make a presentation on the topic retinitis and choroiditis from standard textbook from basic to advanced level, also include from Ryan's retina include clinical trials and recent advances.
retinitis choroiditis treatment clinical trials
CMV retinitis treatment advances
toxoplasma retinochoroiditis uveitis treatment
retinitis pigmentosa gene therapy treatment advances
acute retinal necrosis viral retinitis herpes treatment
birdshot chorioretinopathy VKH vogt koyanagi harada treatment
Vogt Koyanagi Harada syndrome uveitis choroiditis treatment
sarcoidosis tuberculosis choroiditis uveitis posterior
ls /home/daytona/workspace/ 2>/dev/null || mkdir -p /home/daytona/workspace && e…
~/retinitis_choroiditis/build_pptx.js
const pptxgen = require("pptxgenjs");
const pres = new pptxgen();
pres.layout = 'LAYOUT_WIDE';
pres.title = 'Retinitis & Choroiditis: Basic to Advanced';
pres.author = 'Orris Medical AI';
// ─── COLOR PALETTE ───────────────────────────────────────────────
const DARK_BG = '0D1B2A'; // deep navy (dominant ~65%)
const MID_BG = '1B2E44'; // mid navy for section slides
const ACCENT1 = '2FBFDE'; // teal-blue accent
const ACCENT2 = 'E8A838'; // amber for highlights
const WHITE = 'F0F4F8';
const LIGHT_TXT = 'C9D8E6';
const PALE = 'E8F4FA';
const RED_ACC = 'E05A5A';
const GREEN_ACC = '4CAF7D';
// ─── MASTER HELPERS ──────────────────────────────────────────────
function addTitleSlide(pres, title, subtitle) {
const sl = pres.addSlide();
// gradient-style background via layered shapes
sl.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: '100%', h: '100%', fill: { color: DARK_BG } });
sl.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 0.4, h: '100%', fill: { color: ACCENT1 } });
sl.addShape(pres.ShapeType.rect, { x: 12.9, y: 0, w: 0.4, h: '100%', fill: { color: ACCENT2 } });
// Decorative circle
sl.addShape(pres.ShapeType.ellipse, { x: 8.5, y: -1.5, w: 5.5, h: 5.5, fill: { color: MID_BG }, line: { color: ACCENT1, width: 2 } });
sl.addText(title, {
x: 0.7, y: 1.8, w: 11.5, h: 1.8,
fontSize: 38, bold: true, color: WHITE, align: 'left',
fontFace: 'Calibri',
});
if (subtitle) {
sl.addText(subtitle, {
x: 0.7, y: 3.7, w: 10, h: 1,
fontSize: 18, color: ACCENT1, align: 'left', fontFace: 'Calibri',
});
}
sl.addText('Based on: Kanski\'s Clinical Ophthalmology 10e | Wills Eye Manual | Ryan\'s Retina | PubMed 2021-2026', {
x: 0.7, y: 6.5, w: 12, h: 0.4,
fontSize: 11, color: LIGHT_TXT, italic: true, align: 'left',
});
return sl;
}
function addSectionSlide(pres, sectionNo, title) {
const sl = pres.addSlide();
sl.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: '100%', h: '100%', fill: { color: MID_BG } });
sl.addShape(pres.ShapeType.rect, { x: 0, y: 2.5, w: '100%', h: 0.08, fill: { color: ACCENT1 } });
sl.addText(`Section ${sectionNo}`, {
x: 1, y: 1.2, w: 11, h: 0.8,
fontSize: 22, color: ACCENT2, bold: false, fontFace: 'Calibri',
});
sl.addText(title, {
x: 1, y: 2.0, w: 11, h: 1.5,
fontSize: 36, bold: true, color: WHITE, fontFace: 'Calibri',
});
return sl;
}
function addContentSlide(pres, title, bullets, note) {
const sl = pres.addSlide();
sl.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: '100%', h: '100%', fill: { color: DARK_BG } });
sl.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: '100%', h: 0.75, fill: { color: MID_BG } });
sl.addShape(pres.ShapeType.rect, { x: 0, y: 0.72, w: 1.2, h: 0.06, fill: { color: ACCENT1 } });
sl.addText(title, {
x: 0.25, y: 0.1, w: 12.8, h: 0.6,
fontSize: 22, bold: true, color: ACCENT1, fontFace: 'Calibri', valign: 'middle',
});
const items = bullets.map((b, i) => ({
text: b.text || b,
options: {
bullet: b.sub ? { indent: 30 } : { type: 'bullet', indent: 18 },
color: b.sub ? LIGHT_TXT : WHITE,
fontSize: b.sub ? 14 : 16,
bold: b.bold || false,
breakLine: true,
}
}));
if (items.length > 0) items[items.length - 1].options.breakLine = false;
sl.addText(items, {
x: 0.3, y: 0.9, w: 12.5, h: 5.8,
fontFace: 'Calibri', valign: 'top',
});
if (note) {
sl.addText(note, {
x: 0.3, y: 6.8, w: 12.5, h: 0.45,
fontSize: 11, color: ACCENT2, italic: true, fontFace: 'Calibri',
});
}
return sl;
}
function addTwoColSlide(pres, title, leftTitle, leftItems, rightTitle, rightItems, bgColor) {
const sl = pres.addSlide();
sl.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: '100%', h: '100%', fill: { color: bgColor || DARK_BG } });
sl.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: '100%', h: 0.75, fill: { color: MID_BG } });
sl.addShape(pres.ShapeType.rect, { x: 0, y: 0.72, w: 1.2, h: 0.06, fill: { color: ACCENT2 } });
sl.addText(title, { x: 0.25, y: 0.1, w: 12.8, h: 0.6, fontSize: 22, bold: true, color: ACCENT2, fontFace: 'Calibri', valign: 'middle' });
// Left col header
sl.addShape(pres.ShapeType.rect, { x: 0.25, y: 0.85, w: 6.0, h: 0.45, fill: { color: ACCENT1 }, rectRadius: 0.05 });
sl.addText(leftTitle, { x: 0.35, y: 0.88, w: 5.8, h: 0.38, fontSize: 15, bold: true, color: DARK_BG, fontFace: 'Calibri' });
const lItems = leftItems.map((b, i) => ({
text: b.text || b,
options: { bullet: true, color: b.highlight ? ACCENT2 : WHITE, fontSize: b.sub ? 13 : 15, bold: b.bold || false, breakLine: true }
}));
if (lItems.length) lItems[lItems.length-1].options.breakLine = false;
sl.addText(lItems, { x: 0.3, y: 1.4, w: 5.9, h: 5.3, fontFace: 'Calibri', valign: 'top' });
// Right col header
sl.addShape(pres.ShapeType.rect, { x: 6.7, y: 0.85, w: 6.0, h: 0.45, fill: { color: ACCENT2 }, rectRadius: 0.05 });
sl.addText(rightTitle, { x: 6.8, y: 0.88, w: 5.8, h: 0.38, fontSize: 15, bold: true, color: DARK_BG, fontFace: 'Calibri' });
const rItems = rightItems.map((b, i) => ({
text: b.text || b,
options: { bullet: true, color: b.highlight ? ACCENT1 : WHITE, fontSize: b.sub ? 13 : 15, bold: b.bold || false, breakLine: true }
}));
if (rItems.length) rItems[rItems.length-1].options.breakLine = false;
sl.addText(rItems, { x: 6.75, y: 1.4, w: 5.9, h: 5.3, fontFace: 'Calibri', valign: 'top' });
// Divider
sl.addShape(pres.ShapeType.line, { x: 6.55, y: 0.85, w: 0, h: 5.9, line: { color: ACCENT1, width: 1, dashType: 'dash' } });
return sl;
}
function addTableSlide(pres, title, headers, rows) {
const sl = pres.addSlide();
sl.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: '100%', h: '100%', fill: { color: DARK_BG } });
sl.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: '100%', h: 0.75, fill: { color: MID_BG } });
sl.addText(title, { x: 0.25, y: 0.1, w: 12.8, h: 0.6, fontSize: 22, bold: true, color: ACCENT1, fontFace: 'Calibri', valign: 'middle' });
const tableRows = [
headers.map(h => ({ text: h, options: { bold: true, color: DARK_BG, fill: ACCENT1, fontSize: 13, align: 'center' } })),
...rows.map((row, ri) => row.map(cell => ({
text: cell,
options: { color: ri % 2 === 0 ? WHITE : LIGHT_TXT, fill: ri % 2 === 0 ? '162030' : '1B2E44', fontSize: 12, align: 'left' }
})))
];
sl.addTable(tableRows, {
x: 0.25, y: 0.9, w: 12.8, h: 5.9,
border: { type: 'solid', pt: 0.5, color: ACCENT1 },
fontFace: 'Calibri',
});
return sl;
}
function addEvidenceSlide(pres, title, items) {
const sl = pres.addSlide();
sl.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: '100%', h: '100%', fill: { color: DARK_BG } });
sl.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: '100%', h: 0.75, fill: { color: '14241a' } });
sl.addShape(pres.ShapeType.rect, { x: 0, y: 0.72, w: 1.2, h: 0.06, fill: { color: GREEN_ACC } });
sl.addText(title, { x: 0.25, y: 0.1, w: 12.8, h: 0.6, fontSize: 22, bold: true, color: GREEN_ACC, fontFace: 'Calibri', valign: 'middle' });
items.forEach((item, i) => {
const yBase = 0.95 + i * 1.18;
if (yBase > 6.5) return;
sl.addShape(pres.ShapeType.rect, { x: 0.25, y: yBase, w: 12.5, h: 1.05, fill: { color: '162030' }, rectRadius: 0.08, line: { color: GREEN_ACC, width: 0.5 } });
sl.addText(item.label, { x: 0.4, y: yBase + 0.04, w: 3.5, h: 0.4, fontSize: 12, bold: true, color: ACCENT2, fontFace: 'Calibri' });
sl.addText(item.pmid || '', { x: 10.5, y: yBase + 0.04, w: 2.0, h: 0.4, fontSize: 10, color: GREEN_ACC, fontFace: 'Calibri', align: 'right' });
sl.addText(item.detail, { x: 0.4, y: yBase + 0.44, w: 12.1, h: 0.55, fontSize: 13, color: LIGHT_TXT, fontFace: 'Calibri', valign: 'top' });
});
return sl;
}
// ═══════════════════════════════════════════════════════════════════
// SLIDE 1 – TITLE
// ═══════════════════════════════════════════════════════════════════
addTitleSlide(pres,
'Retinitis & Choroiditis\nBasic to Advanced',
'Pathophysiology · Clinical Features · Diagnosis · Treatment · Recent Advances'
);
// ═══════════════════════════════════════════════════════════════════
// SLIDE 2 – TABLE OF CONTENTS
// ═══════════════════════════════════════════════════════════════════
addContentSlide(pres, 'Outline of Presentation', [
{ text: '1. Anatomy & Terminology', bold: true },
{ text: ' Retina, Choroid, Uvea – structural overview', sub: true },
{ text: '2. Classification of Retinitis & Choroiditis', bold: true },
{ text: ' Infectious vs non-infectious; choriocapillaritis vs stromal choroiditis', sub: true },
{ text: '3. Infectious Retinitis – Viral', bold: true },
{ text: ' CMV, Acute Retinal Necrosis, Progressive Outer Retinal Necrosis', sub: true },
{ text: '4. Infectious Retinitis – Parasitic & Fungal', bold: true },
{ text: ' Toxoplasma, Histoplasmosis, Candida, Pneumocystis, Cryptococcus', sub: true },
{ text: '5. Retinitis Pigmentosa & Inherited Dystrophies', bold: true },
{ text: '6. Infectious Choroiditis', bold: true },
{ text: ' TB, Syphilis, Ebola, HIV-related', sub: true },
{ text: '7. Non-Infectious (White Dot) Choroiditis Syndromes', bold: true },
{ text: ' MEWDS, APMPPE, Serpiginous, Birdshot, PIC, MFC, VKH', sub: true },
{ text: '8. Clinical Trials & Recent Advances (PubMed 2021-2026)', bold: true },
{ text: '9. Summary & Key Pearls', bold: true },
]);
// ═══════════════════════════════════════════════════════════════════
// SECTION 1
// ═══════════════════════════════════════════════════════════════════
addSectionSlide(pres, 1, 'Anatomy & Terminology');
addTwoColSlide(pres,
'Retina & Choroid – Structural Overview',
'Retina (10 layers)',
[
'Innermost layer of the eye – neural tissue',
'Retinal Pigment Epithelium (RPE): phagocytoses shed photoreceptor outer segments',
'Photoreceptors (rods & cones): transduction of light → neural signal',
'Müller cells, bipolar, ganglion cells form neural circuitry',
'Blood supply: inner retina from central retinal artery; outer retina (RPE + photoreceptors) from choriocapillaris',
'"Retinitis" = inflammation of retinal layers, often necrotising',
'Hallmarks: white/yellow patches, haemorrhages, vasculitis, vitritis',
],
'Choroid (3 layers)',
[
'Vascular coat between sclera and RPE',
'Layers: choriocapillaris (inner), Sattler\'s layer (medium vessels), Haller\'s layer (large vessels)',
'Richest blood supply in the body per unit area',
'"Choroiditis" = inflammation of choroid; may extend to RPE ("chorioretinitis")',
'ICG angiography is gold standard for choroidal imaging',
'OCTA reveals choriocapillaris flow voids in active choroiditis',
'Bruch\'s membrane separates RPE from choriocapillaris',
]
);
addContentSlide(pres, 'Key Definitions', [
{ text: 'Retinitis – focal or diffuse inflammation of the retina. Can be infectious (viral, parasitic, fungal, bacterial) or non-infectious.', bold: false },
{ text: 'Choroiditis – inflammation of the choroid. Classified by anatomical layer involved (choriocapillaritis vs stromal) and aetiology.', bold: false },
{ text: 'Chorioretinitis / Retinochoroiditis – combined inflammation; the dominant structure named first (e.g., toxoplasma retinochoroiditis = retina primary target).', bold: false },
{ text: 'Panuveitis – inflammation of all uveal layers + retina (e.g., Acute Retinal Necrosis, VKH disease).', bold: false },
{ text: 'White Dot Syndromes – heterogeneous group of idiopathic inflammatory conditions characterised by discrete white/yellow lesions at the level of the outer retina, RPE or choroid.', bold: false },
{ text: 'Immune Recovery Uveitis (IRU) – paradoxical worsening in CMV retinitis after ART-mediated immune reconstitution.', bold: false },
]);
// ═══════════════════════════════════════════════════════════════════
// SECTION 2
// ═══════════════════════════════════════════════════════════════════
addSectionSlide(pres, 2, 'Classification of Retinitis & Choroiditis');
addTableSlide(pres, 'ICG Angiographic Classification of Choroiditis (Kanski 10e)',
['Class', 'Subtype', 'Examples'],
[
['1A', 'Primary Choriocapillaritis\n(trigger unknown)', 'MEWDS, APMPPE, Serpiginous choroidopathy, MFC, PIC'],
['1B', 'Secondary Choriocapillaritis\n(pathogen triggers immune response)', 'Acute syphilitic posterior placoid chorioretinitis (ASPPC)\nTB-related serpiginous choroiditis'],
['2A', 'Primary Stromal Choroiditis\n(stroma is target)', 'Birdshot retinochoroidopathy (HLA-A29)\nVogt–Koyanagi–Harada disease\nSympathetic ophthalmia'],
['2B', 'Secondary Stromal Choroiditis\n(secondary to systemic inflammation)', 'Sarcoidosis\nTubercular chorioretinitis\nSyphilitic chorioretinitis'],
]
);
addTwoColSlide(pres,
'Classification of Retinitis',
'Infectious Retinitis',
[
{ text: 'Viral:', bold: true },
{ text: ' CMV retinitis (most common in AIDS)', sub: true },
{ text: ' Acute Retinal Necrosis (HSV/VZV)', sub: true },
{ text: ' PORN – Progressive Outer Retinal Necrosis (VZV)', sub: true },
{ text: ' Rubella, Measles/SSPE, West Nile, Ebola, Zika', sub: true },
{ text: 'Parasitic:', bold: true },
{ text: ' Toxoplasma retinochoroiditis (most common cause worldwide)', sub: true },
{ text: 'Fungal:', bold: true },
{ text: ' Candida, Histoplasma, Cryptococcus, Pneumocystis', sub: true },
{ text: 'Bacterial:', bold: true },
{ text: ' Syphilitic retinitis, TB retinitis', sub: true },
],
'Non-Infectious Retinitis',
[
{ text: 'Inherited Dystrophies:', bold: true },
{ text: ' Retinitis Pigmentosa (most common hereditary retinal degeneration)', sub: true },
{ text: ' Cone-rod dystrophy, Leber congenital amaurosis', sub: true },
{ text: 'Autoimmune / Inflammatory:', bold: true },
{ text: ' Birdshot retinochoroidopathy', sub: true },
{ text: ' Sarcoid retinitis', sub: true },
{ text: 'Paraneoplastic:', bold: true },
{ text: ' CAR (cancer-associated retinopathy)', sub: true },
{ text: 'Drug-induced:', bold: true },
{ text: ' Chloroquine/hydroxychloroquine maculopathy', sub: true },
{ text: ' Rifabutin-associated uveitis', sub: true },
]
);
// ═══════════════════════════════════════════════════════════════════
// SECTION 3 – VIRAL RETINITIS
// ═══════════════════════════════════════════════════════════════════
addSectionSlide(pres, 3, 'Infectious Retinitis – Viral');
addContentSlide(pres, 'CMV Retinitis – Introduction & Risk Factors',
[
{ text: 'Aetiology:', bold: true },
{ text: ' Cytomegalovirus (CMV) – member of Herpesviridae. Primary infection in immunocompetent is usually subclinical; retinitis from reactivation of latent virus in immunocompromised.', sub: true },
{ text: 'Epidemiology:', bold: true },
{ text: ' Most common opportunistic intraocular infection in AIDS (CD4+ <50 cells/µl is strongest risk factor).', sub: true },
{ text: ' Also occurs post-transplant, haematological malignancy, prolonged immunosuppression.', sub: true },
{ text: ' Incidence has fallen dramatically since introduction of HAART/ART, but prevalence remains high.', sub: true },
{ text: 'Risk associations:', bold: true },
{ text: ' HIV-related retinal microangiopathy (cotton-wool spots + haemorrhages) is a marker for increased CMV retinitis risk.', sub: true },
{ text: ' CD4+ <100 cells/µl: discontinue antiviral therapy when CD4+ reaches >100–150 cells/µl.', sub: true },
{ text: 'Without treatment, blindness is essentially inevitable.', bold: true },
],
'Kanski\'s Clinical Ophthalmology 10e, p.489 | Wills Eye Manual'
);
