Give me a 10marks answer about Safety features of anaesthesia machine from standard textbooks for AIIMS md anaesthesia exams
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the content needed for a thorough 10-mark answer. Here is the complete structured answer:
Safety Features of the Anaesthesia Machine
(Source: Morgan & Mikhail's Clinical Anesthesiology, 7e; Miller's Anesthesia, 10e; Barash's Clinical Anesthesia, 9e)
Introduction
The modern anaesthesia machine (workstation) incorporates multiple layers of safety features designed to prevent the delivery of hypoxic gas mixtures, unintended volatile agent overdose, barotrauma, and electrical hazards. Equipment-related adverse outcomes are rarely from device malfunction - misuse is three times more prevalent than mechanical failure. The ASTM International standard (F1850-00) specifies the essential safety features that all modern workstations must incorporate.
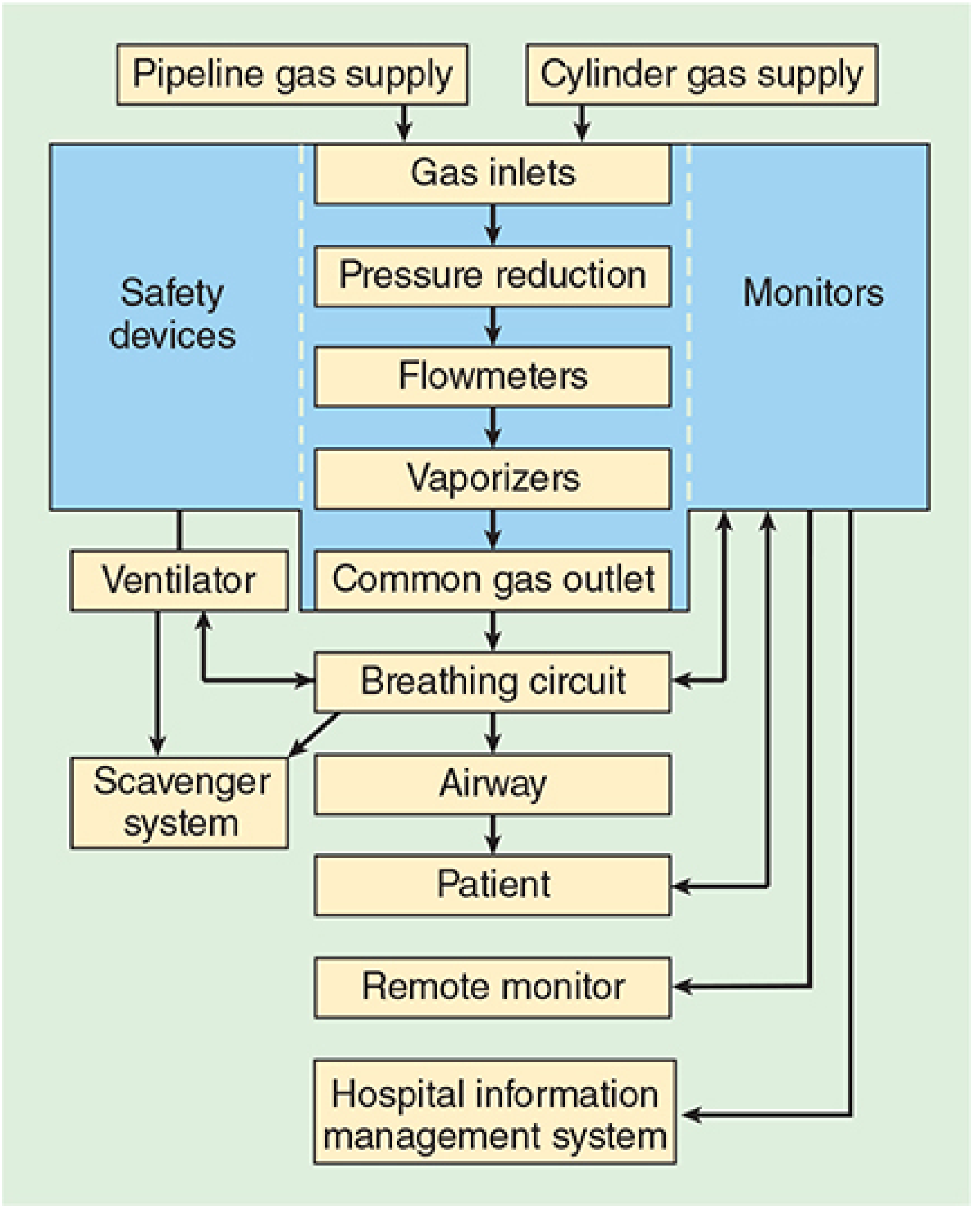
Figure: Functional schematic of the anaesthesia workstation - Morgan & Mikhail, 7e
I. Gas Supply Safety Features
1. Diameter Index Safety System (DISS) - Pipeline Inlets
- Oxygen and nitrous oxide are delivered via a piping network colour-coded and connected via non-interchangeable DISS fittings specific to each gas
- Interchangeability is prevented by making the bore diameter of the body and the connection nipple unique for each gas
- A filter traps debris from the wall supply; a one-way check valve prevents retrograde gas flow into the pipeline
- Pipeline pressure delivered to the machine: approximately 50 psig
- Purpose: Prevents incorrect pipeline attachment and detects supply failure or pressure fluctuation
2. Pin Index Safety System (PISS) - Cylinder Inlets
- Cylinders attach via hanger-yoke assemblies incorporating the Pin Index Safety System (PISS)
- Index pins on the yoke correspond to specific holes on the cylinder valve - each gas has a unique pin configuration, preventing attachment of the wrong cylinder
- Yoke assembly includes: index pins, a Bodok washer, a gas filter, and a check valve
- Cylinders are also colour coded (O₂ = green in North America; N₂O = blue)
- Cylinder gases are regulated down to 45 psig (slightly below pipeline pressure), ensuring preferential use of the pipeline supply when a cylinder is left open
- Purpose: Prevents incorrect cylinder attachment; provides backup gas in the event of pipeline failure
3. Pressure Regulators and High-Pressure Relief Valves
- Cylinder pressure (up to 1900 psig for O₂) is reduced by regulators to a safe working level
- A high-pressure relief valve for each gas opens when supply pressure exceeds 95-110 psig (e.g., in regulator failure)
- Purpose: Prevents dangerous pressure surges from reaching the machine
II. Oxygen Failure Protection Devices
4. Oxygen Failure Safety Device (Fail-Safe / Nitrous Cut-Off)
- Nitrous oxide, air, and other gases must pass through safety devices before reaching their flow control valves; oxygen passes directly
- These devices allow other gas flow only if sufficient oxygen pressure is present (sensed via a "piloting pressure" line from the oxygen inlet)
- Two types:
- Threshold shut-off valve (older): Closes completely if O₂ pressure falls below ~20 psig - entirely preventing N₂O flow
