Prp in orthopaedics 10 mark pg answer with flow chart and images
"platelet-rich plasma"[MeSH Terms] AND "orthopedics"[MeSH Terms]
PRP platelet rich plasma orthopaedics mechanism preparation classification clinical applications 2024
https://pmc.ncbi.nlm.nih.gov/articles/PMC12754507
Medical flowchart diagram showing PRP (Platelet-Rich Plasma) preparation and mechanism of action in orthopaedics. The flowchart should show: Step 1: Blood Collection (20-60 mL venous blood with anticoagulant) → Step 2: First Centrifugation (soft spin 1000-1200 rpm, 10 min) separating Red Blood Cells layer, Buffy coat (platelets + WBC), and Platelet Poor Plasma → Step 3: Second Centrifugation (hard spin 2000-3000 rpm, 15 min) concentrating platelets → Step 4: PRP Product (platelet concentration 3-8x baseline, ~1 million platelets/μL) → Step 5: Activation (thrombin + calcium chloride, or autologous activation at injury site) → Step 6: Growth Factor Release (PDGF, TGF-β, VEGF, IGF-1, EGF, FGF) → Step 7: Clinical Application at target site. Clean professional medical diagram style with blue and red color scheme, labeled boxes with arrows.
Medical classification diagram of PRP (Platelet-Rich Plasma) types used in orthopaedics. Show a 2x2 grid classification table based on two axes: Leukocyte content (Low/High) vs Fibrin architecture (Liquid plasma / Fibrin gel). Four quadrants: 1) P-PRP - Pure Platelet Rich Plasma (low leukocytes, liquid), 2) L-PRP - Leukocyte and Platelet Rich Plasma (high leukocytes, liquid), 3) P-PRF - Pure Platelet Rich Fibrin (low leukocytes, gel), 4) L-PRF - Leukocyte and Platelet Rich Fibrin (high leukocytes, gel). Below show PAW classification boxes: P=Platelet concentration, A=Activation method, W=White blood cell content. Clinical uses column: OA joints prefer LP-PRP, tendons prefer L-PRP. Professional medical diagram, clean colors, clearly labeled.