addTwoColSlide(pres,
'CMV Retinitis – Clinical Features',
'Presentation & Findings',
[
'Reduced vision (macular involvement) or floaters',
'"Pizza pie" or "Margherita pizza" appearance: dense white retinal infiltration + flame haemorrhages along vascular arcades',
'Two patterns: Fulminant (confluent, haemorrhagic) vs Indolent (granular, peripheral, less haemorrhagic)',
'One eye usually affected initially; progresses to both in 50% if untreated',
'Minimal vitritis in active phase (contrast with ARN)',
'Optic neuritis may result from direct spread',
'Frosted branch angiitis (FBA) in ~6%',
'Retinal detachment (RD) – major morbidity: up to 50% in advanced cases',
],
'Complications',
[
{ text: 'Immune Recovery Uveitis (IRU):', bold: true },
{ text: ' Paradoxical inflammation after ART-mediated immune reconstitution; residual viral antigen triggers vigorous immune response', sub: true },
{ text: ' Manifestations: severe vitritis, CMO, ERM, neovascularisation; can progress to phthisis', sub: true },
{ text: 'Retinal necrosis → RRD: irregular pigmentation, atrophy, retinal holes', sub: true },
{ text: 'Cataract (late stage)', sub: true },
{ text: 'CMV anterior uveitis (iridocyclitis): elevated IOP, corneal endotheliitis, sectoral iris atrophy in immunocompetent', sub: true },
]
);
addContentSlide(pres, 'CMV Retinitis – Diagnosis & Treatment',
[
{ text: 'Diagnosis:', bold: true },
{ text: ' Clinical appearance is usually pathognomonic in the correct context', sub: true },
{ text: ' Vitreous/aqueous PCR for CMV DNA (gold standard when in doubt)', sub: true },
{ text: ' CD4+ count and plasma HIV-RNA levels', sub: true },
{ text: 'Systemic Treatment:', bold: true },
{ text: ' ART (antiretroviral therapy) – mainstay of management; restores innate CMV suppression', sub: true },
{ text: ' IV Ganciclovir: 5 mg/kg BD × 2–3 weeks induction, then maintenance', sub: true },
{ text: ' Oral Valganciclovir: 900 mg BD induction, 900 mg OD maintenance – comparable efficacy to IV ganciclovir', sub: true },
{ text: ' Foscarnet, Cidofovir: for ganciclovir-resistant CMV', sub: true },
{ text: 'Intravitreal Treatment:', bold: true },
{ text: ' Ganciclovir 2 mg / Foscarnet 2.4 mg intravitreal injections for immediate macular-threatening disease', sub: true },
{ text: ' Ganciclovir intravitreal implant (Vitrasert) – sustained local delivery for up to 6–8 months', sub: true },
{ text: 'Retinal Detachment:', bold: true },
{ text: ' PPV + silicone oil is treatment of choice; laser demarcation for prophylaxis', sub: true },
],
'Kanski\'s Clinical Ophthalmology 10e, p.491'
);
addContentSlide(pres, 'Acute Retinal Necrosis (ARN)',
[
{ text: 'Definition:', bold: true },
{ text: ' Rare but devastating necrotising retinitis in otherwise healthy individuals', sub: true },
{ text: ' Cause: HSV-1/2 (younger patients) and VZV (older patients)', sub: true },
{ text: 'American Uveitis Society Diagnostic Criteria:', bold: true },
{ text: ' 1. One or more discrete foci of peripheral retinal necrosis (deep yellow-white infiltrates, well-defined borders)', sub: true },
{ text: ' 2. Circumferential spread in the absence of treatment', sub: true },
{ text: ' 3. Occlusive retinal vasculitis including arteritis', sub: true },
{ text: ' 4. Prominent anterior uveitis + vitritis (panuveitis)', sub: true },
{ text: ' 5. Rapid progression without treatment', sub: true },
{ text: 'Prognosis:', bold: true },
{ text: ' >50% achieve only 6/60 due to retinal/optic nerve ischaemia or rhegmatogenous retinal detachment (RRD)', sub: true },
{ text: 'Treatment:', bold: true },
{ text: ' IV Aciclovir 15 mg/kg every 8 h for 10–14 days → Oral aciclovir 800 mg 5× daily for 6–12 weeks', sub: true },
{ text: ' Oral Valaciclovir / Famciclovir as alternative oral agents', sub: true },
{ text: ' Intravitreal Ganciclovir or Foscarnet as adjunct', sub: true },
{ text: ' Prophylactic laser photocoagulation posterior to lesions reduces RD risk', sub: true },
{ text: ' PPV + silicone oil for established RRD', sub: true },
],
'Kanski\'s Clinical Ophthalmology 10e, p.492'
);
addTwoColSlide(pres,
'Progressive Outer Retinal Necrosis (PORN) vs ARN',
'ARN (Acute Retinal Necrosis)',
[
{ text: 'Patients: immunocompetent', bold: true },
'Cause: HSV (young), VZV (old)',
'Location: Peripheral, circumferential spread',
'Vitritis: Prominent (panuveitis)',
'Vasculitis: Occlusive arteritis – prominent',
'Haemorrhage: Common',
'Progression: Rapid without treatment',
{ text: 'Treatment: IV Aciclovir → oral', bold: false },
'RD risk: Up to 75% without prophylaxis',
{ text: 'PCR: Aqueous/vitreous for HSV/VZV DNA', bold: false },
],
'PORN (Progressive Outer Retinal Necrosis)',
[
{ text: 'Patients: Severely immunocompromised (CD4+ <10)', bold: true, highlight: true },
'Cause: VZV predominantly',
'Location: Multifocal, outer retina, posterior pole early',
'Vitritis: Absent or minimal',
'Vasculitis: Absent',
'Haemorrhage: Less common',
'Progression: Extremely rapid',
{ text: 'Treatment: IV Ganciclovir + Foscarnet (combination)', bold: false, highlight: true },
'RD risk: Nearly 70% within weeks',
{ text: 'Prognosis: Very poor; bilateral in >70%', bold: false, highlight: true },
]
);
// ═══════════════════════════════════════════════════════════════════
// SECTION 4 – PARASITIC & FUNGAL
// ═══════════════════════════════════════════════════════════════════
addSectionSlide(pres, 4, 'Infectious Retinitis – Parasitic & Fungal');
addContentSlide(pres, 'Toxoplasma Retinochoroiditis',
[
{ text: 'Aetiology:', bold: true },
{ text: ' Most common cause of posterior uveitis worldwide', sub: true },
{ text: ' Toxoplasma gondii (obligate intracellular protozoan); acquired by ingestion of oocysts or undercooked meat', sub: true },
{ text: ' Most ocular toxoplasmosis is reactivation of congenital infection', sub: true },
{ text: 'Classic Clinical Features:', bold: true },
{ text: ' "Headlight in the fog" – focal white fluffy retinitis adjacent to an old pigmented chorioretinal scar', sub: true },
{ text: ' Dense overlying vitritis (vitreous cells and haze)', sub: true },
{ text: ' Unilateral in 80%; may be bilateral in congenital or immunocompromised forms', sub: true },
{ text: ' In AIDS: atypical – multiple lesions, absent scar, no overlying vitritis ("pizza pie" mimicking CMV)', sub: true },
{ text: 'Diagnosis:', bold: true },
{ text: ' Clinical diagnosis in typical cases; supported by Sabin-Feldman dye test, IgG/IgM titres', sub: true },
{ text: ' Aqueous PCR (Toxoplasma DNA) when in doubt or atypical', sub: true },
{ text: 'Treatment:', bold: true },
{ text: ' Gold standard: Pyrimethamine 100 mg loading → 25 mg OD + Sulfadiazine 1g QID + Folinic acid + Steroids', sub: true },
{ text: ' Alternatives: Trimethoprim-Sulfamethoxazole (TMP-SMX), Clindamycin, Azithromycin, Atovaquone', sub: true },
{ text: ' Treat for 4–6 weeks; prophylaxis with low-dose TMP-SMX in immunocompromised', sub: true },
],
'Kanski\'s Clinical Ophthalmology 10e; PMID 34370174'
);
addContentSlide(pres, 'Fungal Choroiditis / Chorioretinitis',
[
{ text: 'Presumed Ocular Histoplasmosis Syndrome (POHS):', bold: true },
{ text: ' Triad: (1) Multiple white atrophic chorioretinal "histo spots" ~200µm; (2) Peripapillary atrophy; (3) Absence of vitritis', sub: true },
{ text: ' Endemic in Mississippi River Valley, USA; immune-mediated, not direct infection in most cases', sub: true },
{ text: ' Complication: Macular neovascularisation (MNV/CNV) → anti-VEGF treatment', sub: true },
{ text: 'Pneumocystis Choroiditis (AIDS):', bold: true },
{ text: ' Multiple pale choroidal lesions with yellow hue, no vitritis; bilateral; often asymptomatic', sub: true },
{ text: ' Occurs when <100 CD4+ cells and without TMP-SMX prophylaxis', sub: true },
{ text: ' Treatment: IV Pentamidine or TMP-SMX', sub: true },
{ text: 'Cryptococcus Choroiditis (AIDS):', bold: true },
{ text: ' Multiple choroidal lesions; often with CNS cryptococcal meningitis; severe disc swelling', sub: true },
{ text: ' Treatment: Amphotericin B + Flucytosine, then Fluconazole maintenance', sub: true },
{ text: 'Candida Chorioretinitis:', bold: true },
{ text: ' Fluffy white "string of pearls" vitreous infiltrate; classic in IV drug users, TPN patients', sub: true },
{ text: ' Treatment: Fluconazole (systemic) ± intravitreal Amphotericin B / Voriconazole', sub: true },
],
'Kanski\'s Clinical Ophthalmology 10e, pp.400-403'
);
// ═══════════════════════════════════════════════════════════════════
// SECTION 5 – RETINITIS PIGMENTOSA
// ═══════════════════════════════════════════════════════════════════
addSectionSlide(pres, 5, 'Retinitis Pigmentosa & Inherited Dystrophies');
addContentSlide(pres, 'Retinitis Pigmentosa (RP) – Overview',
[
{ text: 'Definition:', bold: true },
{ text: ' Clinically and genetically diverse group of inherited diffuse retinal degenerations; initially affects rod photoreceptors, then cones and RPE', sub: true },
{ text: 'Epidemiology:', bold: true },
{ text: ' Most common hereditary retinal degeneration: prevalence 1:3,000–1:5,000', sub: true },
{ text: 'Inheritance Patterns:', bold: true },
{ text: ' Autosomal Dominant (AD): mutations in Rhodopsin gene (most common cause of AD-RP); PRPF31, PRPF3, ROM1', sub: true },
{ text: ' Autosomal Recessive (AR): ABCA4, RPGR, CNGB1, USH2A', sub: true },
{ text: ' X-linked: RPGR gene mutation (90% of XL cases) – most severe form', sub: true },
{ text: ' Sporadic: ~40% of cases; may be any pattern', sub: true },
{ text: 'Syndromic RP (20–30% of cases):', bold: true },
{ text: ' Usher syndrome (RP + sensorineural deafness) – most common cause', sub: true },
{ text: ' Bardet-Biedl syndrome, Refsum disease, Kearns-Sayre (mitochondrial)', sub: true },
{ text: ' Leber Congenital Amaurosis: severe early-onset RP variant (~5%)', sub: true },
{ text: 'Pathogenesis:', bold: true },
{ text: ' Affected genes encode: phototransduction cascade, retinoid cycle, photoreceptor structural proteins, RPE function', sub: true },
{ text: ' ~100+ gene loci identified; ~50% of patients still lack known mutation', sub: true },
],
'Kanski\'s Clinical Ophthalmology 10e, p.646'
);
addTwoColSlide(pres,
'Retinitis Pigmentosa – Clinical Features & Management',
'Clinical Features',
[
{ text: 'Classic Triad:', bold: true },
{ text: ' Bone-spicule pigmentation (mid-peripheral, perivascular)', sub: true },
{ text: ' Arteriolar attenuation', sub: true },
{ text: ' Waxy disc pallor', sub: true },
{ text: 'Symptoms:', bold: true },
{ text: ' Nyctalopia / dark adaptation difficulty (earliest symptom)', sub: true },
{ text: ' Peripheral visual field constriction ("tunnel vision")', sub: true },
{ text: ' Photopsia, reduced contrast sensitivity', sub: true },
{ text: 'Associated features: CMO (cystoid macular oedema) in ~20%, posterior subcapsular cataract, myopia, keratoconus', sub: true },
{ text: 'Investigations:', bold: true },
{ text: ' ERG: severely reduced or extinguished rod response (pathognomonic)', sub: true },
{ text: ' Goldman visual fields, FAF (RPE atrophy), OCT (photoreceptor loss)', sub: true },
{ text: ' Genetic testing: important for counselling and eligibility for gene therapy', sub: true },
],
'Treatment & Emerging Therapies',
[
{ text: 'No cure currently, but multiple emerging treatments:', bold: true },
{ text: 'Vitamin A palmitate 15,000 IU/day: may slow progression (CATT study)', sub: true },
{ text: 'Low-vision aids, protective spectacles (UV/blue light)', sub: true },
{ text: 'Carbonic anhydrase inhibitors (Acetazolamide/Dorzolamide) for CMO', sub: true },
{ text: 'Gene Therapy:', bold: true, highlight: true },
{ text: ' Voretigene neparvovec (Luxturna): FDA/EMA approved 2017/2018 for RPE65-associated RP (biallelic mutations) – landmark first approved ocular gene therapy', sub: true },
{ text: 'Retinal Implants:', bold: true },
{ text: ' Argus II epiretinal implant (Second Sight): approved for severe RP', sub: true },
{ text: 'Stem Cell Therapy:', bold: true },
{ text: ' Under investigation; multiple Phase I/II trials (PMID 37798796)', sub: true },
{ text: 'Optogenetics & neuroprotection: emerging', sub: true },
]
);
// ═══════════════════════════════════════════════════════════════════
// SECTION 6 – INFECTIOUS CHOROIDITIS
// ═══════════════════════════════════════════════════════════════════
addSectionSlide(pres, 6, 'Infectious Choroiditis');
addContentSlide(pres, 'Tubercular & Syphilitic Chorioretinitis',
[
{ text: 'Tubercular Chorioretinitis:', bold: true },
{ text: ' Caused by Mycobacterium tuberculosis (haematogenous dissemination)', sub: true },
{ text: ' Classic: small choroidal granulomas (2nd frequency feature after uveitis)', sub: true },
{ text: ' TB serpiginous choroiditis: geographic, serpiginous chorioretinal scars mimicking idiopathic serpiginous', sub: true },
{ text: ' Eales disease: retinal periphlebitis + neovascularisation in young Asian men (TB association)', sub: true },
{ text: ' Diagnosis: Mantoux/TST, IGRA (Quantiferon Gold), CXR; aqueous PCR for M. tuberculosis', sub: true },
{ text: ' Treatment: Standard 4-drug ATT (HRZE × 2 months → HR × 4–10 months) + oral corticosteroids', sub: true },
{ text: 'Syphilitic Chorioretinitis:', bold: true },
{ text: ' Treponema pallidum; the "Great Imitator" – can mimic any uveitis pattern', sub: true },
{ text: ' Acute syphilitic posterior placoid chorioretinitis (ASPPC): single large yellow-orange placoid foveal lesion; associated with HIV co-infection', sub: true },
{ text: ' Necrotising retinitis, vitritis, optic neuritis, panuveitis all possible', sub: true },
{ text: ' Diagnosis: VDRL/RPR (screening) + TPHA/FTA-ABS (confirmatory); LP if neurological involvement', sub: true },
{ text: ' Treatment: IV Benzylpenicillin G 18-24 MU/day × 10-14 days (neurosyphilis protocol)', sub: true },
],
'Kanski\'s Clinical Ophthalmology 10e'
);
addContentSlide(pres, 'Sarcoidosis & HIV-Related Ocular Inflammation',
[
{ text: 'Sarcoidosis Uveitis/Choroiditis:', bold: true },
{ text: ' Multisystem granulomatous disease; ocular involvement in 25–50% (can be presenting feature)', sub: true },
{ text: ' Posterior: retinal periphlebitis ("candle wax drippings"), choroidal granulomas, CMO, disc oedema', sub: true },
{ text: ' Choroidal granulomas appear as pale yellow nodules; can mimic metastatic disease', sub: true },
{ text: ' Diagnosis: Elevated ACE & lysozyme, CXR/HRCT chest (bilateral hilar LAP), biopsy (non-caseating granulomas)', sub: true },
{ text: ' Treatment: Systemic corticosteroids as first-line; methotrexate, mycophenolate mofetil for steroid-sparing; infliximab for refractory cases', sub: true },
{ text: 'HIV-Related Ocular Disease:', bold: true },
{ text: ' HIV Microangiopathy: retinal cotton-wool spots + haemorrhages; most frequent retinopathy in AIDS (up to 70%)', sub: true },
{ text: ' Associated with declining CD4+ count – marker for increased CMV retinitis risk', sub: true },
{ text: ' Lesions disappear spontaneously; treatment is ART', sub: true },
{ text: ' Kaposi sarcoma (eyelid, conjunctiva), B-cell lymphoma (orbit), opportunistic infections are part of the AIDS ocular spectrum', sub: true },
],
'Kanski\'s Clinical Ophthalmology 10e; PMID 37176633'
);
// ═══════════════════════════════════════════════════════════════════
// SECTION 7 – WHITE DOT SYNDROMES / NON-INFECTIOUS CHOROIDITIS
// ═══════════════════════════════════════════════════════════════════
addSectionSlide(pres, 7, 'Non-Infectious (White Dot) Choroiditis Syndromes');
addContentSlide(pres, 'MEWDS & APMPPE',
[
{ text: 'Multiple Evanescent White Dot Syndrome (MEWDS):', bold: true },
{ text: ' Uncommon idiopathic; acute onset; typically young adult females', sub: true },
{ text: ' 25–50% report preceding viral illness; influenza vaccination occasionally implicated', sub: true },