- Proportioning device / Balance regulator (modern): Proportionately reduces N₂O pressure in relation to falling O₂ pressure; completely shuts off N₂O only below a minimum O₂ pressure (e.g., 0.5 psig for N₂O, 10 psig for other gases)
- Previously called the "fail-safe" or "nitrous cut-off" valve
- Purpose: Prevents administration of N₂O or other gases when oxygen supply fails
5. Low Oxygen Pressure Alarm
- A pneumatic or electronic sensor activates an audible alarm when inlet oxygen pressure drops below a threshold value (usually 20-30 psig)
- Per ASTM standards, this alarm must be automatically enabled when the machine is switched on
- Limitation: Does not protect against gas line misconnections in which threshold pressure may be maintained by a gas containing no oxygen
III. Flowmeter Safety Features
6. Oxygen Positioned Downstream (Nearest to Vaporizer)
- In three-gas machines, oxygen flowmeter is always positioned furthest downstream (nearest to the vaporizer and common gas outlet)
- If a leak develops in or downstream from a proximal gas flowmeter (e.g., N₂O), the oxygen flowing last will dilute the effect
- Conversely, if the oxygen flowmeter itself leaks, no other gas can dilute the resulting hypoxic mixture - hence O₂ is kept last to minimise this risk
- Purpose: Reduces risk of delivering hypoxic mixtures in the event of a flowmeter leak
7. Oxygen/Nitrous Oxide Ratio Controller (Hypoxic Guard)
- Links N₂O and O₂ flow valves either pneumatically (e.g., Dräger Sensitive Oxygen Ratio Controller, SORC) or mechanically (e.g., Link-25 system on Datex-Ohmeda)
- Ensures a minimum oxygen concentration of 21-25% is always delivered, regardless of operator error in setting flowmeters
- If the operator attempts to set a hypoxic N₂O:O₂ ratio, the device automatically increases O₂ flow or decreases N₂O flow
- Purpose: Prevents delivery of a hypoxic gas mixture to the patient
8. Minimum Oxygen Flow
- The oxygen flow control valve is designed to deliver a minimum oxygen flow (typically 200-250 mL/min) automatically when the machine is switched on
- Achieved via a minimum flow resistor
- Purpose: Ensures some oxygen always enters the breathing circuit even if the operator forgets to set oxygen flow
9. Fluted, Colour-Coded, Touch-Coded Oxygen Knob
- The oxygen flow control knob is fluted, larger, and protrudes further than other knobs
- Purpose: Tactile and visual differentiation prevents inadvertent manipulation of the wrong gas
IV. Vaporizer Safety Features
10. Vaporizer Interlock (Exclusion) Device
- Interlocking devices prevent the simultaneous administration of more than one volatile agent from multiple vaporizers mounted on the back bar
- When one vaporizer is turned on, the others are mechanically locked off
- Purpose: Prevents accidental volatile agent overdose from multiple vaporizers
11. Agent-Specific Keyed Filling Ports
- Modern vaporizers use agent-specific, keyed filling adaptors so that the incorrect volatile agent cannot be introduced into a vaporizer
- Each filling system is colour-coded and physically unique per agent
- Purpose: Prevents filling a vaporizer with the wrong volatile agent (e.g., halothane into a sevoflurane vaporizer), which could cause overdose or underdose
12. Oxygen Flush Bypasses Vaporizers
