How to write provisional diagnosis for each clinical finding in oral cavity in oral medicine in general op
provisional diagnosis oral cavity lesions oral medicine general OPD clinical findings
https://assets.ctfassets.net/u2qv1tdtdbbu/5fow2rTLLJwzQmR2MB…
How to Write a Provisional Diagnosis for Oral Cavity Findings in Oral Medicine (General OPD)
What Is a Provisional Diagnosis?
"Provisional Diagnosis: [Most likely condition], possibly [differential 1] / [differential 2]"
- Most likely diagnosis
- Second possibility
- Third possibility (rule out)
The Framework: How to Arrive at a Provisional Diagnosis
Step 1 - Characterize the Lesion
| Feature | What to Assess |
|---|---|
| Color | White, red, red-white mixed, brown/black, blue, normal |
| Surface texture | Smooth, rough, papillary, verrucous, ulcerated, crusted |
| Consistency | Soft, firm, hard, fluctuant, rubbery |
| Base | Pedunculated, sessile, flat, depressed |
| Border | Well-defined, ill-defined, raised, rolled, undermined |
| Size | In cm (measured or estimated) |
| Site | Exact anatomic location |
| Number | Single vs. multiple |
| Can it be wiped off? | Removable = fungal/debris; Non-removable = keratotic/mucosal |
| Associated features | Ulceration, bleeding, induration, lymphadenopathy |
Step 2 - Take a Focused History
- Onset (sudden vs. gradual), duration
- Pain (spontaneous, on eating/talking, burning)
- Change in size
- Habit history: tobacco (smoke/smokeless), alcohol, areca nut, pan masala
- Trauma history (sharp tooth, denture, biting)
- Systemic illness (diabetes, immunocompromise, HIV, anemia)
- Drug history (NSAIDs, ACE inhibitors, phenytoin, amlodipine)
- Recurrence
Step 3 - Correlate Finding + History = Provisional Diagnosis
Clinical Findings and Their Provisional Diagnoses
A. WHITE LESIONS
| Clinical Finding | Provisional Diagnosis | Key Differentials |
|---|---|---|
| White patch, non-scrapable, lateral tongue/buccal mucosa, smoker | Leukoplakia (homogeneous) | Frictional keratosis, lichen planus |
| White patch, non-scrapable, speckled/nodular, high-risk site (floor of mouth, ventral tongue) | Erythroleukoplakia / Proliferative verrucous leukoplakia | Erythroplakia, squamous cell carcinoma |
| White, curd-like plaques, scrapable, leaves erythematous base | Pseudomembranous candidiasis (oral thrush) | Burnt food debris, diphtheria |
| White lacy/reticular lines, bilateral buccal mucosa, middle-aged adult | Oral lichen planus (reticular type) | Lichenoid drug reaction, frictional keratosis |
| White patch at mucosa, following tobacco pouch site, limited mouth opening | Oral submucous fibrosis (OSMF) | Scleroderma, OSMF + carcinoma |
| White thick plaques on buccal mucosa, bilateral, folded/corrugated, non-scrapable | White sponge nevus | Leukoedema (disappears on stretching), hereditary benign intraepithelial dyskeratosis |
| White lesion on buccal mucosa that disappears when stretched | Leukoedema | Normal variant |
| Hairy white projections, lateral tongue, HIV patient | Oral hairy leukoplakia | Candidiasis, frictional keratosis |
"Non-homogeneous white patch, 2x1.5 cm, at right buccal mucosa, non-scrapable, patient with 15-year tobacco chewing history. Provisional diagnosis: Oral leukoplakia (non-homogeneous type), Rule out early squamous cell carcinoma."