{ text: ' Clinical: painless monocular blurring (6/9–6/60), photopsia, scotomas; subtle posterior vitritis in 50%', sub: true },
{ text: ' Fundus: 100–300 µm ill-defined grey-white patches sparing the fovea; "orange granular fovea" (pathognomonic)', sub: true },
{ text: ' Multimodal imaging: FAF shows hyperAF dots (key diagnostic tool); ICG shows hypofluorescent dots; OCT shows IS/OS disruption', sub: true },
{ text: ' Spontaneous recovery over weeks; 10% recur → suspect MFC if recurrent', sub: true },
{ text: ' No treatment required', sub: true },
{ text: 'Acute Posterior Multifocal Placoid Pigment Epitheliopathy (APMPPE):', bold: true },
{ text: ' Young adults; bilateral; often follows viral illness (immune-mediated choriocapillaritis)', sub: true },
{ text: ' Multiple cream-coloured placoid lesions at RPE level in posterior pole', sub: true },
{ text: ' FA: early hypofluorescence → late hyperfluorescence (classic pattern)', sub: true },
{ text: ' Usually self-limited; rare CNS vasculitis association (cerebral ischaemia – urgent investigation)', sub: true },
{ text: ' Steroids if CNS involvement or persistent/recurrent', sub: true },
],
'Kanski\'s Clinical Ophthalmology 10e, pp.508-510'
);
addContentSlide(pres, 'Serpiginous Choroidopathy',
[
{ text: 'Definition:', bold: true },
{ text: ' Rare, chronic, progressive choroiditis of unknown aetiology; primarily affecting choriocapillaris', sub: true },
{ text: 'Demographics:', bold: true },
{ text: ' Middle-aged adults; no sex predilection; bilateral (often asymmetric)', sub: true },
{ text: 'Clinical Features:', bold: true },
{ text: ' Active lesions: grey-white subretinal infiltrates with pseudopod-like ("snake-like") extensions from prior scarred areas', sub: true },
{ text: ' Lesions extend centrifugally, commonly around the disc and macula', sub: true },
{ text: ' Inactive lesions: chorioretinal scarring with sharp borders, pigment disturbance', sub: true },
{ text: ' Visual loss when fovea involved (may be sudden); CMO can occur', sub: true },
{ text: 'Imaging:', bold: true },
{ text: ' FA: early hypofluorescence → late hyperfluorescence in active disease', sub: true },
{ text: ' FAF: hyperautofluorescence at active edge (key for monitoring)', sub: true },
{ text: ' ICGA: marked hypofluorescence throughout all phases', sub: true },
{ text: ' OCTA: flow void at choriocapillaris level', sub: true },
{ text: 'Treatment:', bold: true },
{ text: ' Oral/IV steroids; immunosuppressives (azathioprine, mycophenolate, cyclosporine, tacrolimus); infliximab', sub: true },
{ text: ' Important DDx: TB-related serpiginous choroiditis (treat with ATT first!)', sub: true },
],
'Kanski\'s Clinical Ophthalmology 10e, p.510'
);
addContentSlide(pres, 'Birdshot Retinochoroidopathy',
[
{ text: 'Definition:', bold: true },
{ text: ' Uncommon idiopathic chronic bilateral inflammatory disease; severe retinitis + stromal choroiditis as independent events', sub: true },
{ text: 'Demographics:', bold: true },
{ text: ' Middle-aged women; HLA-A29 positive in >95% (vs 7% general population)', sub: true },
{ text: 'Clinical Features:', bold: true },
{ text: ' Insidious impairment of central vision + floaters, nyctalopia, dyschromatopsia, photopsia', sub: true },
{ text: ' Bilateral vitritis', sub: true },
{ text: ' Multiple ill-defined ovoid cream-coloured choroidal patches (<1DD), postero-pole and midperiphery, radiating from disc', sub: true },
{ text: ' CMO, epiretinal membrane, macular neovascularisation (MNV) can develop', sub: true },
{ text: 'Investigations:', bold: true },
{ text: ' HLA-A29: >95% positive (essential test)', sub: true },
{ text: ' FA: extensive vascular leakage; diffuse macular oedema (fovea often spared)', sub: true },
{ text: ' ICGA: more numerous hypofluorescent lesions than clinically apparent', sub: true },
{ text: ' ERG and visual fields for monitoring', sub: true },
{ text: 'Prognosis:', bold: true },
{ text: ' ~1/3 achieve final VA <6/60; improving with aggressive sustained immunomodulatory therapy', sub: true },
{ text: 'Treatment:', bold: true },
{ text: ' Oral corticosteroids, periocular/intravitreal steroids; systemic immunosuppressives (mycophenolate, cyclosporine); biologics (infliximab, daclizumab)', sub: true },
],
'Kanski\'s Clinical Ophthalmology 10e, p.513'
);
addTwoColSlide(pres,
'Vogt–Koyanagi–Harada (VKH) Disease',
'Clinical Features & Diagnosis',
[
{ text: 'Multisystem granulomatous autoimmune disease attacking melanocyte-containing tissues', bold: false },
{ text: 'Demographics:', bold: true },
{ text: ' Asian, Hispanic, Middle Eastern individuals; women > men; HLA-DR4 association', sub: true },
{ text: 'Four Stages:', bold: true },
{ text: ' 1. Prodromal: meningism, fever, tinnitus, hearing loss, alopecia, vitiligo, poliosis', sub: true },
{ text: ' 2. Uveitic: bilateral granulomatous panuveitis, multiple serous retinal detachments, disc oedema', sub: true },
{ text: ' 3. Convalescent: sunset glow fundus (diffuse RPE depigmentation), Dalen-Fuchs nodules', sub: true },
{ text: ' 4. Chronic recurrent: bilateral granulomatous AU, secondary glaucoma, CNV', sub: true },
{ text: 'Diagnosis: Revised International Criteria (2001)', bold: true },
{ text: ' No preceding penetrating ocular trauma/surgery; no other cause identified; bilateral ocular involvement + ≥2/4 neurological/auditory/integumentary criteria', sub: true },
{ text: 'OCTA/ICG: Reveals choroidal thickening, stromal hypofluorescence, flow voids', sub: true },
],
'Treatment',
[
{ text: 'High-dose systemic corticosteroids:', bold: true, highlight: true },
{ text: ' IV methylprednisolone 1g/day × 3 days → oral prednisolone 1 mg/kg/day taper over ≥6 months', sub: true },
{ text: 'Early aggressive treatment reduces chronic disease sequelae', sub: true },
{ text: 'Steroid-sparing immunomodulatory therapy:', bold: true },
{ text: ' Azathioprine, mycophenolate mofetil, cyclosporine', sub: true },
{ text: ' Infliximab / adalimumab for refractory cases', sub: true },
{ text: 'Complications to manage:', bold: true },
{ text: ' Secondary glaucoma: medical/surgical', sub: true },
{ text: ' Cataract extraction (post-inflammation)', sub: true },
{ text: ' CNV: Anti-VEGF therapy', sub: true },
{ text: 'Recent OCTA meta-analysis (PMID 38456233):', bold: false },
{ text: ' Confirms choroidal flow voids as reliable marker for disease activity and treatment response monitoring', sub: true, highlight: true },
]
);
addContentSlide(pres, 'Other White Dot Syndromes',
[
{ text: 'Punctate Inner Choroidopathy (PIC):', bold: true },
{ text: ' Young, highly myopic women; small punched-out lesions at inner choroid; NO vitritis (distinguishes from MFC)', sub: true },
{ text: ' Complications: CNV in 40–75%; anti-VEGF therapy effective', sub: true },
{ text: 'Multifocal Choroiditis (MFC):', bold: true },
{ text: ' Similar to PIC but with anterior segment activity, vitritis (50–75%) and more lesions', sub: true },
{ text: ' Lesions: punched-out chorioretinal scars (50–350 µm) in posterior pole + periphery', sub: true },
{ text: ' CNV complication; consider steroid therapy for active inflammation', sub: true },
{ text: 'Sympathetic Ophthalmia (SO):', bold: true },
{ text: ' Bilateral granulomatous panuveitis following penetrating trauma or intraocular surgery to fellow eye', sub: true },
{ text: ' Latency: 90% within 1 year (peak: 4–8 weeks); rarely occurs decades later', sub: true },
{ text: ' Treatment: High-dose systemic steroids ± immunosuppressives; evisceration of the exciting eye within 2 weeks may prevent SO but NOT thereafter', sub: true },
{ text: 'Relentless Placoid Chorioretinitis (RPC / Ampiginous Choroiditis):', bold: true },
{ text: ' Hybrid of APMPPE + serpiginous; hundreds of lesions anterior and posterior to equator; chronic, relentless progression', sub: true },
{ text: ' Progressive Subretinal Fibrosis & Uveitis (SFU):', bold: true },
{ text: ' Myopic young women; subretinal fibrosis → poor visual prognosis; may be spectrum with MFC/PIC', sub: true },
],
'Kanski\'s Clinical Ophthalmology 10e, pp.508-517'
);
// ═══════════════════════════════════════════════════════════════════
// SECTION 8 – CLINICAL TRIALS & RECENT ADVANCES
// ═══════════════════════════════════════════════════════════════════
addSectionSlide(pres, 8, 'Clinical Trials & Recent Advances\n(PubMed 2021–2026)');
addEvidenceSlide(pres, 'Recent Evidence – CMV Retinitis & Viral Retinitis',
[
{
label: 'CMV Retinitis – Antiviral Therapy Meta-Analysis (2025)',
pmid: 'PMID 39549781',
detail: 'Systematic review/meta-analysis in Surv Ophthalmol (Putera et al., 2025): Oral valganciclovir equivalent to IV ganciclovir for induction in AIDS-related CMV retinitis; intravitreal therapy provides faster local response but must be combined with systemic ART.',
},
{
label: 'Antiviral Treatment for ARN – Systematic Review (2024)',
pmid: 'PMID 37774799',
detail: 'Meta-analysis in Surv Ophthalmol (Putera et al., 2024): IV aciclovir followed by oral antiviral remains standard. Intravitreal ganciclovir/foscarnet as adjunct improves outcomes. Combination prophylactic laser reduces RD incidence.',
},
{
label: 'Viral Retinitis Diagnostics – Advances in Microbiological Diagnosis (2022)',
pmid: 'PMID 38983563',
detail: 'Review in Front Ophthalmol (Gueudry & Bodaghi, 2022): Real-time PCR of aqueous/vitreous has transformed diagnosis of herpetic retinitis. Metagenomic next-generation sequencing (mNGS) emerging for refractory/atypical cases.',
},
{
label: 'Corticosteroids & Immunomodulation in Infectious Uveitis (2024)',
pmid: 'PMID 38330155',
detail: 'Review (Akhavanrezayat et al., 2024): Careful adjunctive steroid use in viral and parasitic retinitis; steroids contraindicated as monotherapy but improve outcomes in CMV-IRU, toxoplasma retinochoroiditis, and TB uveitis when combined with targeted antimicrobials.',
},
{
label: 'Ocular Pathogen Resistance – Emerging Challenges (2025)',
pmid: 'PMID 41599633',
detail: 'Review in Pharmaceuticals (Ather & Conrady, 2025): Ganciclovir-resistant CMV increasing (UL97, UL54 mutations). New agents: Letermovir and Maribavir under investigation for drug-resistant CMV retinitis.',
},
]
);
addEvidenceSlide(pres, 'Recent Evidence – Choroiditis & Uveitis Advances',
[
{
label: 'VKH – OCTA for Disease Monitoring (Systematic Review 2024)',
pmid: 'PMID 38456233',
detail: 'Systematic review/meta-analysis (Liang et al., 2024): OCTA reliably quantifies choriocapillaris flow voids in VKH. Abnormal OCTA findings persist even in "quiet" VKH, suggesting subclinical activity – important for treatment decisions.',
},
{
label: 'Sarcoidosis-Related Uveitis – Review (2023)',
pmid: 'PMID 37176633',
detail: 'Review in J Clin Med (Giorgiutti et al., 2023): Infliximab effective as steroid-sparing for sarcoid uveitis. New biologics (secukinumab, tocilizumab) in trials. ACE still useful but not specific. Whole-body PET-CT superior for staging.',
},
{
label: 'VKH Disease – Multimodal Imaging Review (2026)',
pmid: 'PMID 41644040',
detail: 'State-of-the-art review in Prog Retin Eye Res (Xia et al., 2026): Comprehensive multimodal imaging including widefield OCTA, enhanced depth OCT (EDI-OCT), and en face imaging now recommended for staging and monitoring VKH. Subclinical choroidal changes detected before clinical recurrence.',
},
{
label: 'Posterior Uveitis Management – Practical Tips for Retina Specialists (2023)',
pmid: 'PMID 37589912',
detail: 'Review (Paez-Escamilla et al., 2023): Step-up immunosuppression approach validated; systemic biologics (adalimumab – Humira, approved for uveitis) reduce steroid burden and relapses in non-infectious posterior uveitis including choroiditis syndromes.',
},
{
label: 'Advanced Multimodal Imaging in Granulomatous Uveitis (2026)',
pmid: 'PMID 42279083',
detail: 'Review in J Clin Med (Capobianco et al., 2026): Ultra-widefield FA, OCTA, and AI-assisted image analysis improving differential diagnosis between TB, sarcoid, and idiopathic choroiditis.',
},
]
);
addEvidenceSlide(pres, 'Recent Evidence – Retinitis Pigmentosa & Inherited Retinal Diseases',
[
{
label: 'Voretigene Neparvovec (Luxturna) Gene Therapy – Long-term Data',
pmid: 'PMID 34839010',
detail: 'Schneider et al. (Prog Retin Eye Res, 2022): Multi-year follow-up confirms durable vision improvement with voretigene in RPE65-deficiency. Bilateral subretinal injection preferred; immunosuppression protocol important to prevent immune rejection.',
},
{
label: 'Genetic Therapies for RP – Current Breakthroughs (2025)',
pmid: 'PMID 40869487',
detail: 'Pniakowska et al. (J Clin Med, 2025): Active gene therapy trials for >10 RP-causing genes (RPGR, CNGB3, PDE6A, CNGA3). Antisense oligonucleotides (ASOs) for PRPF31. Optogenetics (channelrhodopsin AAV vectors) in Phase I/II trials for end-stage RP.',
},
{
label: 'Stem Cell Therapy for Inherited Retinal Disease – Meta-Analysis (2023)',
pmid: 'PMID 37798796',
detail: 'Systematic review/meta-analysis in Stem Cell Res Ther (Chen et al., 2023): Subretinal RPE stem cell transplantation shows early safety signals in Phase I/II trials for RP and Stargardt; 12-month visual acuity improvements in some patients. Further Phase III trials needed.',
},
{
label: 'TUDCA Neuroprotection in Retinal Disorders (2024)',
pmid: 'PMID 37691227',
detail: 'Systematic review (Li et al., Curr Neuropharmacol, 2024): Tauroursodeoxycholic acid (TUDCA) exerts neuroprotective effects in RP models; Phase II trials underway. Mechanism: ER stress reduction, anti-apoptotic effects on photoreceptors.',
},
{
label: 'Ocular Toxoplasmosis SS-OCT Biomarkers (2026)',
pmid: 'PMID 42096258',
detail: 'Sree Keerti et al. (Ocul Immunol Inflamm, 2026): Swept-source OCT reveals choroidal thickness and structural retinal changes as objective biomarkers for disease activity and treatment monitoring in toxoplasmic retinochoroiditis.',
},
]
);
// ═══════════════════════════════════════════════════════════════════
// SLIDE – RYAN'S RETINA HIGHLIGHTS
// ═══════════════════════════════════════════════════════════════════
addContentSlide(pres, "Ryan's Retina – Key Concepts & Clinical Pearls",
[
{ text: 'CMV Retinitis (Ryan\'s Retina, Chapter on AIDS & Retina):', bold: true },
{ text: ' Ganciclovir-resistant CMV retinitis: mutations in UL97 (kinase, ~90%) or UL54 (polymerase, ~10%); switch to Foscarnet or Cidofovir; emerging agent: Letermovir', sub: true },
{ text: ' Ganciclovir intravitreal implant (Vitrasert, 4.5 mg): superior local disease control but NO protection for fellow eye – must combine with systemic valganciclovir', sub: true },
{ text: 'Toxoplasma Retinochoroiditis (Ryan\'s Retina):', bold: true },
{ text: ' TOXO Study (Brazil): long-term TMP-SMX prophylaxis reduces recurrence rate by ~75% in high-risk patients (immunosuppressed, large lesions, near disc/macula)', sub: true },
{ text: ' Intravitreal clindamycin (1 mg) + dexamethasone (400 µg) – effective alternative when systemic therapy not tolerated (Level II evidence)', sub: true },
{ text: 'ARN – Prophylactic Laser (Ryan\'s Retina):', bold: true },
{ text: ' 360° laser retinopexy applied posterior to active lesions reduces risk of RD from ~75% to ~35%', sub: true },
{ text: ' PPV with endolaser + silicone oil tamponade is the standard surgical approach for established RRD in ARN', sub: true },
{ text: 'Birdshot Retinochoroidopathy – Adalimumab Trial:', bold: true },
{ text: ' MEAD trial data: adalimumab (anti-TNF) reduces systemic corticosteroid requirement and maintains ERG responses in birdshot; now part of step-up algorithm', sub: true },
{ text: 'Sympathetic Ophthalmia (Ryan\'s Retina):', bold: true },
{ text: ' Evisceration within 2 weeks of inciting injury may prevent SO; after SO is established, enucleation does NOT improve outcome of the fellow eye', sub: true },
],
"Ryan's Retina (6e) – Schachat et al."