- The oxygen flush valve delivers 100% O₂ at 35-75 L/min directly to the common gas outlet, bypassing all flowmeters and vaporizers
- Purpose: Allows rapid refilling or flushing of the breathing circuit without delivering volatile agents; also useful in emergency O₂ delivery
V. Breathing Circuit Safety Features
13. Breathing Circuit Pressure Monitor and Alarms
- Continuous monitoring of airway/circuit pressure with alarms for:
- Sustained positive pressure (suggests obstruction or ventilator malfunction - risk of barotrauma)
- High peak airway pressure
- Negative airway pressure (suggests fresh gas supply failure or inspiratory valve incompetence)
- Disconnection / low pressure alarm (most common cause of unrecognized breathing circuit failure)
- Purpose: Prevents pulmonary barotrauma; detects circuit disconnection or occlusion
14. Exhaled Volume Monitor
- Measures exhaled tidal and minute volumes
- Purpose: Detects hypoventilation and hyperventilation; confirms circuit integrity
15. Oxygen Concentration Monitor and Alarm
- A paramagnetic or fuel-cell oxygen analyser continuously measures FiO₂ within the breathing circuit
- Must be automatically enabled when the machine is turned on (per ASTM standards)
- Purpose: Provides a last line of defence against delivery of a hypoxic mixture in the event of a low-pressure system leak that the flowmeter-level safety features cannot detect
16. Capnography and Anaesthetic Gas Measurement
- Continuous end-tidal CO₂ and volatile agent monitoring
- Purpose: Guides ventilation; prevents anaesthetic overdose; helps detect oesophageal intubation and circuit disconnection; reduces awareness
VI. Electrical and Mechanical Safety Features
17. Backup Battery
- Modern machines have a battery backup capable of providing temporary electrical power for >30 minutes to all monitors and alarms in the event of power failure
- Purpose: Maintains essential monitoring even during mains power failure
18. Scavenger System
- Collects and disposes of waste anaesthetic gases (WAGs) from the circuit's adjustable pressure-limiting/pop-off (APL) valve and ventilator
- Purpose: Prevents contamination of the operating room environment; protects theatre personnel from chronic exposure to trace volatile agents and N₂O
Summary Table (ASTM Essential Safety Features)
| Safety Feature | Purpose |
|---|---|
| DISS pipeline fittings + filter + check valve | Prevents incorrect pipeline connections |
| Pin Index Safety System (PISS) for cylinders | Prevents incorrect cylinder connections |
| Low O₂ pressure alarm | Detects O₂ supply failure |
| Hypoxic guard (O₂:N₂O ratio controller) | Ensures minimum 21-25% O₂ delivery |
| O₂ failure safety device (fail-safe / proportioning) | Prevents N₂O flow when O₂ fails |
| O₂ flowmeter downstream to all other gases | Reduces hypoxia risk from proximal gas leak |
| O₂ concentration monitor + alarm (auto-enabled) | Last line of defence against hypoxic mixtures |
| Vaporizer interlock device | Prevents simultaneous multi-agent delivery |
| Agent-specific keyed filling ports | Prevents wrong-agent filling errors |
| O₂ flush bypasses vaporizers | Emergency circuit flush without volatile agent delivery |
| Circuit pressure monitor + alarms | Prevents barotrauma; detects disconnection |
| Exhaled volume monitor | Detects hypo/hyperventilation |
| Capnography + gas measurement | Guides ventilation; prevents overdose |