Medical diagram showing clinical applications of PRP in orthopaedics with anatomical illustrations. A central circle labeled "PRP in Orthopaedics" with radiating arrows to 6 application boxes: 1) Osteoarthritis - knee joint illustration, shows intra-articular injection; 2) Tendinopathy - lateral epicondyle/Achilles tendon illustration, shows peri-tendinous injection; 3) Bone Healing - fracture site with callus, augments non-unions; 4) Ligament/ACL Injuries - knee ligament diagram; 5) Rotator Cuff Repair - shoulder anatomy, reduces retear rate; 6) Cartilage Defects - articular cartilage repair. Each box has a small anatomical icon. Clean medical illustration style, blue and orange color scheme, professional textbook quality.
PLATELET-RICH PLASMA (PRP) IN ORTHOPAEDICS
Definition
Composition
| Component | Role |
|---|---|
| Platelets (>4 × 10⁵/μL) | Source of growth factors |
| Alpha granules | Contain PDGF, TGF-β, IGF-1, VEGF, EGF |
| Dense granules | Contain serotonin, ADP, calcium |
| Plasma proteins | Fibrin scaffold, fibronectin, vitronectin |
Preparation - Step-by-Step Flowchart
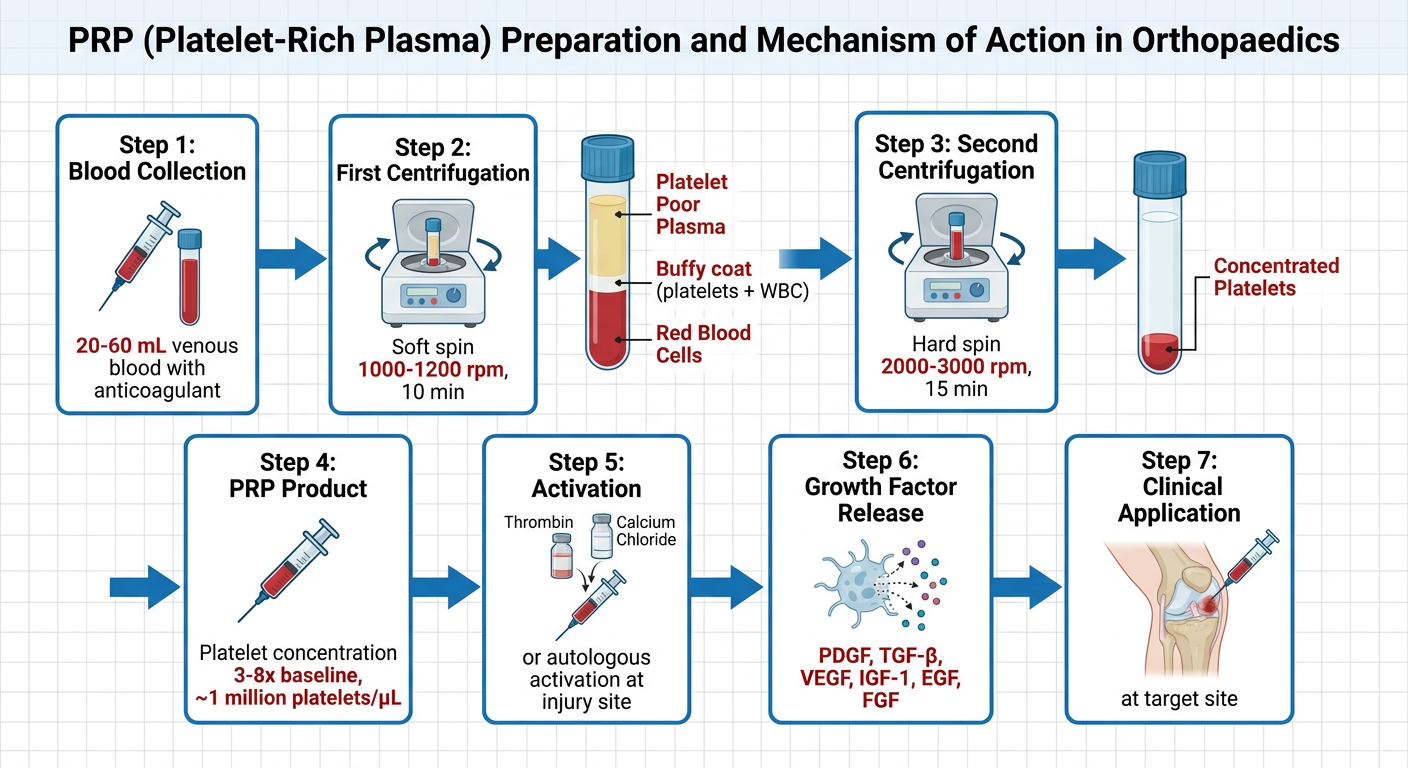
- Blood Collection - 20-60 mL venous blood collected into ACD (Acid Citrate Dextrose) anticoagulant tubes
- First Centrifugation (Soft Spin) - 1000-1200 rpm for 8-10 min
- Separates: Red cell layer (bottom) + Buffy coat (platelets + WBC) + Platelet-poor plasma (top)
- Plasma Transfer - Buffy coat + upper plasma carefully aspirated
- Second Centrifugation (Hard Spin) - 2000-3000 rpm for 10-15 min
- Concentrates platelets into pellet