);
// ═══════════════════════════════════════════════════════════════════
// SECTION 9 – SUMMARY
// ═══════════════════════════════════════════════════════════════════
addSectionSlide(pres, 9, 'Summary & Key Pearls');
addTableSlide(pres, 'Quick Differential Diagnosis at a Glance',
['Condition', 'Vitritis', 'Location', 'Key Feature', 'Treatment'],
[
['CMV Retinitis', 'Mild', 'Peripheral → central', '"Pizza pie" + haemorrhages', 'Valganciclovir + ART'],
['ARN', 'Severe', 'Peripheral → posterior', 'Panuveitis; occlusive vasculitis', 'IV Aciclovir → oral'],
['PORN', 'Absent', 'Outer retina; multifocal', 'Very rapid; immunocompromised', 'IV Ganciclovir + Foscarnet'],
['Toxoplasma', 'Dense', 'Adjacent to old scar', '"Headlight in fog"', 'Pyrimethamine + Sulfa'],
['Sarcoid', 'Present', 'Periphlebitis', 'Candle-wax drippings', 'Steroids ± immunosuppressives'],
['MEWDS', 'Mild', 'Outer retina, posterior', 'Orange granular fovea; spontaneous resolution', 'Observation'],
['APMPPE', 'Mild', 'RPE, posterior pole', 'Early hypofluorescence FA', 'Observation (± steroids)'],
['Birdshot', 'Present', 'Choroid, posterior', 'HLA-A29+; cream ovoid lesions', 'Immunosuppressives'],
['VKH', 'Present', 'Pan-uveal + systemic', 'Sunset glow; serous RD; poliosis', 'High-dose steroids'],
['Serpiginous', 'Absent', 'RPE/choriocapillaris', 'Jigsaw snake-like progression', 'Immunosuppressives; rule out TB'],
['RP (Inherited)', 'Absent', 'Mid-peripheral', 'Bone spicule + waxy disc', 'Gene therapy (RPE65); VA: Luxturna'],
]
);
addContentSlide(pres, 'Key Clinical Pearls',
[
{ text: 'CMV retinitis is the most common cause of infectious retinitis in AIDS; CD4+ <50 is the strongest risk factor. Always start ART.', bold: false },
{ text: 'Toxoplasma is the most common cause of posterior uveitis worldwide – "headlight in the fog" next to an old scar is pathognomonic.', bold: false },
{ text: 'ARN requires IV Aciclovir urgently and prophylactic laser retinopexy to prevent devastating RRD.', bold: false },
{ text: 'PORN is ARN in the severely immunocompromised – no vitritis, rapid progression, very poor prognosis.', bold: false },
{ text: 'Birdshot: >95% HLA-A29 positive – this is a near-mandatory test. Visual field (not VA) is the monitoring tool.', bold: false },
{ text: 'VKH mimics posterior scleritis and Harada disease; early high-dose steroids prevent sunset glow fundus and chronic sequelae.', bold: false },
{ text: 'Serpiginous choroidopathy – always rule out TB before immunosuppression; ATT in endemic areas.', bold: false },
{ text: 'Luxturna (voretigene neparvovec) was the first FDA-approved gene therapy for any genetic disease – targets biallelic RPE65 mutations in RP.', bold: false },
{ text: 'OCTA is revolutionising choroiditis evaluation – it detects subclinical choriocapillaris flow voids and reveals activity in "quiet" eyes.', bold: false },
{ text: 'Ganciclovir-resistant CMV: suspect in patients failing therapy; test for UL97/UL54 mutations; Letermovir is a promising new alternative.', bold: false },
],
'Sources: Kanski\'s Clinical Ophthalmology 10e | Wills Eye Manual | Ryan\'s Retina 6e | PubMed 2021–2026'
);
// ─── FINAL SLIDE ──────────────────────────────────────────────────
const finalSl = pres.addSlide();
finalSl.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: '100%', h: '100%', fill: { color: DARK_BG } });
finalSl.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 0.4, h: '100%', fill: { color: ACCENT1 } });
finalSl.addShape(pres.ShapeType.rect, { x: 12.9, y: 0, w: 0.4, h: '100%', fill: { color: ACCENT2 } });
finalSl.addText('Thank You', {
x: 0.7, y: 2.2, w: 11.5, h: 1.5,
fontSize: 52, bold: true, color: WHITE, align: 'center', fontFace: 'Calibri',
});
finalSl.addText('Questions & Discussion', {
x: 0.7, y: 3.8, w: 11.5, h: 0.8,
fontSize: 24, color: ACCENT1, align: 'center', fontFace: 'Calibri',
});
finalSl.addText(
'References: Kanski\'s Clinical Ophthalmology 10e (Salmon & Kanski) | The Wills Eye Manual (Wolters Kluwer) | Ryan\'s Retina 6e (Schachat et al.) | Goldman-Cecil Medicine | PubMed PMIDs: 39549781, 37774799, 38983563, 38330155, 41599633, 38456233, 37176633, 41644040, 37798796, 40869487, 37691227, 34839010, 42096258',
{
x: 0.7, y: 5.5, w: 11.5, h: 1.8,
fontSize: 10, color: LIGHT_TXT, align: 'center', italic: true, fontFace: 'Calibri',
}
);
// ─── WRITE FILE ───────────────────────────────────────────────────
pres.writeFile({ fileName: '/home/daytona/workspace/retinitis_choroiditis/Retinitis_Choroiditis_Presentation.pptx' })
.then(() => console.log('SUCCESS: Presentation saved.'))
.catch(e => { console.error('ERROR:', e); process.exit(1); });
cd /home/daytona/workspace/retinitis_choroiditis && node build_pptx.js 2>&1
ls -lh /home/daytona/workspace/retinitis_choroiditis/Retinitis_Choroiditis_Prese…
Retinitis Choroiditis Presentation
Presentation · PPTX
What's Inside (27 slides, WIDE 16:9 format)
Slide-by-Slide Breakdown
| Section | Slides | Content |
|---|---|---|
| Title & Outline | 1–2 | Title, 9-section outline |
| 1. Anatomy | 3–4 | Retina vs choroid structure, key definitions (retinitis, choroiditis, panuveitis, white dot syndromes, IRU) |
| 2. Classification | 5–6 | ICG angiographic classification table (Kanski 10e) + infectious vs non-infectious retinitis two-column |
| 3. Viral Retinitis | 7–11 | CMV retinitis (intro, clinical features, diagnosis + treatment), ARN (criteria, treatment), PORN vs ARN comparison |
| 4. Parasitic/Fungal | 12–13 | Toxoplasma retinochoroiditis, Histoplasma/Pneumocystis/Cryptococcus/Candida |
| 5. RP & Inherited | 14–15 | RP genetics, clinical triad, gene therapy (Luxturna), stem cells, optogenetics |
| 6. Infectious Choroiditis | 16–17 | TB (serpiginous, Eales), Syphilis (ASPPC), Sarcoidosis, HIV microangiopathy |
| 7. White Dot Syndromes | 18–21 | MEWDS, APMPPE, Serpiginous choroidopathy, Birdshot, VKH, PIC, MFC, SO |
| 8. Clinical Trials | 22–25 | Three evidence slides with 5 studies each (PMIDs cited) + Ryan's Retina highlights |
| 9. Summary | 26–27 | Quick differential diagnosis table (11 conditions), Key Clinical Pearls, Thank You |
Key Clinical Trials & Recent Advances Included
- PMID 39549781 - CMV retinitis antiviral meta-analysis 2025 (valganciclovir = IV ganciclovir)
- PMID 37774799 - ARN antiviral systematic review 2024 (IV aciclovir + prophylactic laser)
- PMID 38456233 - VKH OCTA systematic review 2024 (subclinical choriocapillaris voids)
- PMID 40869487 - RP genetic therapies 2025 (RPGR, optogenetics, ASOs)
- PMID 37798796 - Stem cell therapy for inherited retinal disease (meta-analysis 2023)
- PMID 41599633 - Emerging ganciclovir resistance; Letermovir/Maribavir 2025
- PMID 41644040 - VKH multimodal imaging state-of-the-art 2026
- PMID 42096258 - SS-OCT biomarkers in toxoplasma retinochoroiditis 2026
continue
adalimumab non-infectious uveitis posterior clinical trial
retinitis pigmentosa optogenetics gene therapy clinical trial 2023 2024 2025
intravitreal dexamethasone implant uveitis macular edema
optogenetics retinal degeneration clinical trial human
sympathetic ophthalmia treatment outcomes immunosuppression
APMPPE serpiginous choroiditis multimodal imaging OCT
~/retinitis_choroiditis/build_extension.js
/**
* EXTENSION SCRIPT – adds ~20 new slides to the existing presentation
* Covers: Investigations/Imaging, Drug Protocols, Management Algorithms,
* Advanced Clinical Trials (MERIT, TRIOZ, VISUAL, MUV), Aspergillus/Coccidio,
* RP investigations, Syphilis chorioretinitis deep-dive, Emerging Therapies,
* Approach to Uveitis workup, and updated pearls.
*/
const pptxgen = require("pptxgenjs");
const pres = new pptxgen();
pres.layout = 'LAYOUT_WIDE';
pres.title = 'Retinitis & Choroiditis – Extended Module';
pres.author = 'Orris Medical AI';
// ─── PALETTE (identical to base deck for continuity) ─────────────
const DARK_BG = '0D1B2A';
const MID_BG = '1B2E44';
const ACCENT1 = '2FBFDE';
const ACCENT2 = 'E8A838';
const WHITE = 'F0F4F8';
const LIGHT_TXT = 'C9D8E6';
const RED_ACC = 'E05A5A';
const GREEN_ACC = '4CAF7D';
const PURPLE = '8B6FD6';
const TEAL2 = '1A8C8C';
// ─── HELPERS (copied verbatim) ────────────────────────────────────
function addSectionSlide(pres, sectionNo, title) {
const sl = pres.addSlide();
sl.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: '100%', h: '100%', fill: { color: MID_BG } });
sl.addShape(pres.ShapeType.rect, { x: 0, y: 2.5, w: '100%', h: 0.08, fill: { color: ACCENT1 } });
sl.addText(`Section ${sectionNo}`, { x: 1, y: 1.2, w: 11, h: 0.8, fontSize: 22, color: ACCENT2, fontFace: 'Calibri' });
sl.addText(title, { x: 1, y: 2.0, w: 11, h: 1.5, fontSize: 36, bold: true, color: WHITE, fontFace: 'Calibri' });
return sl;
}
function addContentSlide(pres, title, bullets, note, accentCol) {
const acc = accentCol || ACCENT1;
const sl = pres.addSlide();
sl.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: '100%', h: '100%', fill: { color: DARK_BG } });
sl.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: '100%', h: 0.75, fill: { color: MID_BG } });
sl.addShape(pres.ShapeType.rect, { x: 0, y: 0.72, w: 1.2, h: 0.06, fill: { color: acc } });
sl.addText(title, { x: 0.25, y: 0.1, w: 12.8, h: 0.6, fontSize: 22, bold: true, color: acc, fontFace: 'Calibri', valign: 'middle' });
const items = bullets.map((b) => ({
text: b.text || b,
options: {
bullet: b.sub ? { indent: 30 } : { type: 'bullet', indent: 18 },
color: b.sub ? LIGHT_TXT : WHITE,
fontSize: b.sub ? 14 : 16,
bold: b.bold || false,
breakLine: true,
}
}));
if (items.length) items[items.length - 1].options.breakLine = false;
sl.addText(items, { x: 0.3, y: 0.9, w: 12.5, h: 5.8, fontFace: 'Calibri', valign: 'top' });
if (note) sl.addText(note, { x: 0.3, y: 6.8, w: 12.5, h: 0.45, fontSize: 11, color: ACCENT2, italic: true, fontFace: 'Calibri' });
return sl;
}
function addTwoColSlide(pres, title, lTitle, lItems, rTitle, rItems, accentL, accentR) {
const aL = accentL || ACCENT1;
const aR = accentR || ACCENT2;
const sl = pres.addSlide();
sl.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: '100%', h: '100%', fill: { color: DARK_BG } });
sl.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: '100%', h: 0.75, fill: { color: MID_BG } });
sl.addShape(pres.ShapeType.rect, { x: 0, y: 0.72, w: 1.2, h: 0.06, fill: { color: aR } });
sl.addText(title, { x: 0.25, y: 0.1, w: 12.8, h: 0.6, fontSize: 22, bold: true, color: aR, fontFace: 'Calibri', valign: 'middle' });
sl.addShape(pres.ShapeType.rect, { x: 0.25, y: 0.85, w: 6.0, h: 0.45, fill: { color: aL }, rectRadius: 0.05 });
sl.addText(lTitle, { x: 0.35, y: 0.88, w: 5.8, h: 0.38, fontSize: 15, bold: true, color: DARK_BG, fontFace: 'Calibri' });
const lArr = lItems.map(b => ({ text: b.text||b, options: { bullet: true, color: b.highlight ? ACCENT2 : WHITE, fontSize: b.sub ? 13 : 15, bold: b.bold||false, breakLine: true } }));
if (lArr.length) lArr[lArr.length-1].options.breakLine = false;
sl.addText(lArr, { x: 0.3, y: 1.4, w: 5.9, h: 5.3, fontFace: 'Calibri', valign: 'top' });
sl.addShape(pres.ShapeType.rect, { x: 6.7, y: 0.85, w: 6.0, h: 0.45, fill: { color: aR }, rectRadius: 0.05 });
sl.addText(rTitle, { x: 6.8, y: 0.88, w: 5.8, h: 0.38, fontSize: 15, bold: true, color: DARK_BG, fontFace: 'Calibri' });
const rArr = rItems.map(b => ({ text: b.text||b, options: { bullet: true, color: b.highlight ? ACCENT1 : WHITE, fontSize: b.sub ? 13 : 15, bold: b.bold||false, breakLine: true } }));
if (rArr.length) rArr[rArr.length-1].options.breakLine = false;
sl.addText(rArr, { x: 6.75, y: 1.4, w: 5.9, h: 5.3, fontFace: 'Calibri', valign: 'top' });
sl.addShape(pres.ShapeType.line, { x: 6.55, y: 0.85, w: 0, h: 5.9, line: { color: ACCENT1, width: 1, dashType: 'dash' } });
return sl;
}
function addTableSlide(pres, title, headers, rows, accentCol) {
const acc = accentCol || ACCENT1;
const sl = pres.addSlide();
sl.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: '100%', h: '100%', fill: { color: DARK_BG } });
sl.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: '100%', h: 0.75, fill: { color: MID_BG } });
sl.addText(title, { x: 0.25, y: 0.1, w: 12.8, h: 0.6, fontSize: 22, bold: true, color: acc, fontFace: 'Calibri', valign: 'middle' });
const tableRows = [
headers.map(h => ({ text: h, options: { bold: true, color: DARK_BG, fill: acc, fontSize: 13, align: 'center' } })),
...rows.map((row, ri) => row.map(cell => ({ text: cell, options: { color: ri%2===0 ? WHITE : LIGHT_TXT, fill: ri%2===0 ? '162030' : '1B2E44', fontSize: 12, align: 'left' } })))
];
sl.addTable(tableRows, { x: 0.25, y: 0.9, w: 12.8, h: 5.9, border: { type: 'solid', pt: 0.5, color: acc }, fontFace: 'Calibri' });
return sl;
}
function addEvidenceSlide(pres, title, items) {
const sl = pres.addSlide();
sl.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: '100%', h: '100%', fill: { color: DARK_BG } });
sl.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: '100%', h: 0.75, fill: { color: '14241a' } });
sl.addShape(pres.ShapeType.rect, { x: 0, y: 0.72, w: 1.2, h: 0.06, fill: { color: GREEN_ACC } });
sl.addText(title, { x: 0.25, y: 0.1, w: 12.8, h: 0.6, fontSize: 22, bold: true, color: GREEN_ACC, fontFace: 'Calibri', valign: 'middle' });
items.forEach((item, i) => {
const yBase = 0.95 + i * 1.18;
if (yBase > 6.5) return;
sl.addShape(pres.ShapeType.rect, { x: 0.25, y: yBase, w: 12.5, h: 1.05, fill: { color: '162030' }, rectRadius: 0.08, line: { color: GREEN_ACC, width: 0.5 } });
sl.addText(item.label, { x: 0.4, y: yBase+0.04, w: 3.5, h: 0.4, fontSize: 12, bold: true, color: ACCENT2, fontFace: 'Calibri' });
