Dka patient with potassium 2.8
Reading File
Finding Sources
Searching PubMed
"diabetic ketoacidosis" AND "hypokalemia" AND potassium replacement
Finding Sources
Searching PubMed
"diabetic ketoacidosis" AND potassium AND management
Reading File
Reading File
Reading File
Loading Image
Here is a focused breakdown of managing a DKA patient with K+ of 2.8 mEq/L:
DKA with Hypokalemia (K+ 2.8 mEq/L) - Management
Why This Is Dangerous
In DKA, total body potassium is always severely depleted (losses up to 7 mmol/kg) due to osmotic diuresis, vomiting, and intracellular shifts from acidosis. The serum K+ can appear normal or even high initially because acidosis drives K+ out of cells. A presenting K+ of 2.8 means total body depletion is profound - the true deficit is far worse than the number suggests.
When insulin is started, it rapidly drives potassium back into cells. Without correcting hypokalemia first, this will cause life-threatening arrhythmias and respiratory muscle paralysis.
Step-by-Step Management
1. HOLD INSULIN - Do Not Start Until K+ ≥ 3.3-3.5 mEq/L
"Do not give insulin until potassium is 3.3 mEq/L or greater." - Rosen's Emergency Medicine
2. Aggressive IV Potassium Replacement
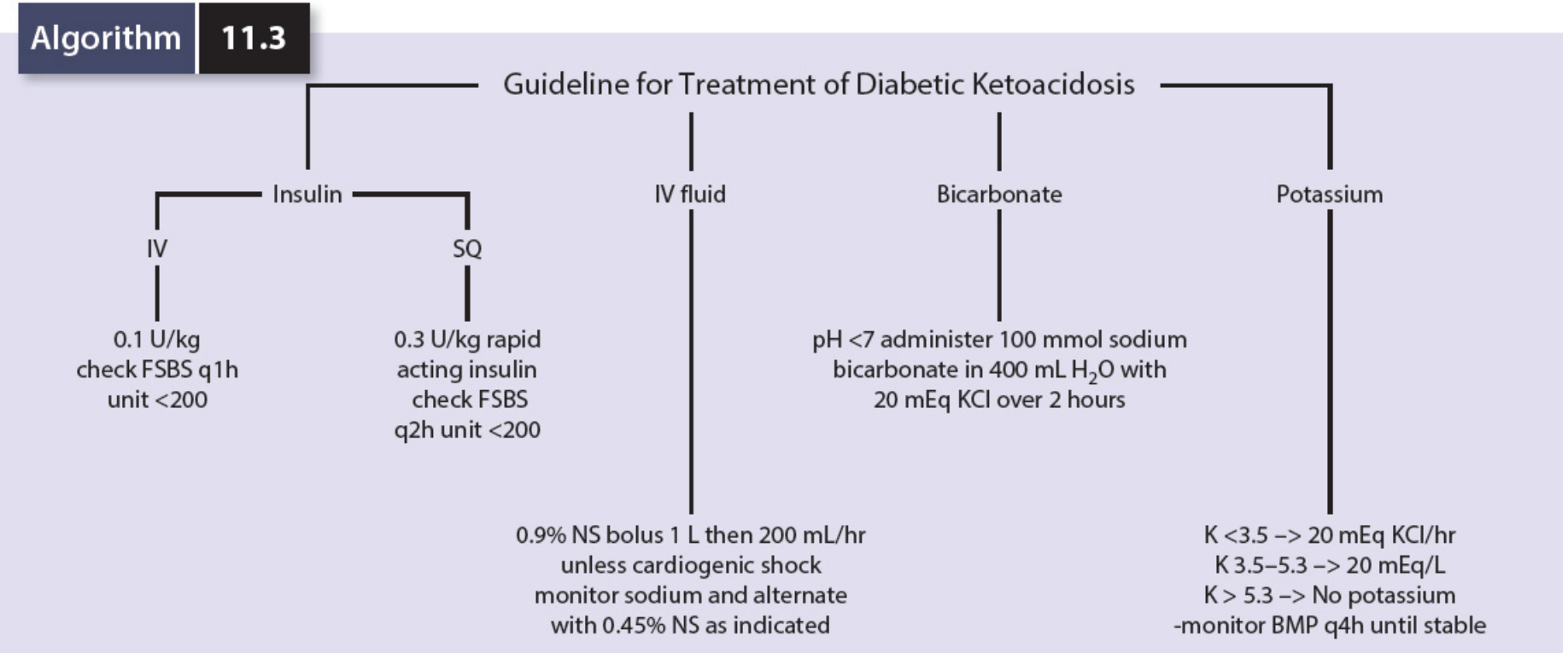
Per the DKA treatment algorithm (Mulholland & Greenfield's Surgery, Algorithm 11.3):
| Serum K+ | Action |
|---|---|
| < 3.5 mEq/L (your patient) | 20 mEq KCl/hr IV |
| 3.5-5.3 mEq/L | 20 mEq/L added to each IV bag |
| > 5.3 mEq/L | No potassium; monitor BMP q4h |
- Administer KCl 20-40 mEq/hour IV via a large peripheral or central line
- Recheck K+ every 1-2 hours
- Only start insulin once K+ is confirmed ≥ 3.3-3.5 mEq/L
3. IV Fluids - Start Immediately (Do Not Wait)
Fluid resuscitation should begin right away regardless of K+ status:
- 0.9% Normal Saline - 2-4 L in the first 2-4 hours
- Bolus 1 L NS, then 200 mL/hr
4. Once K+ ≥ 3.3-3.5 mEq/L - Start Insulin
- Fixed-rate IV insulin infusion: 0.1 units/kg/hour regular insulin
- Continue potassium supplementation: add 20-40 mEq KCl to each liter of IV fluid as long as K+ < 5.5 mEq/L and the patient is making urine
- Monitor K+ every 1-2 hours once insulin is running
5. When Glucose Drops to ≤ 250-300 mg/dL
- Switch IV fluid to D5W/0.45% NS or add 10% dextrose to the fluid regimen
- Reduce insulin infusion to 0.05 units/kg/hour once glucose <250 and ketones <1.0 mmol/L
6. Other Electrolytes to Monitor
- Magnesium - correct with 1-2 g MgSO4 IV (hypomagnesemia worsens potassium repletion)
- Phosphate - replace only if < 1.0 mg/dL with symptoms
- Bicarbonate - not usually indicated; consider only if pH < 7.0
7. Continuous Monitoring
- Serum K+, glucose, bicarbonate, anion gap every 1-2 hours
- ECG monitoring (look for flattened T waves, U waves, prolonged QT from hypokalemia)
- Strict fluid balance with urine output tracking
Summary: Priorities in Order
- IV fluids (NS) - start now
- IV KCl replacement - start now (20 mEq/hr)
- Recheck K+ in 1-2 hours
- Start insulin only when K+ ≥ 3.3 mEq/L
- Continue K+ supplementation throughout insulin therapy
Sources: Rosen's Emergency Medicine (9e), Goldman-Cecil Medicine, Mulholland & Greenfield's Surgery (7e), Comprehensive Clinical Nephrology (7e)
This is a shared conversation. Sign in to Orris to start your own chat.