- Resuspension - Supernatant discarded, pellet resuspended in small plasma volume (~3-8 mL)
- Activation - Optional external activation with thrombin + CaCl₂, or left for autologous activation at injection site
Classification of PRP
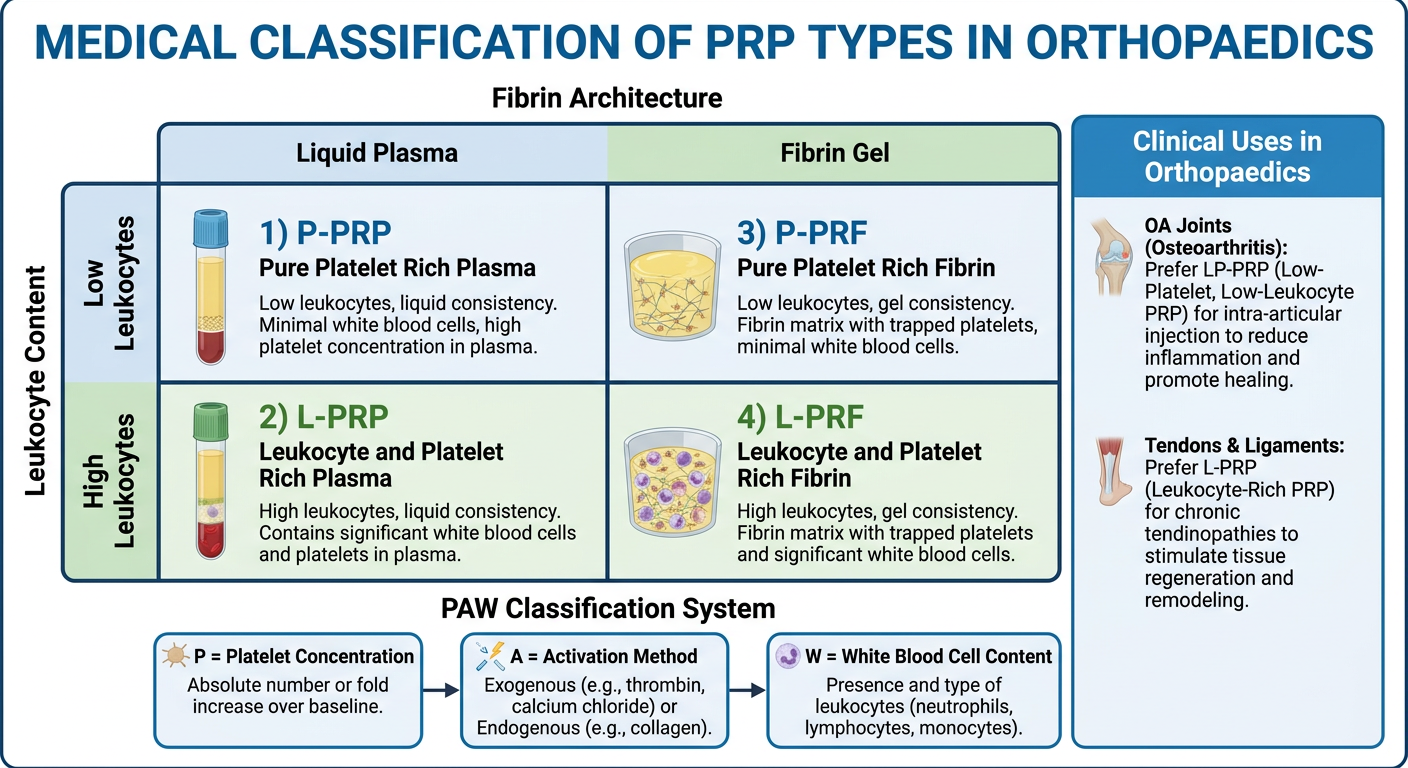
Dohan Ehrenfest Classification (4 Families):
| Type | Leukocytes | Fibrin | Example |
|---|---|---|---|
| P-PRP (Pure Platelet-Rich Plasma) | Absent | Liquid | PRGF-Endoret |
| L-PRP (Leukocyte-PRP) | Present | Liquid | Biomet GPS, ACP |
| P-PRF (Pure Platelet-Rich Fibrin) | Absent | Gel/Membrane | Fibrinet |
| L-PRF (Leukocyte-PRF) | Present | Gel/Membrane | Intra-Spin L-PRF |
PAW Classification (Delong et al.):
- P = Platelet concentration (absolute count)
- A = Activation method (exogenous/autologous)
- W = White blood cell content (above/below baseline)
Mechanism of Action
Platelet Activation
↓
Alpha-granule degranulation
↓
Growth Factor Release
├── PDGF (Platelet-Derived GF) → Cell proliferation, collagen synthesis, chemotaxis
├── TGF-β (Transforming GF-β) → ECM production, cartilage repair
├── VEGF (Vascular Endothelial GF) → Angiogenesis, neovascularization
├── IGF-1 (Insulin-like GF-1) → Cell proliferation, bone mineralization
├── EGF (Epidermal GF) → Fibroblast proliferation
└── FGF (Fibroblast GF) → Wound healing
↓
├── Tissue Regeneration
├── Anti-inflammation (↑M2 macrophages, ↓IL-1, TNF-α)
├── Analgesia (serotonin from dense granules)
└── Antimicrobial effect
Clinical Applications in Orthopaedics
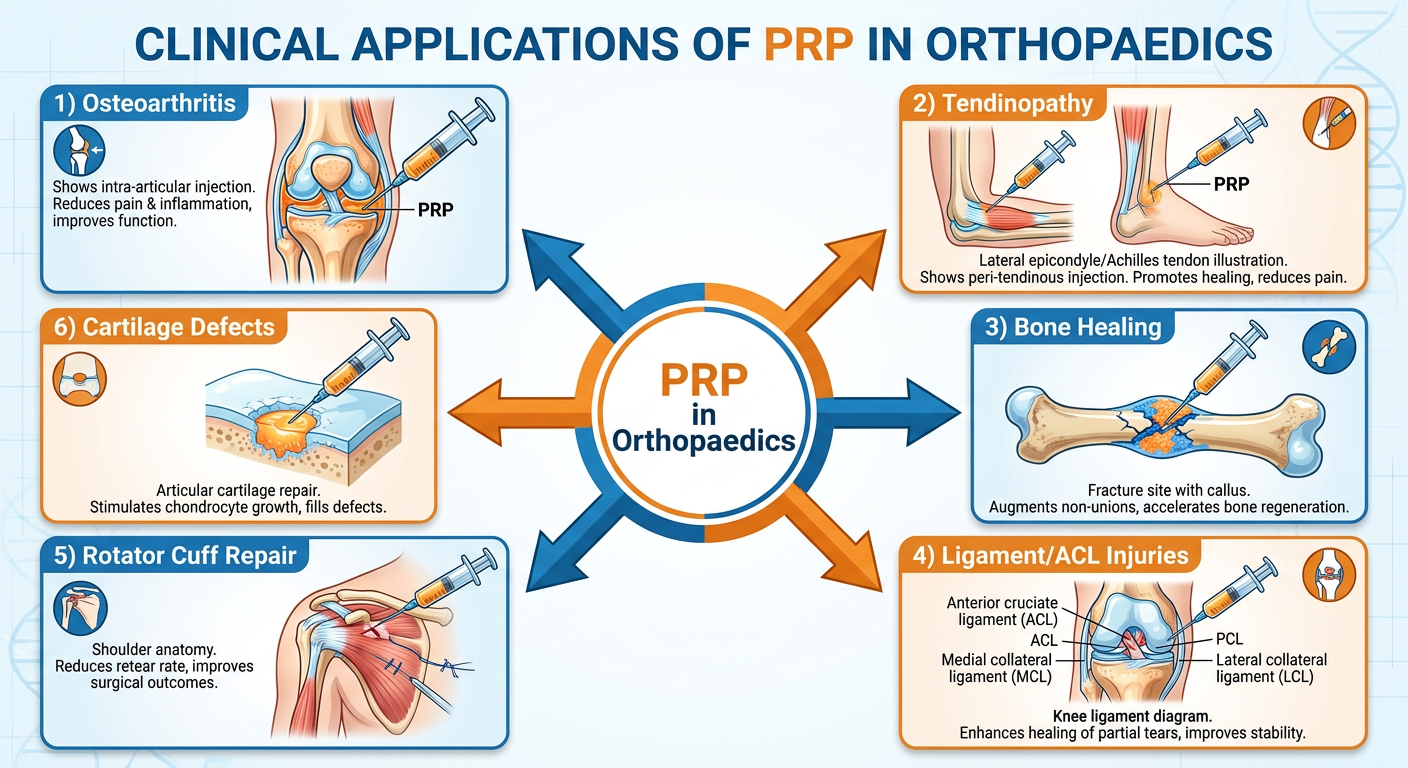
1. Osteoarthritis (OA)
- Knee OA: Intra-articular PRP injection; improves pain and function, particularly in early-to-moderate OA (Grade I-II Kellgren-Lawrence); L-PRP preferred