sl.addText(item.pmid||'', { x: 10.5, y: yBase+0.04, w: 2.0, h: 0.4, fontSize: 10, color: GREEN_ACC, fontFace: 'Calibri', align: 'right' });
sl.addText(item.detail, { x: 0.4, y: yBase+0.44, w: 12.1, h: 0.55, fontSize: 13, color: LIGHT_TXT, fontFace: 'Calibri', valign: 'top' });
});
return sl;
}
function addFlowSlide(pres, title, steps) {
// A simple vertical flowchart-style slide
const sl = pres.addSlide();
sl.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: '100%', h: '100%', fill: { color: DARK_BG } });
sl.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: '100%', h: 0.75, fill: { color: MID_BG } });
sl.addShape(pres.ShapeType.rect, { x: 0, y: 0.72, w: 1.2, h: 0.06, fill: { color: PURPLE } });
sl.addText(title, { x: 0.25, y: 0.1, w: 12.8, h: 0.6, fontSize: 22, bold: true, color: PURPLE, fontFace: 'Calibri', valign: 'middle' });
const boxH = 0.7;
const gap = 0.22;
const startY = 0.88;
const cols = steps[0].length; // 1 or 3 per row
const bw = cols === 3 ? 3.8 : 11.5;
const bx = cols === 3 ? [0.3, 4.5, 8.7] : [0.6];
steps.forEach((row, ri) => {
const y = startY + ri * (boxH + gap);
row.forEach((step, ci) => {
const fillCol = step.color || (ri % 2 === 0 ? TEAL2 : PURPLE);
sl.addShape(pres.ShapeType.roundRect, { x: bx[ci], y, w: bw, h: boxH, fill: { color: fillCol }, rectRadius: 0.12 });
sl.addText(step.text, { x: bx[ci]+0.12, y: y+0.04, w: bw-0.24, h: boxH-0.08, fontSize: step.fontSize||13, bold: step.bold||false, color: WHITE, fontFace: 'Calibri', valign: 'middle', align: 'center', wrap: true });
});
// Arrow between rows (for single-col flows)
if (cols === 1 && ri < steps.length - 1) {
sl.addShape(pres.ShapeType.line, { x: 6.35, y: y+boxH, w: 0, h: gap, line: { color: ACCENT2, width: 2 }, });
}
});
return sl;
}
// ══════════════════════════════════════════════════════════════════
// PART A – INVESTIGATIVE APPROACH (New Sections 10-13)
// ══════════════════════════════════════════════════════════════════
// ─── SECTION 10 – INVESTIGATIONS & IMAGING ───────────────────────
addSectionSlide(pres, 10, 'Investigations & Multimodal Imaging');
addContentSlide(pres, 'Multimodal Imaging in Retinitis & Choroiditis – Overview',
[
{ text: 'Fundus Photography (FP):', bold: true },
{ text: ' Baseline documentation of lesion morphology, haemorrhage, exudates, pigmentation, vascular changes', sub: true },
{ text: 'Fluorescein Angiography (FA):', bold: true },
{ text: ' Gold standard for retinal vascular leakage, vasculitis, and disc staining', sub: true },
{ text: ' Patterns: early hypofluorescence (choriocapillaritis) vs late hyperfluorescence (active leakage)', sub: true },
{ text: ' Key: "pizza pie" hyperfluorescence in CMV; placoid early block in APMPPE', sub: true },
{ text: 'Indocyanine Green Angiography (ICGA):', bold: true },
{ text: ' Essential for choroidal imaging; detects lesions invisible on FA', sub: true },
{ text: ' Hypofluorescent lesions in Birdshot, MEWDS, VKH, serpiginous throughout all phases', sub: true },
{ text: 'OCT (Optical Coherence Tomography):', bold: true },
{ text: ' Retinal layer analysis: IS/OS disruption, ellipsoid zone loss, SRF, CMO, ERM, RPE changes', sub: true },
{ text: ' EDI-OCT: Enhanced Depth Imaging → choroidal thickness measurement (increased in VKH, decreased after treatment)', sub: true },
{ text: 'OCTA (OCT Angiography):', bold: true },
{ text: ' Non-invasive; detects choriocapillaris flow voids (VKH, MEWDS, Birdshot)', sub: true },
{ text: ' Identifies sub-clinical MNV (macular neovascularisation) without dye injection', sub: true },
{ text: 'Fundus Autofluorescence (FAF):', bold: true },
{ text: ' Hyperautofluorescence at active lesion margins (serpiginous, MEWDS, APMPPE)', sub: true },
{ text: ' Hypoautofluorescence = RPE atrophy / inactive scarring', sub: true },
],
'Kanski\'s Clinical Ophthalmology 10e; Baharani et al., Surv Ophthalmol 2022 (PMID 35007618)'
);
addTableSlide(pres, 'FA & ICGA Patterns in Key Choroiditis Syndromes',
['Condition', 'FA – Early', 'FA – Late', 'ICGA Pattern', 'FAF'],
[
['CMV Retinitis', 'Hyperfluorescence, leakage', 'Progressive staining', 'Not primary modality', 'N/A'],
['Toxoplasma', 'Hyperfluorescence (lesion)', 'Intense leakage + disc stain', 'Hypofluorescence', 'Hypoautofluorescence (scar)'],
['MEWDS', 'Hyperfluorescence (dots)', 'Hyperfluorescence', 'Early hypofluorescent dots', 'Hyper AF (multiple dots) – KEY'],
['APMPPE', 'Hypofluorescence (block)', 'Hyperfluorescence', 'Hypofluorescence all phases', 'Hyperautofluorescent'],
['Serpiginous', 'Hypofluorescence', 'Hyperfluorescence (active edge)', 'Hypofluorescence all phases', 'Hyperautofluorescent active edge'],
['Birdshot', 'Extensive vascular leakage', 'Diffuse staining', 'Multiple hypofluorescent spots (>clinical)', 'Hypoautofluorescent spots'],
['VKH', 'Multifocal hypofluorescent dots', 'Multiple serous RD; disc stain', 'Stromal hypofluorescence', 'Hypoautofluorescence (RPE)'],
['MFC/PIC', 'Hypofluorescence (lesion)', 'Late hyperfluorescence', 'Hypofluorescence; persistent old', 'Hypoautofluorescent lesions'],
],
ACCENT1
);
addContentSlide(pres, 'Systemic Workup for Posterior Uveitis / Retinitis',
[
{ text: 'Mandatory Blood Tests:', bold: true },
{ text: ' FBC, ESR, CRP, LFTs, RFTs, blood glucose', sub: true },
{ text: ' Syphilis serology: RPR/VDRL + TPHA/FTA-ABS (always rule out "the great imitator")', sub: true },
{ text: ' Quantiferon-Gold (TB-IGRA) / Mantoux; CXR or HRCT chest', sub: true },
{ text: ' HIV Ab/Ag (CD4+ count if positive); TORCH serology (toxoplasma IgG/IgM)', sub: true },
{ text: ' ACE + Serum lysozyme (sarcoidosis)', sub: true },
{ text: ' HLA-A29 (Birdshot); HLA-B51 (Behçet\'s disease)', sub: true },
{ text: 'Specific Microbiological Tests:', bold: true },
{ text: ' Aqueous/Vitreous PCR: CMV, HSV-1/2, VZV, EBV, Toxoplasma DNA', sub: true },
{ text: ' Goldmann-Witmer coefficient (GWC) for local antibody production (toxoplasma, CMV)', sub: true },
{ text: ' Metagenomic NGS: emerging for refractory/undiagnosed uveitis', sub: true },
{ text: 'Imaging:', bold: true },
{ text: ' Chest CT (sarcoidosis, TB, lymphoma), MRI brain (ARN, VKH, SSPE)', sub: true },
{ text: ' Lumbar puncture if CNS involvement suspected (APMPPE, ARN, neurosyphilis, VKH)', sub: true },
{ text: 'Electrophysiology:', bold: true },
{ text: ' Full-field ERG (RP, birdshot, cancer-associated retinopathy)', sub: true },
{ text: ' Pattern ERG, multifocal ERG, VEP as indicated', sub: true },
],
'Systematic approach recommended before initiating immunosuppression – always rule out infectious causes first'
);
// ─── SECTION 11 – DRUG PROTOCOLS ─────────────────────────────────
addSectionSlide(pres, 11, 'Drug Protocols & Treatment Ladders');
addTableSlide(pres, 'Antiviral Drug Protocols – CMV & Herpes Retinitis',
['Drug', 'Indication', 'Dose / Route', 'Duration', 'Key Notes'],
[
['Valganciclovir', 'CMV retinitis (induction + maintenance)', '900 mg BD PO (induction)\n900 mg OD PO (maintenance)', 'Induction: 3 wks\nMaintenance: until CD4 >150', 'Equivalent to IV GCV; preferred oral agent; renal dose adjustment required'],
['Ganciclovir IV', 'CMV – severe, vision-threatening', '5 mg/kg BD IV', '2–3 weeks induction', 'Myelosuppression (↓WBC/Plt); monitor FBC weekly'],
['Foscarnet IV', 'Ganciclovir-resistant CMV; ARN combination', '90 mg/kg BD IV', '2–3 weeks', 'Nephrotoxic; electrolyte imbalances (↓Ca, ↓Mg, ↓K)'],
['Cidofovir IV', 'Ganciclovir + Foscarnet resistant CMV', '5 mg/kg IV weekly × 2, then every 2 wks', 'Maintenance', 'Severe nephrotoxicity; must co-administer Probenecid + IV saline'],
['Aciclovir IV', 'ARN – first-line induction', '15 mg/kg every 8 h IV', '10–14 days', 'Then oral aciclovir 800 mg 5× daily × 6–12 wks; reduces 2nd eye risk'],
['Valaciclovir PO', 'ARN – alternative/step-down', '1–1.5 g TDS', '6–12 weeks after IV', 'Better bioavailability than aciclovir; preferred oral step-down'],
['Ganciclovir IVT', 'CMV – immediate macular threat', '2 mg in 0.05–0.1 ml', 'Every 1–2 weeks', 'Always combine with systemic therapy; no fellow-eye protection'],
['Letermovir', 'Ganciclovir-resistant CMV (emerging)', '480 mg OD PO/IV', 'Ongoing', 'CMV terminase inhibitor; novel mechanism; currently approved for CMV prophylaxis post-HSCT'],
],
ACCENT2
);
addTableSlide(pres, 'Anti-Parasitic / Anti-Fungal Drug Protocols',
['Drug', 'Indication', 'Dose', 'Duration', 'Key Notes'],
[
['Pyrimethamine + Sulfadiazine', 'Toxoplasma – gold standard', 'Pyrimeth 100 mg LD → 25–50 mg OD; Sulfa 1 g QID', '4–6 weeks', 'Add Folinic acid 5–10 mg OD to prevent marrow toxicity; monitor FBC'],
['TMP-SMX (Co-trimoxazole)', 'Toxoplasma – alternative; also prophylaxis', '960 mg BD (treatment) or 480 mg OD (prophylaxis)', '4–6 wks (Tx); long-term (prophylaxis)', 'Equally effective; avoid in sulfa allergy; covers PCP simultaneously'],
['Clindamycin IVT', 'Toxoplasma – intravitreal alternative', '1 mg/0.05 ml IVT', 'Weekly × 4–6 weeks', 'With IVT dexamethasone 400 µg; for systemic contraindication'],
['Amphotericin B IV', 'Candida, Cryptococcus, Aspergillus', '1 mg/kg/day', '2–6 weeks', 'Nephrotoxic; liposomal formulation preferred for renal protection'],
['Voriconazole PO/IV', 'Aspergillus, Candida, broad fungal', '400 mg BD LD → 200 mg BD', '4–6 weeks minimum', 'High ocular penetration; broad spectrum; monitor LFTs and QTc'],
['Fluconazole PO', 'Candida, Cryptococcus maintenance', '200–400 mg OD', 'Maintenance (indefinite in AIDS)', 'Well-tolerated; use after Ampho B induction for Cryptococcus'],
['Pyrimeth + Azithromycin', 'Toxoplasma – alternative', 'Pyrimeth 25 mg + Azithro 500 mg OD', '4–6 weeks', 'For sulfa-allergic patients (PMID 40698108)'],
['Isoniazid+Rifamp+Pyrazin+Ethamb', 'TB choroiditis – ATT standard 4-drug', 'Weight-based dosing', '2 months HRZE → 4–10 months HR', 'Add prednisolone 1 mg/kg in TB uveitis; serpiginous TB: longer ATT'],
],
GREEN_ACC
);
addTableSlide(pres, 'Immunosuppressive / Biologic Therapy for Non-Infectious Uveitis & Choroiditis',
['Drug', 'Class', 'Indication', 'Dose', 'Key Trial / Evidence'],
[
['Prednisolone', 'Corticosteroid', 'First-line all non-infectious', '1 mg/kg/day → taper', 'Standard of care'],
['Methotrexate', 'Antimetabolite', 'Birdshot, sarcoid, VKH (steroid-sparing)', '7.5–25 mg/wk + folic acid', 'Widely used; hepatotoxicity monitoring'],
['Mycophenolate Mofetil', 'Antimetabolite', 'VKH, birdshot, MFC, serpiginous', '1–3 g/day BD', 'Well-tolerated; preferred in childbearing age'],
['Azathioprine', 'Antimetabolite', 'VKH, sarcoid, serpiginous', '1–3 mg/kg/day', 'TPMT genotyping before initiation'],
['Cyclosporine', 'Calcineurin inhibitor', 'Birdshot, VKH, severe posterior uveitis', '2–5 mg/kg/day', 'Nephrotoxic; monitor BP and creatinine'],
['Adalimumab (Humira)', 'Anti-TNF biologic', 'Non-infectious uveitis (FDA approved)', '80 mg SC LD → 40 mg Q2W', 'VISUAL I+II trials (PMID 32469621) – reduces relapse and steroid burden'],
['Infliximab (Remicade)', 'Anti-TNF biologic', 'Sarcoid, Behçet\'s, refractory birdshot/VKH', '5–10 mg/kg IV Q6–8W', 'Highly effective; TB reactivation risk – screen before use'],
['Tocilizumab', 'Anti-IL-6 biologic', 'Refractory uveitic macular oedema', '8 mg/kg IV Q4W', 'Emerging evidence; Phase II trials'],
['Dexamethasone Implant (Ozurdex)', 'Intravitreal steroid', 'Uveitic CMO; posterior uveitis flare', '0.7 mg IVT implant', 'MERIT trial (PMID 37318415); TRIOZ trial (PMID 39168590)'],
],
PURPLE
);
// ─── SECTION 12 – MANAGEMENT ALGORITHMS ──────────────────────────
addSectionSlide(pres, 12, 'Management Algorithms');
addFlowSlide(pres, 'Management Algorithm – CMV Retinitis in AIDS',
[
[{ text: 'New AIDS Patient with Reduced Vision / Floaters', bold: true, color: MID_BG, fontSize: 15 }],
[{ text: 'Ophthalmological Assessment: Fundus Exam + FFA + CD4+ Count', color: TEAL2, fontSize: 13 }],
[{ text: 'CMV Retinitis Confirmed (Pizza-pie pattern; CD4 <50)', bold: true, color: '8B1A1A', fontSize: 14 }],
[{ text: 'Immediate: Oral Valganciclovir 900 mg BD + ART Optimisation\n(Intravitreal Ganciclovir if immediate macular threat)', color: TEAL2, fontSize: 13 }],
[{ text: '3-Week Induction → Maintenance 900 mg OD\nMonitor CD4+ count monthly', color: PURPLE, fontSize: 13 }],
[{ text: 'CD4+ >100-150 cells/µl maintained × 6 months', color: TEAL2, fontSize: 13 }],
[{ text: 'Discontinue anti-CMV maintenance therapy; continue ART\nMonitor for Immune Recovery Uveitis (IRU)', color: '2D5A1B', fontSize: 13 }],
]
);
addFlowSlide(pres, 'Management Algorithm – Acute Retinal Necrosis (ARN)',
[
[{ text: 'Patient: Healthy individual, Painful Red Eye + Floaters + Reduced Vision', bold: true, color: MID_BG, fontSize: 14 }],
[{ text: 'Slit-Lamp: Panuveitis (AU + Vitritis)\nFundus: Peripheral Yellow-White Necrosis + Occlusive Vasculitis', color: TEAL2, fontSize: 13 }],
[{ text: 'Aqueous PCR: HSV/VZV DNA Confirmed → Diagnose ARN', bold: true, color: '8B1A1A', fontSize: 14 }],
[{ text: 'Immediate: IV Aciclovir 15 mg/kg every 8 h IV × 10–14 days\n± Intravitreal Ganciclovir/Foscarnet', color: TEAL2, fontSize: 13 }],
[{ text: 'Prophylactic 360° Laser Retinopexy posterior to lesions (reduces RD: 75% → 35%)', bold: true, color: PURPLE, fontSize: 13 }],
[{ text: 'Step-down: Oral Valaciclovir 1–1.5 g TDS × 6–12 weeks\nOral Prednisolone if severe inflammation (after anti-viral cover)', color: TEAL2, fontSize: 13 }],
[{ text: 'Established RRD: PPV + Endolaser + Silicone Oil Tamponade', color: '8B1A1A', fontSize: 13 }],
]
);
addFlowSlide(pres, 'Management Algorithm – Non-Infectious Choroiditis (Step-Up Approach)',
[
[