B. RED/ERYTHEMATOUS LESIONS
| Clinical Finding | Provisional Diagnosis | Key Differentials |
|---|---|---|
| Bright red velvety patch, floor of mouth/ventral tongue, cannot be scraped, painless | Erythroplakia | Early SCC, candidiasis (atrophic) |
| Red burning mucosa, denture wearer, atrophic/erythematous | Denture stomatitis (atrophic candidiasis) | Contact allergy to denture material |
| Intense red erythema with white patches, burning, diabetic/immunocompromised | Erythematous candidiasis | Erythroplakia |
| Patchy red depapillation on dorsal tongue | Median rhomboid glossitis / Atrophic glossitis | Erythematous candidiasis, B12/iron deficiency |
| Map-like erythematous patches with white borders, moves over time | Benign migratory glossitis (geographic tongue) | Psoriatic tongue, early lichen planus |
| Red inflamed gingiva, generalized, not resolving with scaling | Plasma cell gingivitis / Desquamative gingivitis | Drug-induced gingivitis, leukemic infiltration |
C. ULCERATIVE LESIONS
| Clinical Finding | Provisional Diagnosis | Key Differentials |
|---|---|---|
| Small round painful ulcer (<1 cm), recurrent, movable mucosa, heals without scar | Minor recurrent aphthous stomatitis (RAS) | Herpetiform ulcers, traumatic ulcer |
| Large painful ulcer (>1 cm), persists 2-6 weeks, single, heals with scar | Major aphthous ulcer (Sutton's disease) | SCC, traumatic ulcer |
| Multiple tiny (<3 mm) ulcers in crops, movable mucosa, exquisitely painful | Herpetiform aphthous stomatitis | Primary herpetic gingivostomatitis |
| Multiple vesicles rupturing to ulcers, gingivitis, fever, child/young adult | Primary herpetic gingivostomatitis | Hand-foot-mouth disease, erythema multiforme |
| Single painless ulcer with indurated (hard) margins, non-movable mucosa | Squamous cell carcinoma | Traumatic ulcer, major aphthous |
| Ulcer with sloping margins, coinciding with sharp tooth/denture flange | Traumatic ulcer | Minor aphthous, SCC |
| Multiple erosions/ulcers after drug exposure, target lesions on skin | Erythema multiforme / Stevens-Johnson syndrome | Pemphigus, pemphigoid |
| Large irregular erosions, Nikolsky sign positive, older adult | Pemphigus vulgaris | Mucous membrane pemphigoid, erosive lichen planus |
| Desquamative erosions, mainly gingiva, tense blisters | Mucous membrane pemphigoid | Pemphigus vulgaris, erosive LP |
D. PIGMENTED LESIONS
| Clinical Finding | Provisional Diagnosis | Key Differentials |
|---|---|---|
| Diffuse brown pigmentation, buccal mucosa, gingiva, racial variation | Physiologic (racial) melanosis | Addison's disease, drug-induced |
| Focal dark blue-gray patch, near amalgam restoration | Amalgam tattoo | Melanocytic nevus, oral melanoma |
| Black/brown macule on gingiva or hard palate, diffuse, patient on antimalarials/minocycline | Drug-induced pigmentation | Racial pigmentation, heavy metal |
| Irregular dark brown/black macule, changing, solitary | Oral melanoma (rule out) | Amalgam tattoo, melanocytic nevus |
| Diffuse gingival/buccal brownish pigmentation + systemic symptoms (fatigue, hypotension) | Addison's disease | Racial pigmentation |
E. SWELLINGS / LUMPS
| Clinical Finding | Provisional Diagnosis | Key Differentials |
|---|---|---|
| Soft, sessile, pink, smooth swelling on buccal mucosa/tongue, non-tender | Fibroma (irritation fibroma) | Lipoma, neurofibroma |
| Soft, pedunculated, papillary/finger-like projection, white | Squamous papilloma (HPV) | Verruca vulgaris, condyloma acuminatum |
| Soft, translucent, fluctuant swelling, floor of mouth | Ranula (mucous retention cyst) | Dermoid cyst, sublingual salivary gland tumor |
| Hard nodular swelling, palate or buccal mucosa, along midline/alveolar ridge | Torus palatinus / Torus mandibularis | Bony exostosis, osteoma |
| Firm, slowly enlarging swelling, hard palate, painless | Pleomorphic adenoma (minor salivary gland) | Mucoepidermoid carcinoma, Adenoid cystic carcinoma |
| Fluctuant red swelling near tooth with caries, tender, soft | Periapical abscess / Dentoalveolar abscess | Cellulitis, infected cyst |
| Firm gingival swelling, pregnancy / phenytoin / amlodipine use | Drug-induced gingival overgrowth / Pregnancy epulis | Hereditary gingival fibromatosis |