- Mechanism: inhibits synoviocyte activation, reduces IL-1β and TNF-α, promotes chondrocyte survival
- Evidence: Meta-analyses show superiority over hyaluronic acid at 3-6 months
2. Tendinopathies
- Lateral epicondylitis (Tennis Elbow): Peri-tendinous injection; most robust evidence
- Patellar tendinopathy, Achilles tendinopathy: Ultrasound-guided intratendinous injection
- Rotator Cuff: Adjunct to arthroscopic repair; a 2024 RCT (Rossi et al.) showed reduced retear rate from 34.1% to 15.2% with LP-PRP
- Mechanism: Promotes tenocyte proliferation, collagen type-I synthesis, neovascularization
3. Bone Healing
- Fracture non-unions and delayed unions: PRP applied at fracture site (open or percutaneous)
- Bone grafts: PRP mixed with autograft or allograft to improve osteogenesis
- Mechanism: PDGF and TGF-β stimulate osteoblast proliferation; VEGF enhances revascularization
4. Ligament Injuries
- ACL/PCL tears: Adjunct in reconstruction (applied at graft-tunnel interface)
- Medial collateral ligament sprains: Accelerates healing in partial tears
- Mechanism: Fibroblast activation, collagen remodeling
5. Cartilage Defects
- Osteochondral lesions: Combined with microfracture or as standalone injection
- Adjunct to ACI (Autologous Chondrocyte Implantation)
6. Spine
- Degenerative disc disease, facet joint injections
- Lumbar disc pathologies (emerging evidence)
Contraindications
| Absolute | Relative |
|---|---|
| Thrombocytopenia (<100,000/μL) | NSAIDs use (stop 1 week prior) |
| Active infection at site | Corticosteroid use |
| Platelet dysfunction syndromes | Smoking |
| Anticoagulant therapy | Anemia |
| Active malignancy |
Advantages & Limitations
- Autologous - minimal immunogenic risk
