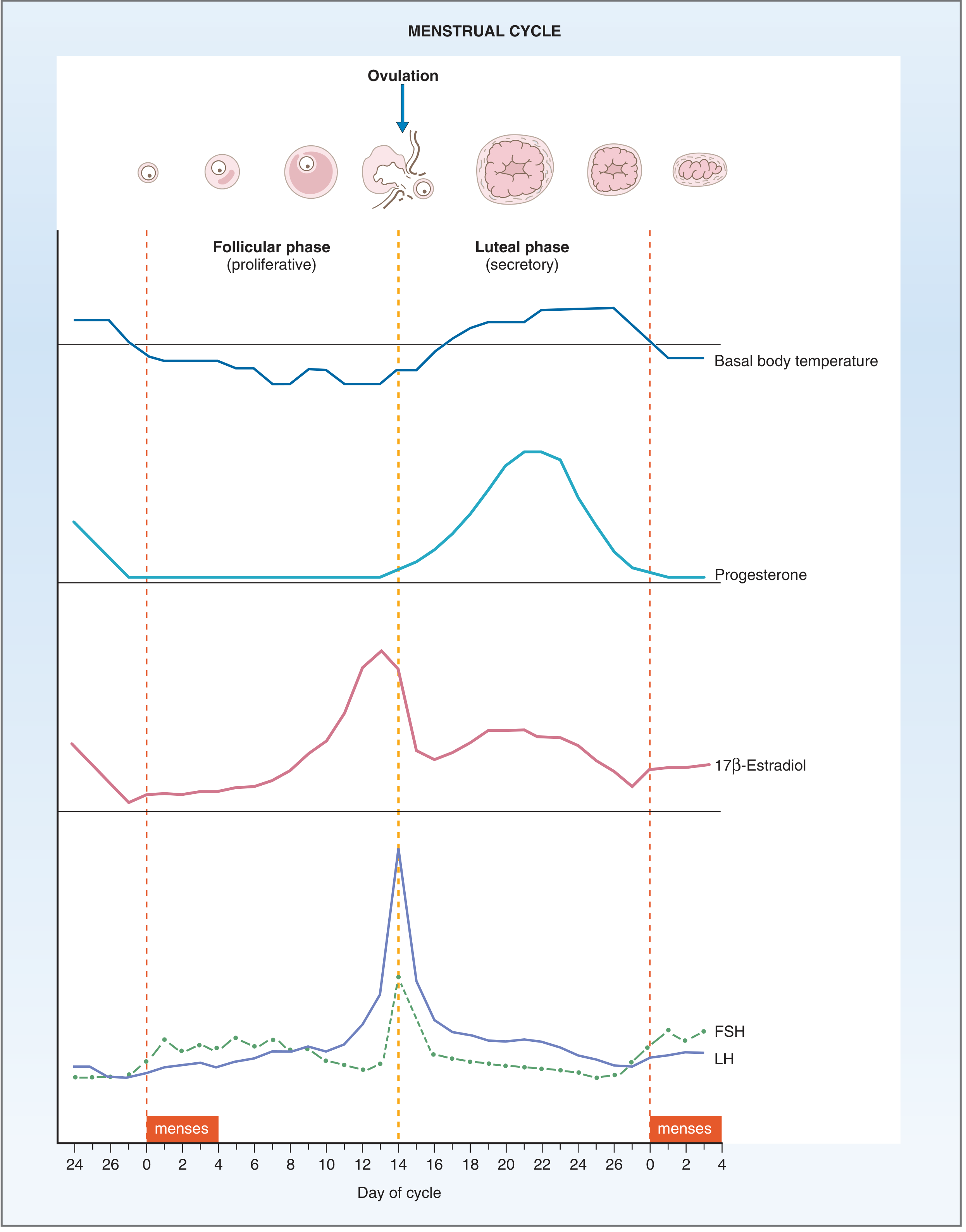
Fig. 10.10 Events of the menstrual cycle. - Costanzo Physiology 7th Edition, p. 480
Summary Table
| Phase | Days | Dominant Hormone | Ovarian Structure | Endometrium | Cervical Mucus |
|---|---|---|---|---|---|
| Menstrual | 1-5 | Low E2 & P4 | Primordial follicles recruiting | Shedding | - |
| Follicular / Proliferative | 1-14 | Estradiol (E2) | Growing → dominant follicle | Proliferating, glands grow | Watery, ferning, sperm-friendly |
| Ovulation | ~14 | LH surge | Follicle ruptures | - | Peak watery |
| Luteal / Secretory | 14-28 | Progesterone (P4) | Corpus luteum | Secretory, glycogen, edema | Thick, scant, no ferning |
Key Clinical Notes
- A normal cycle ranges from 21 to 35 days; the luteal phase is almost always ~14 days; it is the follicular phase that varies in length
- Basal body temperature rises ~0.2-0.5°C after ovulation due to progesterone's thermogenic effect (as shown in the Costanzo diagram above)
- If fertilization occurs, the embryo's trophoblast secretes hCG starting ~Day 8 post-ovulation, which "rescues" the corpus luteum and sustains progesterone production until the placenta takes over in the second trimester
- The straight arteries and proximal spiral arteries do not change during the cycle; only the distal spiral arteries respond to estrogen and progesterone - this protects the regenerative basal layer
This is a shared conversation. Sign in to Orris to start your own chat.