{ text: 'Step 1\nTOPICAL & PERIOCULAR STEROIDS\n(mild localised disease)', color: '2D5A1B', fontSize: 12 },
{ text: 'Assess:\nVisual fields, ERG,\nFA/ICGA/OCT at 6-8 wks', color: MID_BG, fontSize: 12 },
{ text: 'If inadequate response\nor bilateral / severe\n→ Step 2', color: '6B3000', fontSize: 12 },
],
[
{ text: 'Step 2\nORAL PREDNISOLONE\n1 mg/kg/day + slow taper', color: TEAL2, fontSize: 12 },
{ text: 'Target:\nQuiescent inflammation\n<5 cells/HPF\nStable VA & fields', color: MID_BG, fontSize: 12 },
{ text: 'If >10mg/day needed\nfor >3 months → Step 3', color: '6B3000', fontSize: 12 },
],
[
{ text: 'Step 3\nSTEROID-SPARING IMMUNOSUPPRESSION\nMMF / MTX / Azathioprine', color: PURPLE, fontSize: 12 },
{ text: 'Duration:\nMinimum 2 years\nof quiescence before\ntaper attempt', color: MID_BG, fontSize: 12 },
{ text: 'If refractory\n→ Step 4', color: '6B3000', fontSize: 12 },
],
[
{ text: 'Step 4\nBIOLOGICS\nAdalimumab / Infliximab\nTocilizumab (CMO)', color: '8B1A1A', fontSize: 12 },
{ text: 'Monitoring:\nOphthalmic review Q4-8W\nSystemic monitoring\n(BP, LFTs, CBC)', color: MID_BG, fontSize: 12 },
{ text: 'Adjuncts:\nIVT Ozurdex for CMO\nAnti-VEGF for MNV', color: TEAL2, fontSize: 12 },
],
]
);
// ─── SECTION 13 – DEEP-DIVE CLINICAL ENTITIES ────────────────────
addSectionSlide(pres, 13, 'Deep-Dive: Selected Clinical Entities');
addTwoColSlide(pres, 'Syphilitic Chorioretinitis – The Great Imitator',
'Clinical Patterns',
[
{ text: 'Can mimic virtually any uveitis pattern – always test', bold: true, highlight: true },
{ text: 'Anterior uveitis (~4% of secondary syphilis)', sub: true },
{ text: ' Granulomatous or non-granulomatous; may have elevated IOP', sub: true },
{ text: 'Acute syphilitic posterior placoid chorioretinitis (ASPPC):', bold: true },
{ text: ' Single large yellow-orange placoid macular lesion', sub: true },
{ text: ' Strongly associated with HIV co-infection', sub: true },
{ text: ' FA: early hypofluorescence → late hyperfluorescence', sub: true },
{ text: 'Necrotising retinitis (mimics ARN/CMV)', sub: true },
{ text: 'Optic neuritis, papilloedema, neuroretinitis', sub: true },
{ text: 'Vitritis, panuveitis, episcleritis', sub: true },
{ text: 'Intermediate uveitis, retinal vasculitis', sub: true },
{ text: 'Congenital syphilis: interstitial keratitis, "salt and pepper" retinopathy, saddle nose deformity', sub: true },
],
'Diagnosis & Treatment',
[
{ text: 'Always test for HIV and STIs simultaneously', bold: true, highlight: true },
{ text: 'Serology:', bold: true },
{ text: ' Screening: RPR or VDRL (non-treponemal – titre correlates with disease activity)', sub: true },
{ text: ' Confirmatory: TPHA, FTA-ABS (treponemal – remain positive lifelong)', sub: true },
{ text: ' False positives in RPR: TB, leprosy, malaria, collagen disease', sub: true },
{ text: 'CSF analysis if neurosyphilis suspected (visual or neurological symptoms)', sub: true },
{ text: 'Treatment:', bold: true },
{ text: ' 1st line: IV Benzylpenicillin G 18–24 MU/day continuous or 3–4 MU IV Q4h × 10–14 days', sub: true },
{ text: ' Alternative (penicillin allergy): IV Ceftriaxone 2 g OD × 10–14 days', sub: true },
{ text: ' Follow-up RPR titres at 3, 6, 12 months (fourfold drop = treatment response)', sub: true },
{ text: 'Jarisch-Herxheimer reaction: fever, rigors within 24h of first treatment – reassure and treat symptomatically', sub: true },
], ACCENT1, ACCENT2
);
addTwoColSlide(pres, 'Multifocal Choroiditis & PIC – Current Approach',
'MFC – Multifocal Choroiditis with Panuveitis',
[
'Uncommon; usually bilateral but asymmetric; chronic/recurrent',
'Young/middle-aged women; often preceded by viral illness',
{ text: 'Key finding:', bold: true },
{ text: ' Ovoid yellowish-grey lesions 50–350 µm; posterior pole + periphery', sub: true },
{ text: ' Vitritis in 50% + anterior uveitis', sub: true },
{ text: ' Inactive lesions = punched-out scars resembling POHS', sub: true },
{ text: ' MNV occurs in 25–35%; CMO, subretinal fibrosis (SFU spectrum)', sub: true },
{ text: 'Investigations:', bold: true },
{ text: ' FA: early hypofluorescence, late hyperfluorescence; ICGA: hypofluorescent lesions', sub: true },
{ text: ' OCT: sub-RPE material, outer retina disruption', sub: true },
{ text: ' OCTA: choriocapillaris flow voids', sub: true },
{ text: 'New MUV Guideline (PMID 40288596):', bold: true, highlight: true },
{ text: ' Recommends OCTA + ICGA as standard workup for MFC; FAF for MNV surveillance', sub: true },
],
'PIC – Punctate Inner Choroidopathy',
[
'Young, highly myopic women (essentially no males)',
{ text: 'KEY: No vitritis or anterior uveitis – distinguishes from MFC', bold: true, highlight: true },
'Small (100–300 µm) punched-out lesions at level of inner choroid/RPE',
'Located at posterior pole; bilateral in ~75%',
{ text: 'MNV (CNV) in 40–75%:', bold: true },
{ text: ' Most common complication; major cause of VA loss', sub: true },
{ text: ' Anti-VEGF (Ranibizumab, Bevacizumab) is first-line treatment', sub: true },
{ text: 'FA: early hypofluorescence → late staining; MNV shows late leakage', sub: true },
{ text: 'OCTA: detects sub-clinical MNV before it causes symptoms', sub: true },
{ text: 'Active PIC lesions: consider short-course oral prednisolone to reduce new lesion formation', sub: true },
{ text: 'New MUV Guideline 2025 (PMID 40288596):', bold: true, highlight: true },
{ text: ' Standardised OCTA protocol for MNV detection and follow-up recommended', sub: true },
]
);
addContentSlide(pres, 'Aspergillus Endophthalmitis & Rare Fungal Choroiditis',
[
{ text: 'Aspergillus Endophthalmitis:', bold: true },
{ text: ' Risk factors: IV drug use, chronic lung disease, organ transplantation, neutropenia', sub: true },
{ text: ' Presentation: Iridocyclitis, vitritis, yellow retinal/subretinal macular infiltrates (earlier macular involvement than Candida)', sub: true },
{ text: ' Occlusive retinal vasculitis is common; rapid progression; endocarditis risk', sub: true },
{ text: ' Treatment: Voriconazole (high ocular penetration) PO/IV + intravitreal Voriconazole; early PPV', sub: true },
{ text: 'Coccidioidomycosis:', bold: true },
{ text: ' Coccidioides immitis via inhalation; severe granulomatous AU + multifocal choroiditis', sub: true },
{ text: ' Endemic in southwestern USA, Mexico; treatment: Fluconazole/Itraconazole', sub: true },
{ text: 'Candida Chorioretinitis – Diagnostic Pearls:', bold: true },
{ text: ' "String of pearls" white vitreous infiltrate = pathognomonic of Candida endophthalmitis', sub: true },
{ text: ' Risk: IV drug abuse, TPN, broad-spectrum antibiotics, immunosuppression, indwelling catheters', sub: true },
{ text: ' Fluconazole systemic + intravitreal Amphotericin B (5–10 µg) or Voriconazole', sub: true },
{ text: ' Early PPV for vitreous involvement; reduces fungal load and improves drug penetration', sub: true },
{ text: 'IDSA Guidelines on Fungal Endophthalmitis:', bold: true },
{ text: ' IV Amphotericin B + Flucytosine for Candida/Cryptococcus; Voriconazole for Aspergillus; resistance screening recommended', sub: true },
],
'Kanski\'s Clinical Ophthalmology 10e, pp.497–502'
);
addTwoColSlide(pres, 'Sympathetic Ophthalmia – Advanced Concepts',
'Pathogenesis & Clinical Features',
[
'Bilateral granulomatous panuveitis after penetrating ocular trauma or intraocular surgery',
{ text: 'Pathogenesis:', bold: true },
{ text: ' Autoimmune reaction to uveal pigment antigens (S-antigen, IRBP, recoverin) exposed at surgery/trauma', sub: true },
{ text: ' HLA-DR4, HLA-DQw3 associations', sub: true },
{ text: 'Timing:', bold: true },
{ text: ' Shortest recorded: 5 days; 90% within 1 year', sub: true },
{ text: ' Peak risk: 4–8 weeks after injury', sub: true },
{ text: ' Rare cases: decades later after seemingly minor surgery', sub: true },
{ text: 'Exciting eye: worsening panuveitis', sub: true },
{ text: 'Sympathising eye (fellow): initially anterior uveitis → granulomatous panuveitis, multiple choroidal granulomas (Dalen-Fuchs nodules), disc oedema, serous RD', sub: true },
{ text: 'Dalen-Fuchs nodules:', bold: true },
{ text: ' Subretinal granulomatous aggregates of RPE + macrophages; appear between Bruch\'s membrane and RPE', sub: true },
],
'Prophylaxis & Treatment',
[
{ text: 'CRITICAL POINT:', bold: true, highlight: true },
{ text: ' Evisceration/enucleation of the exciting eye within 2 weeks of injury MAY prevent SO', sub: true },
{ text: ' Once SO is established, removal of exciting eye does NOT improve the sympathising eye prognosis', sub: true },
{ text: 'Treatment:', bold: true },
{ text: ' High-dose oral corticosteroids: Prednisolone 1–1.5 mg/kg/day', sub: true },
{ text: ' Taper slowly over ≥12 months; relapse common on rapid withdrawal', sub: true },
{ text: ' Steroid-sparing: Mycophenolate, Azathioprine, Cyclosporine', sub: true },
{ text: ' Biologics (Infliximab, Adalimumab) for refractory cases', sub: true },
{ text: 'Risk factors for SO after surgery:', bold: true },
{ text: ' Vitreoretinal surgery (highest), repeat procedures, pars planitis surgery, trauma with uveal prolapse', sub: true },
{ text: 'Recent review (PMID 34494974):', bold: false },
{ text: ' Modern immunosuppression protocols achieve long-term remission in >70%; prognosis has markedly improved', sub: true },
{ text: 'OCTA and EDI-OCT now preferred for non-invasive disease monitoring', sub: true },
]
);
addContentSlide(pres, 'Retinitis Pigmentosa – Full Investigation Protocol',
[
{ text: 'Electrophysiology (ISCEV Standards):', bold: true },
{ text: ' Full-field ERG: Reduced/extinguished rod (scotopic) responses earliest; photopic responses late', sub: true },
{ text: ' Pattern ERG (PERG): assesses macular ganglion cell function', sub: true },
{ text: ' Electro-oculogram (EOG): Arden ratio reduced (RPE dysfunction)', sub: true },
{ text: ' Dark adaptometry: prolonged adaptation curve (elevated final rod threshold)', sub: true },
{ text: 'Structural Imaging:', bold: true },
{ text: ' FAF: Abnormal perimacular hyperautofluorescent ring (hallmark) + patchy peripheral hypoAF', sub: true },
{ text: ' OCT: IS/OS (ellipsoid zone) disruption from mid-periphery inward; CMO detection (20%); macular atrophy (40%)', sub: true },
{ text: ' FAF distinguishes RP from normal fundus in 95% as stand-alone test', sub: true },
{ text: ' EDI-OCT: Choroidal thinning in advanced RP', sub: true },
{ text: 'Visual Fields:', bold: true },
{ text: ' Goldmann perimetry: mid-peripheral ring scotoma → tubular vision ("tunnel vision")', sub: true },
{ text: ' Automated (Humphrey 30-2, 60-4): central islands of preserved field', sub: true },
{ text: ' Microperimetry: macular sensitivity for monitoring central function', sub: true },
{ text: 'Genetics:', bold: true },
{ text: ' Next-generation sequencing panels (100+ genes) – identifies causative mutation in ~60% currently', sub: true },
{ text: ' Mandatory for gene therapy eligibility (e.g., RPE65 Sanger sequencing for Luxturna)', sub: true },
{ text: ' Genetic counselling: essential; risk calculation for offspring by inheritance pattern', sub: true },
{ text: ' X-linked carrier females: FAF shows centrifugal hyperautofluorescent lines', sub: true },
],
'Kanski\'s Clinical Ophthalmology 10e, p.648; Gene therapy trials: PMID 39930178'
);
// ═══════════════════════════════════════════════════════════════════
// PART B – ADDITIONAL CLINICAL TRIALS & ADVANCES
// ═══════════════════════════════════════════════════════════════════
addSectionSlide(pres, 14, 'Additional Clinical Trials\nPubMed 2021–2026');
addEvidenceSlide(pres, 'Landmark Trials – Uveitic Macular Edema & Intravitreal Therapy',
[
{
label: 'MERIT Trial – Dexamethasone vs MTX vs Ranibizumab (RCT 2023)',
pmid: 'PMID 37318415',
detail: 'MERIT RCT (Ophthalmology 2023): Intravitreal dexamethasone implant (Ozurdex) achieved best visual gains at 12 months for uveitic CMO. Methotrexate IVT was safer (no IOP rise). Ranibizumab was least effective. Dex implant becomes preferred for non-infectious uveitic CMO.'
},
{
label: 'MERIT 24-Week Re-treatment Outcomes (RCT 2025)',
pmid: 'PMID 39612949',
detail: 'MERIT Group (Ophthalmology 2025): 24-week re-treatment analysis confirms IVT dexamethasone superiority for sustained CMO resolution. IOP elevation in 30% managed medically. Identifies CMO re-treatment criteria: >20% increase in CRT from best response.'
},
{
label: 'TRIOZ Trial – Subconjunctival Triamcinolone vs IVT Ozurdex (RCT Phase III 2025)',
pmid: 'PMID 39168590',
detail: 'Phase III RCT in Br J Ophthalmol (Couret et al., 2025): Subconjunctival triamcinolone non-inferior to IVT Ozurdex at 3 months for uveitic/post-op CMO. Fewer IOP spikes with subconjunctival route. Provides a less invasive alternative to intravitreal injection.'
},
{
label: 'VISUAL I+II Trials – Adalimumab for Non-Infectious Uveitis (RCT 2021)',
pmid: 'PMID 32469621',
detail: 'Merrill et al. (Ocul Immunol Inflamm, 2021): Post-hoc analysis of VISUAL I (active) and II (inactive) RCTs confirms adalimumab reduces time-to-treatment-failure across ALL non-infectious uveitis subtypes. Most benefit in HLA-B27-associated and Birdshot uveitis. Led to FDA approval of adalimumab for non-infectious uveitis.'
},
{
label: 'Intravitreal vs Systemic Treatment in Cataract Surgery with Uveitis (Meta-Analysis 2023)',
pmid: 'PMID 36271933',
detail: 'Meta-analysis Graefes 2023: Perioperative IVT dexamethasone reduces post-cataract CMO flare in uveitis patients equally to systemic prednisolone; IVT route avoids systemic side effects in patients already on long-term immunosuppression.'