| Backup battery (>30 min) | Maintains monitors during power failure |
| Scavenger system | Protects OR personnel from WAGs |
Key Exam Points
- DISS (pipeline) and PISS (cylinder) are the two main connection safety systems - memorize what each prevents
- The "fail-safe" valve is a misnomer - it does NOT prevent hypoxia from gas line misconnections; it only responds to O₂ pressure drop
- The hypoxic guard (O₂:N₂O ratio controller) ensures a minimum 25% O₂ concentration; the O₂ analyser is the final safety net
- O₂ flowmeter is always last/downstream - if it leaks, no gas can dilute the resulting hypoxic mixture, which is why the analyser is indispensable
- Vaporizer interlock prevents simultaneous use; agent-specific filling ports prevent wrong-agent filling - these are two separate features
- Per ASA Closed Claims data, 35% of equipment-related adverse events could have been prevented by a proper pre-anaesthesia machine checkout
References: Morgan & Mikhail's Clinical Anesthesiology, 7e (Table 4-1, pp. 111-118); Miller's Anesthesia, 10e; Barash's Clinical Anesthesia, 9e
Find recent clinical guidelines on pre-anaesthesia equipment checks and maintenance protocols from millers, barasch, Morgan, Baheti, dorsch and dorsch
Finding Sources
Finding Sources
Searching PubMed
pre-anesthesia machine checkout checklist guidelines
Finding Sources
Finding Sources
Searching PubMed
anesthesia equipment safety check guideline
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Searching PubMed
anesthesia workstation checklist patient safety
Searching the Web
Baheti Dorsch Dorsch pre-anaesthesia machine check equipment maintenance protocol guidelines anesthesia
Searching PubMed
pre-anesthesia machine check compliance safety outcome
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC3821271
Note on Baheti and Dorsch & Dorsch: These two texts are not available in the library database, but their content has been retrieved via the Baheti textbook PDF (Understanding Anesthetic Equipment & Procedures, Dwarkadas K. Baheti et al.) and cross-referenced with the PMC article. Dorsch & Dorsch (Understanding Anesthesia Equipment, 5e) is referenced in both Miller's and the PMC article but is not in the digital library; key content from its protocols is captured below via those references.
Pre-Anaesthesia Equipment Check and Machine Maintenance Protocols
(Sources: Miller's Anesthesia 10e; Barash's Clinical Anesthesia 9e; Morgan & Mikhail's Clinical Anesthesiology 7e; Baheti - Understanding Anesthetic Equipment & Procedures; PMC3821271 [Indian Journal of Anaesthesia - Comprehensive PAC Protocol]; ASA Recommendations for Pre-Anaesthesia Checkout, 2008)
I. Background and Rationale
Improperly checking anaesthesia equipment prior to use can lead to patient injury, severe morbidity, and mortality. The ASA Closed Claims database shows equipment-related claims have fallen to approximately 1% of all claims - partly attributed to mandated PAC procedures. However, available evidence consistently shows that anaesthesia providers frequently do not perform a complete pre-anaesthesia check (PAC) and may miss faults even when explicitly looking for them on a sabotaged machine. In 35% of equipment-related adverse events, a proper PAC would have prevented the outcome.