- Minimally invasive, day-care procedure
- Multiple growth factors delivered simultaneously
- No risk of disease transmission
- No standardized preparation protocol
- Large inter-individual variation in platelet yield
- Variable clinical outcomes due to heterogeneous formulations
- Cost - not universally covered by insurance
- Limited high-quality RCT evidence in several indications
Recent Evidence (2024-2026)
- Rossi et al. 2024 showed LP-PRP as adjuvant to rotator cuff repair reduced retear rates significantly (15.2% vs 34.1%)
- A 2026 systematic review (PMID: 41290406) highlights poor standardization in lumbar disc PRP studies, underscoring need for MIBO guideline adherence
- Leukocyte-poor PRP (LP-PRP) is now preferred for intra-articular use (joint spaces) while leukocyte-rich PRP (LR-PRP) is preferred for tendons and ligaments
Summary Table
| Parameter | Details |
|---|---|
| Source | Autologous venous blood |
| Platelet target | ≥ 1 × 10⁶ platelets/μL (3-8× baseline) |
| Preparation | Double centrifugation (soft spin + hard spin) |
| Key growth factors | PDGF, TGF-β, VEGF, IGF-1, EGF, FGF |
| Best evidence | Knee OA, lateral epicondylitis, rotator cuff augmentation |
| Preferred type (joints) | LP-PRP (leukocyte-poor) |
| Preferred type (tendons) | LR-PRP (leukocyte-rich) |
| Frequency of injection | 1-3 injections, 2-4 weeks apart |
- PRP platelet count must be >4 × 10⁵/μL to be called PRP
- "Optimal" platelet concentration is ~1 million/μL (5× baseline)
- L-PRP is pro-inflammatory (suitable for tendons/ligaments); P-PRP is anti-inflammatory (suitable for joints/cartilage)
- PAW classification is the most clinically practical system
- PRP does NOT replace surgery - it is an adjunct or used in early/mild disease