},
]
);
addEvidenceSlide(pres, 'Emerging Therapies & Imaging Guidelines 2024–2026',
[
{
label: 'MUV Taskforce – MFC & PIC Imaging Guidelines (Practice Guideline 2025)',
pmid: 'PMID 40288596',
detail: 'MUV Taskforce Report 5 (Am J Ophthalmol 2025): Evidence and consensus-based imaging guidelines for MFC and PIC. OCTA for MNV surveillance is now standard; ICGA required to classify choroidal lesion burden. Regular FAF recommended for RPE atrophy monitoring. Standardises follow-up intervals by disease activity.'
},
{
label: 'MUV Taskforce – MEWDS Imaging Consensus (Guideline 2025)',
pmid: 'PMID 40571046',
detail: 'MUV Taskforce Report 6 (Am J Ophthalmol 2025): FAF and OCTA are now the essential diagnostic tools for MEWDS. FAF shows hyperautofluorescent dots (present when fundus dots already invisible); OCTA shows choriocapillaris flow voids. ICG also recommended. Diagnosis should include multimodal imaging even when fundus appears normal.'
},
{
label: 'White Spot Syndromes – Advances in Understanding (Review 2023)',
pmid: 'PMID 37574123',
detail: 'Cicinelli et al. (Prog Retin Eye Res, 2023): Unifying concept: most white dot syndromes share a common primary target (choriocapillaris) with variable spread to RPE and outer retina. "Two-hit" model proposed (genetic susceptibility + infectious/environmental trigger). OCTA flow voids are the most sensitive marker of active choriocapillaritis.'
},
{
label: 'Optogenetics for Retinal Degeneration – Ethical & Clinical Perspectives (Review 2022)',
pmid: 'PMID 34724112',
detail: 'Harris & Gilbert (Graefes 2022): First human optogenetics trial (genetically blind RP patient restored partial vision using intravitreal AAV2-ChrimsonR; NEJM 2021). Challenges include: limited light sensitivity, spectral restriction, and latency. Long-term gene expression durability being studied in ongoing Phase I/II trials.'
},
{
label: 'Gene Therapy Trials for Inherited Retinal Diseases – Frequency Analysis (2025)',
pmid: 'PMID 39930178',
detail: 'Ameri et al. (Adv Exp Med Biol, 2025): >60 gene therapy clinical trials active for IRDs as of 2024. RPE65 (Luxturna), RPGR (XL-RP), CNGB3 (achromatopsia), CNGA3, PDE6A, PDE6B are most advanced. Subretinal and intravitreal routes compared; subretinal achieves higher transduction efficiency.'
},
]
);
// ─── SECTION 15 – COMPLICATIONS & SPECIAL POPULATIONS ────────────
addSectionSlide(pres, 15, 'Complications, Special Populations & Pearls');
addTwoColSlide(pres, 'Complications of Retinitis & Choroiditis',
'Vision-Threatening Complications',
[
{ text: 'Retinal Detachment (RRD):', bold: true },
{ text: ' ARN: up to 75% without prophylaxis; PPV + SO', sub: true },
{ text: ' CMV retinitis: up to 50% in advanced disease', sub: true },
{ text: ' PORN: nearly 70% within weeks', sub: true },
{ text: 'Macular Neovascularisation (MNV/CNV):', bold: true },
{ text: ' POHS (40%), PIC (40–75%), MFC (25–35%), VKH (chronic phase), Birdshot', sub: true },
{ text: ' Treatment: anti-VEGF (Ranibizumab, Bevacizumab, Aflibercept)', sub: true },
{ text: 'Cystoid Macular Oedema (CMO):', bold: true },
{ text: ' Common in birdshot, VKH, sarcoid, intermediate uveitis, post-CMV IRU', sub: true },
{ text: ' IVT Ozurdex / IVT MTX; systemic immunosuppression; anti-VEGF limited role', sub: true },
{ text: 'Optic Atrophy:', bold: true },
{ text: ' End-stage birdshot, serpiginous, ARN, CMV; irreversible visual loss', sub: true },
{ text: 'Glaucoma (Secondary):', bold: true },
{ text: ' VKH, sarcoid (trabecular granulomas), steroid-induced OHT, CMV anterior uveitis', sub: true },
],
'Cataract & Systemic Complications',
[
{ text: 'Posterior Subcapsular Cataract (PSC):', bold: true },
{ text: ' RP (very common), corticosteroid-induced, chronic uveitis', sub: true },
{ text: ' Cataract extraction in active uveitis: cover with perioperative IV steroids + IVT dexamethasone', sub: true },
{ text: 'Epiretinal Membrane (ERM):', bold: true },
{ text: ' Post-CMV retinitis, after heavy laser treatment, chronic inflammation', sub: true },
{ text: ' PPV + ERM peel if VA <6/12 with metamorphopsia', sub: true },
{ text: 'Optic Neuritis:', bold: true },
{ text: ' Direct viral spread (CMV, ARN); VKH-associated; sarcoid; syphilis', sub: true },
{ text: 'Drug Side Effects to Monitor:', bold: true },
{ text: ' Chloroquine/HCQ: maculopathy (dose >5 mg/kg/day real weight) – annual OCT + mfERG baseline', sub: true },
{ text: ' Rifabutin: anterior uveitis (hypopyon) – common in HIV patients on prophylaxis', sub: true },
{ text: ' Cidofovir: hypotony (uveitis mechanism)', sub: true },
{ text: ' Corticosteroids: steroid-induced OHT, PSC, systemic diabetes, osteoporosis', sub: true },
{ text: 'Special Populations:', bold: true },
{ text: ' Pregnancy: avoid sulfonamides (Toxo treatment) in 3rd trimester; use spiramycin', sub: true },
{ text: ' Paediatric: congenital toxo, rubella retinopathy, paediatric VKH', sub: true },
]
);
addContentSlide(pres, 'HIV/AIDS Ocular Spectrum – Systematic Overview',
[
{ text: 'Retinal Microangiopathy (most common, 70%):', bold: true },
{ text: ' Cotton-wool spots + haemorrhages; marker for CMV retinitis risk; spontaneous resolution; ART is treatment', sub: true },
{ text: 'CMV Retinitis (most important infectious complication):', bold: true },
{ text: ' CD4+ <50; "pizza pie" retinitis; valganciclovir + ART; discontinue at CD4 >150', sub: true },
{ text: 'Immune Recovery Uveitis (IRU):', bold: true },
{ text: ' After ART in CMV retinitis; severe vitritis, CMO, ERM; treat with IVT or periocular steroids', sub: true },
{ text: 'Toxoplasma Retinochoroiditis (AIDS):', bold: true },
{ text: ' Atypical: multiple lesions, no adjacent scar, minimal vitritis; PCR confirmation helpful', sub: true },
{ text: 'Pneumocystis Choroiditis:', bold: true },
{ text: ' CD4+ <100; pale choroidal lesions; no vitritis; TMP-SMX prophylaxis has nearly eliminated this', sub: true },
{ text: 'Cryptococcal Choroiditis:', bold: true },
{ text: ' Associated with CNS cryptococcosis; multifocal choroidal lesions + papilloedema; Ampho B + Fluconazole', sub: true },
{ text: 'PORN (Progressive Outer Retinal Necrosis):', bold: true },
{ text: ' VZV-driven; CD4+ <10; no vitritis; rapid progression; combination IV ganciclovir + foscarnet', sub: true },
{ text: 'Primary CNS Lymphoma / Intraocular Lymphoma:', bold: true },
{ text: ' Masquerade syndrome; vitritis + subretinal deposits; diagnose by vitreous biopsy for IL-10; treat with methotrexate + radiotherapy', sub: true },
],
'Kanski\'s Clinical Ophthalmology 10e, pp.487-503'
);
// ─── SECTION 16 – APPROACH TO PATIENT ────────────────────────────
addSectionSlide(pres, 16, 'Approach to a Patient with\nPosterior Uveitis / Retinitis');
addFlowSlide(pres, 'Stepwise Diagnostic Approach to Posterior Uveitis',
[
[{ text: 'History: Age, Immunostatus (HIV, transplant), Systemic disease, Travel, Sexual history, TB contacts, Drug history', bold: false, color: TEAL2, fontSize: 13 }],
[{ text: 'Examination: VA, IOP, Slit lamp (AU), Fundus (pattern recognition: location, borders, haemorrhage, vasculitis)', color: MID_BG, fontSize: 13 }],
[
{ text: 'Pattern A\nInfectious Retinitis\n(haemorrhagic, necrotic lesions\nHigh vitritis)', color: '8B1A1A', fontSize: 12 },
{ text: 'Pattern B\nIdiopathic Choroiditis\n(White/cream spots, no/mild vitritis\nSelf-limited)', color: TEAL2, fontSize: 12 },
{ text: 'Pattern C\nGranulomatous Choroiditis\n(HNL granulomas, multisystem\nSarcoid/TB/VKH)', color: PURPLE, fontSize: 12 },
],
[
{ text: 'Pattern A workup:\nAqueous PCR (CMV/HSV/VZV/Toxo)\nCD4+ count; Serology', color: '8B1A1A', fontSize: 12 },
{ text: 'Pattern B workup:\nHLA-A29 (Birdshot)\nFA/ICGA/OCT/FAF\nMUV imaging guidelines', color: TEAL2, fontSize: 12 },
{ text: 'Pattern C workup:\nACE/lysozyme, CXR/CT\nQuantiferon-Gold, VDRL+TPHA\nTissue biopsy if needed', color: PURPLE, fontSize: 12 },
],
[{ text: 'Treat specific cause identified → review response at 6–8 weeks with repeat imaging + VA + IOP', color: '2D5A1B', fontSize: 13 }],
[{ text: 'No response or diagnosis unclear: Vitreous biopsy (cytology, culture, PCR panel, IL-10 for lymphoma)\nConsider metagenomic NGS', color: '6B3000', fontSize: 13 }],
]
);
// ─── SECTION 17 – ADVANCED PEARLS & FUTURE DIRECTIONS ────────────
addSectionSlide(pres, 17, 'Advanced Pearls & Future Directions');
addContentSlide(pres, 'Advanced Clinical Pearls for the Specialist',
[
{ text: 'CMV anterior uveitis in immunocompetent:', bold: true },
{ text: ' Presents as unilateral chronic/recurrent anterior uveitis with elevated IOP + corneal endotheliitis; distinguish from HSV by failure to respond to aciclovir; treat with oral valganciclovir', sub: true },
{ text: 'Frosted Branch Angiitis (FBA):', bold: true },
{ text: ' Striking vascular sheathing; seen in CMV retinitis (~6%), EBV infection, lymphoma, idiopathic (primary FBA – good prognosis); always rule out CMV/lymphoma', sub: true },
{ text: 'SSPE (Subacute Sclerosing Panencephalitis):', bold: true },
{ text: ' Measles-associated CNS degeneration; classical macular grey-white lesion → RPE atrophy scar; onset 6–15 yrs post-measles; fatal; posterior uveitis may be presenting feature', sub: true },
{ text: 'IRVAN (Idiopathic Retinal Vasculitis, Aneurysms, Neuroretinitis):', bold: true },
{ text: ' Rare; arteriolar aneurysms + disc exudates + neuroretinitis; laser photocoagulation to aneurysms + areas of non-perfusion', sub: true },
{ text: 'Acute Idiopathic Maculopathy:', bold: true },
{ text: ' Self-limiting; young adults; Coxsackievirus association; serous macular detachment + oedema → spontaneous resolution; no treatment needed', sub: true },
{ text: 'Relentless Placoid Chorioretinitis (RPC / Ampiginous):', bold: true },
{ text: ' Hundreds of lesions spanning entire retina; chronic, relentless course unlike self-limited APMPPE; sustained immunosuppression required', sub: true },
{ text: '"Sunset Glow Fundus" (VKH):', bold: true },
{ text: ' Pathognomonic of chronic VKH; diffuse RPE depigmentation giving orange background glow; indicates inadequately treated or late VKH; associated with complications including CNV, glaucoma, subretinal fibrosis', sub: true },
],
'Kanski\'s Clinical Ophthalmology 10e, pp.487-520'
);
addContentSlide(pres, 'Future Directions in Retinitis & Choroiditis',
[
{ text: 'Gene Therapy Pipeline (2025–2026):', bold: true },
{ text: ' Active Phase I/II trials: RPGR (XL-RP), CNGA3 (achromatopsia), CNGB3, RLBP1 (Bothnia dystrophy), ABCA4 (Stargardt) – PMID 39930178', sub: true },
{ text: ' Dual-vector AAV strategies for large genes (USH2A, ABCA4) overcoming 4.7kb AAV packaging limit', sub: true },
{ text: 'Optogenetics:', bold: true },
{ text: ' AAV2-ChrimsonR (AGTC): first Phase I/II success in end-stage RP (NEJM 2021); ongoing Phase III trials', sub: true },
{ text: ' Limitation: requires light goggles; photosensitivity threshold being refined', sub: true },
{ text: 'Stem Cell Therapies:', bold: true },
{ text: ' iPS-derived RPE transplantation (subretinal): Phase II ongoing (Japan and USA)', sub: true },
{ text: ' hESC-derived RPE sheet: Phase I/II showing sustained VA stability at 24 months (PMID 37798796)', sub: true },
{ text: 'AI & OCT-Guided Disease Monitoring:', bold: true },
{ text: ' Deep learning algorithms for automated detection of choroidal granulomas, CNV, and lesion progression in uveitis', sub: true },
{ text: ' AI triage for CMV retinitis screening in HIV clinics (PMID 42279083)', sub: true },
{ text: 'New Biologics Under Investigation:', bold: true },
{ text: ' Secukinumab (anti-IL-17): Phase II for Behçet\'s and non-infectious uveitis', sub: true },
{ text: ' Faricimab (anti-VEGF + anti-Ang-2 bispecific): for neovascular complications of choroiditis', sub: true },
{ text: ' Letermovir / Maribavir: new antivirals for ganciclovir-resistant CMV retinitis (Phase II)', sub: true },
],
'Sources: PMID 39930178, 37798796, 34724112, 40869487, 42279083'
);
// ─── FINAL SLIDE OF EXTENSION ─────────────────────────────────────
const endSl = pres.addSlide();
endSl.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: '100%', h: '100%', fill: { color: DARK_BG } });
endSl.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 0.4, h: '100%', fill: { color: ACCENT1 } });
endSl.addShape(pres.ShapeType.rect, { x: 12.9, y: 0, w: 0.4, h: '100%', fill: { color: ACCENT2 } });
endSl.addShape(pres.ShapeType.rect, { x: 0.5, y: 2.4, w: 12.3, h: 0.06, fill: { color: ACCENT1 } });
endSl.addText('Extended Module Complete', {
x: 0.7, y: 1.3, w: 11.5, h: 1.0, fontSize: 36, bold: true, color: WHITE, align: 'center', fontFace: 'Calibri',
});
endSl.addText('Retinitis & Choroiditis – Sections 10–17', {
x: 0.7, y: 2.6, w: 11.5, h: 0.7, fontSize: 22, color: ACCENT1, align: 'center', fontFace: 'Calibri',
});
endSl.addText([
{ text: 'Investigations & Imaging | ', options: { color: LIGHT_TXT, fontSize: 14 } },
{ text: 'Drug Protocols | ', options: { color: ACCENT2, fontSize: 14 } },
{ text: 'Management Algorithms | ', options: { color: LIGHT_TXT, fontSize: 14 } },
{ text: 'Deep-Dives | ', options: { color: ACCENT1, fontSize: 14 } },
{ text: 'Clinical Trials | ', options: { color: ACCENT2, fontSize: 14 } },
{ text: 'Future Directions', options: { color: LIGHT_TXT, fontSize: 14 } },
], { x: 0.7, y: 3.5, w: 11.5, h: 0.5, fontFace: 'Calibri', align: 'center' });
endSl.addText(
'Key Trials: MERIT (PMID 37318415) | TRIOZ (PMID 39168590) | VISUAL I+II (PMID 32469621) | MUV-5 (PMID 40288596) | MUV-6 (PMID 40571046)\nSources: Kanski\'s 10e | Wills Eye Manual | Ryan\'s Retina 6e | PubMed 2021–2026',
{ x: 0.7, y: 5.8, w: 11.5, h: 1.4, fontSize: 10, color: LIGHT_TXT, italic: true, align: 'center', fontFace: 'Calibri' }
);
// ─── WRITE FILE ──────────────────────────────────────────────────
pres.writeFile({ fileName: '/home/daytona/workspace/retinitis_choroiditis/Retinitis_Choroiditis_Extended.pptx' })
.then(() => console.log('SUCCESS: Extended presentation saved.'))