Key facts (Miller's Anesthesia, 10e):
- A complete PAC must be performed each day before first use
- An abbreviated version must be performed before each subsequent case
- All contemporary anesthesia workstations have automated checkout procedures - but none can fully replace a manual checkout; automated checks differ between models and cannot be assumed to cover all critical items
II. Governing Guidelines and Standards
| Organisation | Standard / Guideline |
|---|---|
| ASA (USA) | Recommendations for Pre-Anesthesia Checkout Procedures (2008) - 15-item framework |
| FDA (USA) | Anesthesia Apparatus Checkout Recommendations (now superseded by ASA 2008) |
| AAGBI (UK) | Checking Anaesthetic Equipment (2012) - applicable to all workstations |
| ISO | ISO 80601-2-13:2011 - Safety and essential performance of anaesthetic workstations |
| ASTM International | F1850-00 - Standard specifications for anaesthesia machines |
Baheti (Understanding Anesthetic Equipment): Reproduces both the ASA 2008 15-item PAC and the AAGBI checklist as Appendices 1 and 2, noting the AAGBI checklist is applicable to all workstations and should be used alongside manufacturer-specific checks.
III. ASA 2008 Recommendations: The 15-Item PAC Framework
(Barash 9e, Appendix B; Miller's 10e, Table 20.6; Baheti, Appendix 1 & 2)
Items to be Completed DAILY (Before First Case)
| # | Item | Responsible Party | Rationale |
|---|---|---|---|
| 1 | Verify auxiliary O₂ cylinder and self-inflating manual ventilation device (Ambu bag) are available and functioning | Provider AND technician | Failure to ventilate is a major cause of anaesthesia morbidity/mortality; must be present at every anaesthetising location |
| 3 | Turn on anaesthesia delivery system; confirm AC power is available | Provider OR technician | Machine may run on battery backup silently - first sign of failure can be catastrophic system shutdown when battery is exhausted |
| 5 | Verify pressure is adequate on the spare O₂ cylinder mounted on the machine | Provider AND technician | Backup O₂ must be available if pipeline fails; valve should be closed after checking to prevent inadvertent emptying |
| 6 | Verify piped gas pressures ≥50 psig | Provider AND technician | Minimum supply pressure is required for proper machine function |
| 8 | Verify no leaks in the gas supply lines between flowmeters and the common gas outlet | Provider OR technician | The low-pressure section (flowmeters → vaporizers → common gas outlet) is most vulnerable; each vaporizer must be turned ON individually during leak test |
| 9 | Test scavenging system function | Provider OR technician | Protects OR personnel from waste anaesthetic gases |
| 10 | Calibrate (or verify calibration of) the O₂ monitor; check low-O₂ alarm | Provider OR technician | Final defence against hypoxic gas delivery |
Items to be Completed BEFORE EACH CASE
| # | Item | Responsible Party |
|---|---|---|
| 2 | Verify patient suction adequate to clear the airway | Provider AND technician |
| 4 | Verify availability of required monitors; check alarms (SpO₂, NIBP, capnography, ECG) | Provider OR technician |
| 7 | Verify vaporizers adequately filled; filler ports tightly closed | Provider ONLY |
| 11 | Verify CO₂ absorbent is not exhausted | Provider OR technician |
| 12 | Breathing system pressure and leak testing | Provider AND technician |
| 13 | Verify gas flows properly through the breathing circuit (inspiration and exhalation) | Provider AND technician |
| 14 | Document completion of checkout procedures (on patient chart) | Provider AND technician |
| 15 | Confirm ventilator settings; ANAESTHESIA TIME-OUT | Provider ONLY |
IV. Detailed Protocol by System: Pneumatic, Electrical, Electronic Components
(Synthesised from Miller's 10e; Morgan & Mikhail 7e [Table 4-3, FDA Checkout]; Baheti Appendix 2 [Ravishankar Protocol]; PMC3821271)
A. High-Pressure System
- Oxygen cylinder: Open O₂ cylinder; verify it is at least half full (≥1000 psig) (Morgan) or gauge pressure adequate (Miller's). Then close the cylinder valve - if left open and pipeline fails, the cylinder depletes silently.
- All gas cylinders: Check N₂O, air and other cylinders only if those gases are required for the case.
- Central pipeline supplies: Confirm all hoses are connected and pipeline gauges read ~50 psig.
- Colour coding and DISS connections: Visually inspect; perform a "tug test" (AAGBI/Baheti) to confirm correct insertion of each hose into its Schrader socket. (Note: Repeated disconnection of hoses to test the O₂ failure alarm may cause premature failure of the Schrader socket - the AAGBI therefore recommends checking the O₂ failure alarm weekly by disconnecting rather than daily.)
B. Low-Pressure System (Most Vulnerable to Leaks)
- Initial status check: Close all flow control valves; turn vaporizers off; check vaporizer fill levels and tighten filler caps.
- Negative-pressure leak test (for machines with a common gas outlet check valve):
- Attach suction bulb to the fresh gas outlet
- Squeeze bulb repeatedly until fully collapsed
- Verify bulb stays collapsed for ≥10 seconds (detects leaks as small as 30 mL/min)
- Repeat with each vaporizer turned on individually (to check vaporizer mount seals)
- Remove bulb; reconnect fresh gas hose
- Positive-pressure leak test (for machines without a check valve):
- Can use back-pressure through the breathing circuit
- Vaporizers must still be tested individually
- Vaporizer filler ports: Partially open filler ports are a common leak source. Automated checkout typically does NOT test for vaporizer leaks unless the vaporizer is opened during the test.
C. Flowmeters
- Turn on master switch and all electrical equipment.
- Adjust the flow of all gases through their full range; check for smooth operation of floats and undamaged flow tubes.
- Hypoxic guard test: Attempt to create a hypoxic O₂:N₂O mixture; verify the correct changes in flow or alarm activation (proportioning system check).
- Confirm minimum O₂ flow: With O₂ flow control valve off, verify O₂ flowmeter registers ~50-200 mL/min (minimum mandatory flow).
D. Scavenging System
- Ensure proper connections between the scavenging system and both the APL (pop-off) valve and the ventilator relief valve.
- Adjust waste gas vacuum if adjustable.
- Under-pressure test: With minimum O₂ flow, fully open APL valve, occlude Y-piece, allow scavenger reservoir bag to collapse completely - absorber pressure gauge should read ~zero.
- Over-pressure test: With O₂ flush activated, allow scavenger bag to distend fully - absorber pressure gauge should read <10 cmH₂O.
E. Breathing System / Circle System
- O₂ analyser calibration:
- Expose sensor to room air - should read 21%; if not, calibrate
- Verify low-O₂ alarm is enabled and functioning
- Reinstall sensor and flush with O₂ - should read >90%
- Circuit integrity: Check that breathing circuit is complete, undamaged, and unobstructed; verify unidirectional valves are present and moving correctly.
- CO₂ absorbent: Verify it is not exhausted (colour change indicates exhaustion).
- Leak test of breathing system:
- Set all gas flows to zero; close APL (pop-off) valve; occlude Y-piece
- Pressurize circuit to ~30 cmH₂O with O₂ flush
- Ensure pressure remains fixed for ≥10 seconds
- Open APL valve and verify pressure decreases
- Accessory equipment: Install humidifier, PEEP valve, and other circuit accessories planned for the case.
F. Ventilator
- Place a test lung (or second breathing bag) on the Y-piece.
- Set appropriate ventilator parameters for the next patient.
- Switch to automatic mode; turn ventilator on.
- Fill the bellows and cycle the ventilator; observe bellows function and unidirectional valves.
- Confirm minimum volume alarm is enabled and functioning.
- Check for adequate ventilation of test lung and confirm absence of leaks.
- Return to manual/bag mode before the patient is connected.
G. Monitors
- Check SpO₂, NIBP, ECG, ETCO₂, temperature probe, and nerve stimulator as appropriate.
- Self-test: The Baheti/Ravishankar protocol recommends using monitors on oneself (e.g., SpO₂ on own finger >96%; exhale into capnograph port to generate a CO₂ waveform) before applying to the patient.
- Set alarm limits appropriate for the patient's profile.
- Confirm gas sampling lines are properly attached, patent, and free from kinks.
H. Electrical/Electronic Components (Baheti / Ravishankar Protocol)
- Confirm machine is connected to mains (AC) and switch is on.
- Ensure battery has ≥30 min backup and is charging during machine use.
- For desflurane vaporizers: confirm electrical power and power-up self-test of the vaporizer.