.catch(e => { console.error('ERROR:', e); process.exit(1); });
cd /home/daytona/workspace/retinitis_choroiditis && node build_extension.js 2>&1
ls -lh /home/daytona/workspace/retinitis_choroiditis/
Retinitis Choroiditis Presentation
Presentation · PPTX
Retinitis Choroiditis Extended
Presentation · PPTX
What Was Added in the Extended Module (Sections 10–17)
Section 10 – Investigations & Multimodal Imaging
- Full comparison of FA, ICGA, OCT, EDI-OCT, OCTA, FAF and their specific patterns in each major condition
- Comprehensive FA/ICGA patterns table (8 conditions)
- Systematic workup table: blood tests, PCR, Goldmann-Witmer coefficient, mNGS, imaging, electrophysiology
Section 11 – Drug Protocols (3 detailed tables)
- Antiviral protocols: Valganciclovir, IV Ganciclovir, Foscarnet, Cidofovir, Aciclovir, Letermovir - doses, durations, monitoring
- Anti-parasitic/antifungal: Pyrimethamine/sulfadiazine, TMP-SMX, IVT Clindamycin, Amphotericin B, Voriconazole, ATT for TB
- Immunosuppression ladder: Prednisolone, MTX, MMF, Azathioprine, Cyclosporine, Adalimumab, Infliximab, Tocilizumab, Ozurdex
Section 12 – Management Algorithms (3 flowcharts)
- CMV retinitis in AIDS: step-by-step from diagnosis to ART discontinuation
- ARN: IV aciclovir → laser retinopexy → PPV with silicone oil
- Non-infectious choroiditis: 4-step immunosuppression ladder
Section 13 – Deep-Dives
- Syphilitic chorioretinitis - ASPPC, serology, IV penicillin protocol
- MFC vs PIC - MUV 2025 imaging guidelines integrated
- Aspergillus & Coccidioidomycosis - management protocols
- Sympathetic ophthalmia - 2-week evisceration rule, modern immunosuppression
- RP - complete electrophysiology and imaging investigation protocol
Section 14 – New Clinical Trials
- MERIT RCT 2023 (PMID 37318415) - IVT Ozurdex best for uveitic CMO
- MERIT 24-week 2025 (PMID 39612949) - Re-treatment criteria defined
- TRIOZ Phase III RCT 2025 (PMID 39168590) - Subconjunctival triamcinolone vs Ozurdex
- VISUAL I+II post-hoc 2021 (PMID 32469621) - Adalimumab across all uveitis subtypes
- MUV Taskforce 5 & 6 Guidelines 2025 (PMID 40288596, 40571046)
Sections 15–17 – Complications, HIV Spectrum, Diagnostic Approach Flowchart, Future Directions
- Retinal detachment, MNV, CMO, glaucoma, drug toxicity, pregnancy considerations
- Full HIV ocular spectrum (9 entities)
- 6-step diagnostic algorithm flowchart
- Gene therapy pipeline 2025-2026, optogenetics (AAV2-ChrimsonR trial), AI-guided monitoring, new biologics
Chrons disease and eye
Crohn disease ocular manifestations uveitis episcleritis
inflammatory bowel disease uveitis pathophysiology treatment biologics
IBD anti-TNF vedolizumab ustekinumab ocular side effects uveitis
PMID: 39767762
PMID: 36497759
PMID: 38247834
Crohn's Disease & the Eye
1. Epidemiology
2. Pathophysiology
- Shared antigenic targets between gut mucosa and ocular tissues (uveal tract, episclera) - cross-reactive T-cells activated in the gut migrate to the eye
- Immune dysregulation - dysregulated Th1/Th17 responses; elevated TNF-α, IL-6, IL-17, IL-23 in both bowel and uveal inflammation
- HLA associations - HLA-B27 (anterior uveitis); HLA-DR2 (posterior uveitis in IBD); HLA-B44 (episcleritis in CD)
- Gut-eye axis - increased intestinal permeability allows bacterial antigens to enter the circulation and deposit in ocular vasculature, triggering inflammation
- Molecular mimicry - retinal S-antigen and gut bacteria share epitopes in animal models
3. Ocular Manifestations – Full Spectrum
3A. Episcleritis (Most Common)
- Affects the superficial episcleral vascular plexus
- Two types: Simple (75%, sectoral or diffuse, usually bilateral) and Nodular (25%)
- Key clinical point: Acute episcleritis closely correlates with bowel disease activity - it flares when CD flares and settles with bowel remission
- Symptoms: Mild discomfort, grittiness; up to 50% are asymptomatic
- Signs: Sectoral or diffuse redness in an interpalpebral triangular pattern; VA normal; no deep pain; vessels blanch with 10% phenylephrine (differentiates from scleritis)
- Treatment: Cool compresses; topical steroids (weak, 4× daily 1–2 weeks); topical NSAIDs; occasionally oral ibuprofen; treat the underlying IBD
3B. Scleritis (Less Common, More Serious)
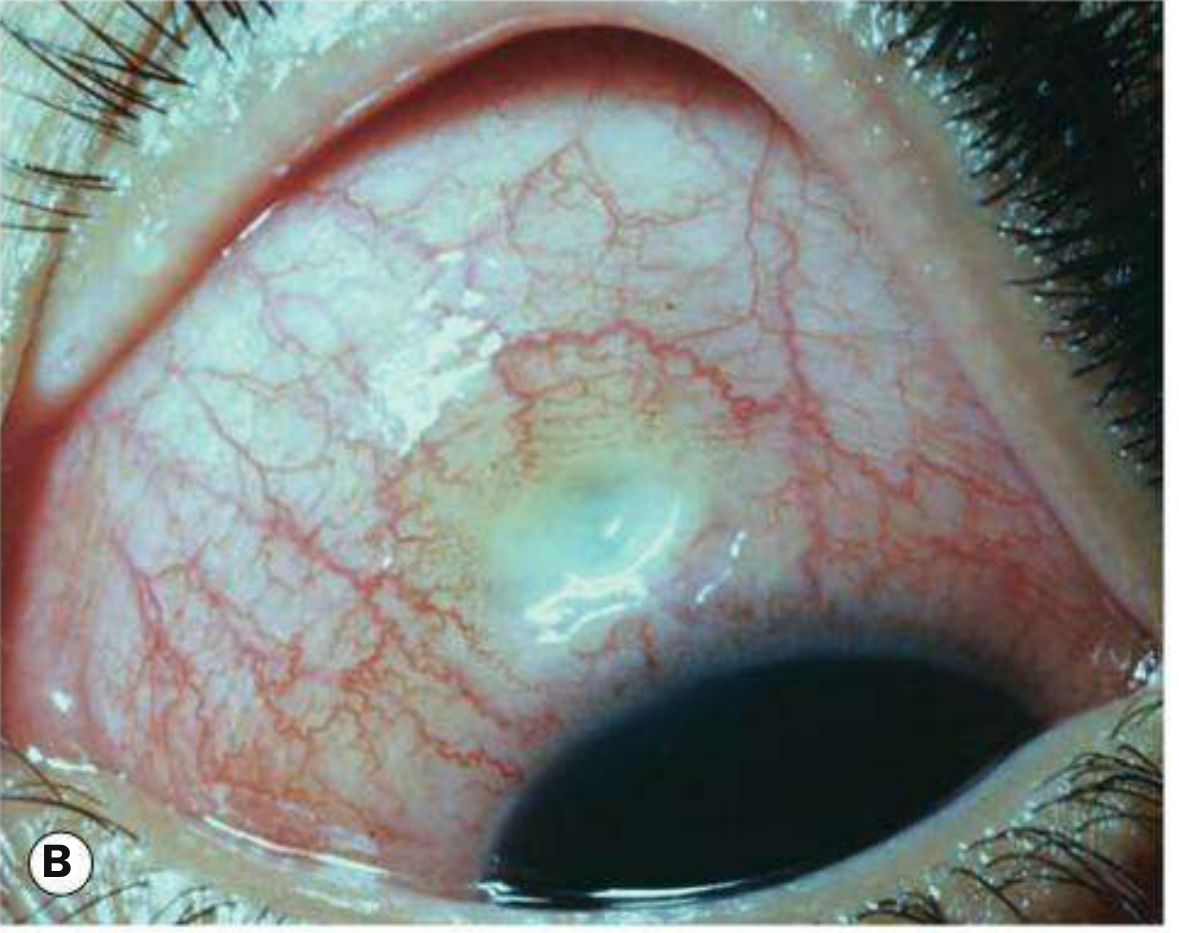
- Involves the deep episcleral and scleral vascular plexus - more painful and potentially vision-threatening
- Types in CD:
- Diffuse non-necrotizing (most common form in IBD)
- Nodular non-necrotizing (see image above - characteristic single or multiple scleral nodules)
- Necrotizing scleritis (rare but most severe; can cause scleromalacia perforans - a painless, silent melting of the sclera)
- Symptoms: Deep boring ache radiating to the brow and temple, worse at night, waking from sleep; photophobia; tearing
- Signs: Deep violaceous hue; vessels do NOT blanch with phenylephrine; globe tenderness on palpation; reduced visual acuity if posterior scleritis
- Scleritis does NOT correlate with bowel activity (unlike episcleritis) - can occur during remission
- Treatment: Oral NSAIDs first-line (indomethacin 25–50 mg TDS); systemic corticosteroids (prednisolone 1 mg/kg/day) for non-necrotizing disease; immunosuppressives (methotrexate, azathioprine, mycophenolate) for recurrent/necrotizing disease; infliximab or adalimumab for refractory cases
3C. Anterior Uveitis (Iridocyclitis)
- Second most common ocular EIM in CD; more common with colonic involvement and HLA-B27 positivity
- Characteristically acute, unilateral, non-granulomatous; can be bilateral in CD (unlike classic ankylosing spondylitis)
- Key clinical point: Uveitis in CD does NOT reliably correlate with bowel activity - it can occur during remission and may even be the presenting feature that leads to IBD diagnosis
- Symptoms: Acute-onset painful red eye; photophobia; blurred vision; circumcorneal (ciliary) injection
- Signs: Keratic precipitates (KP) - fine in non-granulomatous; flare and cells in anterior chamber; posterior synechiae; raised IOP possible
- Marginal keratitis may co-exist: peripheral corneal infiltrates (subepithelial), separated from the limbus by a clear zone
- Complications: Posterior synechiae → irregular pupil; secondary glaucoma; band keratopathy; cataract
- Treatment: Topical steroids + cycloplegics (atropine 1% or cyclopentolate 1%); systemic corticosteroids for severe/bilateral; treat underlying IBD; biologics (infliximab, adalimumab) for refractory - these treat both the bowel and the eye simultaneously
3D. Conjunctival Manifestations
- Keratoconjunctivitis Sicca (Dry Eye Disease): Most common conjunctival finding; significant discomfort though benign; caused by reduced lacrimal gland function and tear film instability driven by chronic systemic inflammation
- Treatment: Preservative-free artificial tears, cyclosporine eye drops (Restasis/Ikervis), punctal plugs
- Non-specific conjunctivitis: Papillary or follicular; often correlates with disease flares
- Conjunctival granulomas: Rare but pathognomonic of CD - non-caseating granulomas on conjunctival biopsy can confirm the diagnosis in atypical cases
3E. Corneal Manifestations
- Marginal keratitis: Peripheral corneal infiltrates (crescent-shaped) separated from the limbus by a clear zone; typically at 4 and 8 o'clock positions; immune complex deposition
- Peripheral Ulcerative Keratitis (PUK): More severe; crescent-shaped ulceration at the peripheral cornea with stromal melting; risk of corneal perforation - requires urgent ophthalmological review; associated with severe active CD; treat with systemic immunosuppression ± anti-TNF therapy
- Exposure keratopathy: If orbital involvement (see 3G below)
3F. Posterior Segment Manifestations
- Less common but important:
- Retinal vasculitis: Periphlebitis (venous sheathing); associated with active severe CD; can cause retinal vein occlusion
- Serous retinal detachment: Rare; associated with severe systemic inflammation
- Optic neuritis: Rare; can be part of severe neurological EIMs of CD; treat with IV methylprednisolone
- Central serous chorioretinopathy: May be drug-related (corticosteroid therapy)
- CMV retinitis: In immunosuppressed CD patients on biologics + immunomodulators (see drug complications section)
3G. Orbital Manifestations
- Orbital inflammatory disease (orbital pseudotumour): Painful proptosis, diplopia, periorbital oedema; non-infective granulomatous inflammation extending to the orbit from adjacent structures or as a direct EIM
- Dacryoadenitis: Lacrimal gland inflammation; rare
4. Relationship Between Ocular EIMs and Bowel Activity
| Ocular EIM | Correlates with Bowel Activity? | More Common in |
|---|---|---|
| Episcleritis | Yes - flares with bowel disease | Colonic CD |
| Scleritis | No - independent | CD > UC |
| Anterior uveitis | No - independent; can precede IBD | CD with HLA-B27, colitis |
| PUK | Yes - severe active disease | Active CD |
| Dry eye | Partial correlation | Both CD and UC |
| Retinal vasculitis | Yes - active disease | Severe CD |
| Conjunctival granulomas | Variable | CD specifically |
5. Drug-Related (Iatrogenic) Ocular Complications
| Drug | Ocular Side Effect | Notes |
|---|---|---|
| Corticosteroids (oral/IV) | Posterior subcapsular cataract | Dose- and duration-dependent |
| Steroid-induced ocular hypertension/glaucoma | Monitor IOP | |
| Indirect: diabetic retinopathy via hyperglycaemia | Long-term use | |
| Central serous chorioretinopathy | ||
| Methotrexate | Conjunctivitis, blepharitis | Ocular surface irritation |
| Anti-TNF-α (infliximab, adalimumab) | Paradoxical uveitis flares in some patients | "Anti-TNF-induced uveitis" - distinct entity; commoner with etanercept than adalimumab/infliximab |
| Demyelinating optic neuritis (rare) | Contraindicate anti-TNF in MS | |
| Opportunistic infections (CMV retinitis, toxoplasma) | In immunosuppressed patients | |
| Vedolizumab (anti-integrin) | May not prevent extra-intestinal uveitis (gut-selective mechanism) | Consider switching to anti-TNF if uveitis develops on vedolizumab |
| Ustekinumab (anti-IL-12/23) | Uveitis risk appears low but data emerging | Limited long-term ocular safety data |
| Aminosalicylates (5-ASA) | Rare: conjunctivitis, episcleritis (hypersensitivity) | |
| Ciclosporin (rescue therapy) | IOP elevation; hirsutism of eyelashes |
6. Treatment Principles
- Mild: Cool compresses, preservative-free artificial tears
- Moderate: Topical steroids (fluorometholone 0.1% QID) or topical NSAIDs
- Treat the underlying CD flare (mesalazine, corticosteroids) - episcleritis will often resolve
- Topical prednisolone acetate 1% (hourly during acute attack, tapering) + topical cycloplegic
- Periocular injection of triamcinolone acetonide if unresponsive
- Systemic prednisolone for bilateral or severe cases
- Methotrexate or azathioprine for recurrent uveitis (steroid-sparing)
- Adalimumab - most evidence for IBD-associated uveitis; dual benefit (bowel + eye)
- Oral indomethacin 25–50 mg TDS or flurbiprofen 100 mg TDS
- Oral prednisolone 1 mg/kg/day for non-NSAID-responsive cases
- Methotrexate, mycophenolate mofetil, or azathioprine for maintenance
- Infliximab or adalimumab for necrotising scleritis
- Urgent: systemic immunosuppression (IV methylprednisolone ± cyclophosphamide)
- Anti-TNF therapy
- Corneal protective contact lens; tectonic glue/graft for perforation risk
- Preservative-free artificial tears hourly; lubricating gels at night
- Topical ciclosporin 0.1% (Ikervis) twice daily for moderate-severe
- Punctal occlusion for severe cases
7. Screening & Monitoring Recommendations
- All newly diagnosed CD patients should have an ophthalmology baseline review
- Patients on long-term corticosteroids: Annual IOP check + slit-lamp for PSC cataract
- Patients starting anti-TNF: Ophthalmology review and education about uveitis symptoms (pain, photophobia, blurred vision) - report immediately
- Patients on hydroxychloroquine (rare in CD): Annual OCT + mfERG for maculopathy
- Active CD with new eye symptoms: Same-day/next-day ophthalmology referral - do not delay
8. Recent Evidence (PubMed 2021–2026)
- Meta-analysis 2022 (Li et al., PMID 36497759): In 190,941 IBD patients, CD carries significantly higher odds of uveitis vs UC (OR 1.60). European CD patients have higher odds of both uveitis and episcleritis.
- Review 2024 (Richardson et al., Biomedicines, PMID 39767762): Comprehensive pathophysiology, epidemiology, and iatrogenic associations; highlights vedolizumab's limitation (gut-selective) in controlling extraintestinal uveitis; recommends integrated gastro-ophthalmology care.
- Review 2024 (Migliorisi et al., Cells, PMID 38247834): Confirms multidisciplinary approach is the backbone of O-EIM management; anti-TNF-α remains first-line biologic for both bowel and uveal disease.
- Systematic Review 2024 (Songel-Sanchis & Cosín-Roger, Diagnostics, PMID 39767176): IBD incidence of ocular EIMs ranges 4–10%; uveitis incidence higher in CD than UC; inadequate routine ophthalmological screening in most IBD centres.
Summary Table – Key Ocular EIMs in Crohn's Disease
| Manifestation | Frequency | Bowel Correlation | Treatment |
|---|---|---|---|
| Episcleritis | Most common | Yes | Topical steroids, treat IBD |
| Anterior uveitis | Common | No | Topical steroids + cycloplegic; adalimumab |
| Scleritis | Uncommon | No | Oral NSAIDs → steroids → biologics |
| Dry eye (KCS) | Common | Partial | Artificial tears, topical ciclosporin |
| Marginal keratitis | Uncommon | Partial | Topical steroids, treat IBD |
| PUK | Rare | Yes | Urgent: systemic steroids + anti-TNF |
| Retinal vasculitis | Rare | Yes | Systemic immunosuppression |
| Orbital disease | Very rare | Variable | Steroids ± surgery |
| Conjunctival granuloma | Very rare | Variable | Pathognomonic; treat IBD |