V. The MS MAIDS Mnemonic (Miller's Anesthesia, 10e - Anesthesia Time-Out)
Before each case, an "Anaesthesia Time-Out" can be performed using this mnemonic (Box 20.3, Miller's 10e):
| Letter | Component |
|---|---|
| M - Machine | PAC complete; vaporizers filled, closed, dial at "0"; all gas flow knobs at zero; ventilator settings appropriate; APL valve open; machine in manual/spontaneous mode |
| S - Suction | Patient suction adequate to clear airway |
| M - Monitors | All required standard monitors present and ready |
| A - Airway | Primary airway equipment AND appropriate backup ready |
| I - Intravenous | IV lines, fluids, and associated equipment ready |
| D - Drugs | All medications available and properly labelled |
| S - Special | Any special or unique items (additional monitors, equipment) for the case are available |
VI. AAGBI Checklist Principles (Baheti, Appendix 1)
- Applicable to all anaesthetic workstations
- Should take only a few minutes to perform
- Is not intended to replace the manufacturer's pre-anaesthetic checks - use alongside them
- For machines with automated self-testing cycles on switch-on: functions tested by the machine need not be manually retested, but the operator must confirm what functions are covered
- The balance: "not so superficial that its value is doubtful, nor so detailed that it is impractical to use"
- O₂ failure alarm: The AAGBI recommends checking this on a weekly basis by disconnecting the O₂ hose (not daily), to avoid premature failure of the Schrader socket; a "tug test" is the daily standard
VII. Maintenance Protocols
Preventive Maintenance
- The PAC is not a replacement for required preventive maintenance (Barash, General Considerations)
- Anaesthesia machines should undergo scheduled professional servicing by manufacturer-certified biomedical technicians
- Clear documentation of regular servicing, component replacement, and satisfactory post-service functioning is mandatory (PMC3821271)
- Vaporizers should be serviced and recalibrated at manufacturer-recommended intervals (typically every 1-2 years)
Between Cases
- Test all new equipment intended for the next patient (suction tubing, breathing circuitry)
- Verify sufficient CO₂ absorbent and volatile agent
- If O₂ cylinder was used during a case: confirm it is at least half full or replace with a full cylinder
- During long procedures: periodically check for exhaustion of volatile agent and CO₂ absorbent
Handover During Long Cases (PMC3821271)
- If anaesthesiologist changes during a long procedure, a formal handover of machine check status must be given, including all component functioning
Machine Relocation
- Whenever an anaesthesia machine is moved to a new location, a complete beginning-of-day checkout must be performed (Barash, Basic Principles)
VIII. Limitations of Automated Checkout (Miller's 10e)
Automated checkout procedures:
- Differ between manufacturers and models
- Cannot be assumed to check all required items - reading the user manual does not always clarify what is being tested
- May not test for leaks at the vaporizer specifically, so loose filler caps or vaporizer mount leaks can be missed
- Many providers do not fully understand what automated checks cover, or make false assumptions about their machine's self-test
- Automated checks should clearly distinguish what is automatically tested from what requires manual checkout
- Ideally, date, time, and outcome of the most recent check should be recorded and accessible to the user
IX. Documentation
- Whoever conducts the PAC must document successful performance; the anaesthesia provider must include this on the patient chart (Barash, Basic Principles)
- Documentation serves as a quality control tool and medicolegal record
- Training in the PAC should also be formally documented, including competency items and successful completion
X. Key Exam Points
- The ASA 2008 Recommendations have 15 items - 15 items daily, 8 items before each subsequent case (items 2, 4, 7, 11-15)
- Item 7 (vaporizer check) and Item 15 (Anaesthesia Time-Out) are the only items exclusively the provider's responsibility - technicians cannot substitute
- The negative-pressure test (suction bulb method) is used on machines with a common gas outlet check valve; the positive-pressure test cannot be used on these machines
- Vaporizer leak test: each vaporizer must be turned on individually - automated checkout typically misses vaporizer leaks
- O₂ failure alarm: test weekly by disconnecting O₂ hose; use a "tug test" daily (AAGBI/Baheti)
- The PAC should be in an ergonomically rational sequence and as short as possible without omitting critical items
- Dorsch & Dorsch (Understanding Anesthesia Equipment, 5e) is the classic reference for in-depth equipment checkout procedures and forms the basis of many institution-specific protocols, though the ASA 2008 guidelines are the current operative standard
Primary references: Miller's Anesthesia, 10e (Chapter 20, pp. 2400-2423); Barash's Clinical Anesthesia, 9e (Appendix B, pp. 2071-2086); Morgan & Mikhail's Clinical Anesthesiology, 7e (Table 4-3, pp. 146-148); Baheti DK et al., Understanding Anesthetic Equipment & Procedures, Appendices 1 & 2; Ravishankar M - PMC3821271
This is a shared conversation. Sign in to Orris to start your own chat.