| Red pedunculated gingival swelling, bleeds on touch, pregnancy | Pyogenic granuloma (pregnancy epulis) | Peripheral giant cell granuloma, fibroma |
| Purple/blue compressible swelling on lip or tongue, blanches on pressure | Hemangioma / Vascular malformation | Varix, mucocele |
| Blue-domed, soft, fluctuant swelling on lower lip, traumatic history | Mucocele | Mucous retention cyst, hemangioma |
F. BONE / GINGIVAL LESIONS
| Clinical Finding | Provisional Diagnosis | Key Differentials |
|---|---|---|
| Red sessile firm swelling on gingiva, bleeds on probing, radiograph shows bone erosion | Peripheral giant cell granuloma | Pyogenic granuloma, peripheral ossifying fibroma |
| Painless expansion of jaw, multilocular radiolucency on X-ray, young patient | Ameloblastoma | Odontogenic keratocyst, dentigerous cyst |
| Painless jaw swelling + "soap-bubble" X-ray appearance | Ameloblastoma / Aneurysmal bone cyst | Central giant cell granuloma |
| Peau d'orange appearance of skin over jaw + fixed lymph nodes | Squamous cell carcinoma | Osteosarcoma, lymphoma |
Standard Format for Writing Provisional Diagnosis in Case Sheet
CLINICAL FINDINGS:
Site: [exact location]
Size: [dimensions in cm]
Shape: [regular/irregular]
Color: [white/red/normal/mixed]
Surface: [smooth/rough/papillary/ulcerated]
Margin: [well-defined/ill-defined; raised/flat]
Base: [sessile/pedunculated]
Consistency: [soft/firm/hard/fluctuant]
Tenderness: [present/absent]
Lymph nodes: [palpable/not palpable; mobile/fixed]
PROVISIONAL DIAGNOSIS:
1. [Most likely diagnosis] — based on [key feature]
2. Rule out [differential 1] — due to [feature]
3. Rule out [differential 2] — due to [feature]
INVESTIGATIONS ADVISED:
- [Incisional biopsy / Exfoliative cytology / Blood work / Radiograph]
Quick Mnemonic for Approaching Any Lesion: "SCABBED"
- S - Site (exact location)
- C - Color
- A - Associated features (pain, ulcer, lymph nodes)
- B - Border / Base
- B - Background history (habits, systemic disease)
- E - Evolution (duration, change)
- D - Diagnosis (most likely first, then differentials)
Important Principles for Writing Provisional Diagnoses
- Most dangerous diagnosis first - If there is any clinical suspicion of malignancy (indurated ulcer, non-healing lesion, lymphadenopathy), list carcinoma/SCC as "rule out" even if less likely.
- Basis must be stated - Always write why you favor that diagnosis: "based on non-scrapable white patch in a tobacco chewer."
- Never write just one diagnosis without differentials, except for clearly benign/classical presentations (e.g., mucocele of lower lip with classic history).
- Habit history changes everything - The same white patch in a non-smoker (rule out candidiasis) vs. a 20-year tobacco chewer (rule out dysplasia/carcinoma) carries very different provisional diagnoses.
- Can it be wiped off? - This single question separates pseudomembranous candidiasis (removable) from all keratotic white lesions (non-removable).
- Nikolsky sign - Positive = mucocutaneous blistering disease (pemphigus, pemphigoid, erythema multiforme).
- Induration = red flag - Any indurated oral lesion warrants "rule out squamous cell carcinoma" regardless of other features.
How to differentiate pit and fissure, decay and deep dental decay , and gross decay with images
pit fissure decay vs deep decay vs gross decay dental caries classification differentiation images
pit fissure caries deep caries gross caries clinical photos radiograph differentiation ICDAS
gross caries vs deep caries clinical appearance pulp involvement symptoms tooth decay stages images dental
Differentiating Pit & Fissure Decay, Deep Decay, and Gross Decay
The Big Picture: Stages of Tooth Decay

1. Pit and Fissure Decay (Early/Moderate Caries)
What it is
The key anatomy
Clinical features
| Feature | Finding |
|---|---|
| Color | Brown/dark staining in fissure; chalky white (demineralization) around fissure edges |
| Surface | Fissure appears discolored or darkened; may or may not be cavitated |
| Cavity | Small or no visible hole - the lesion may be much larger internally than it appears |
| Consistency on probing | Softened/sticky fissure (though a sticky probe alone does NOT diagnose caries) |
| Pain | Mild or none; slight sensitivity to cold/sweet may occur |
| Tooth structure | Largely intact; no gross breakdown |
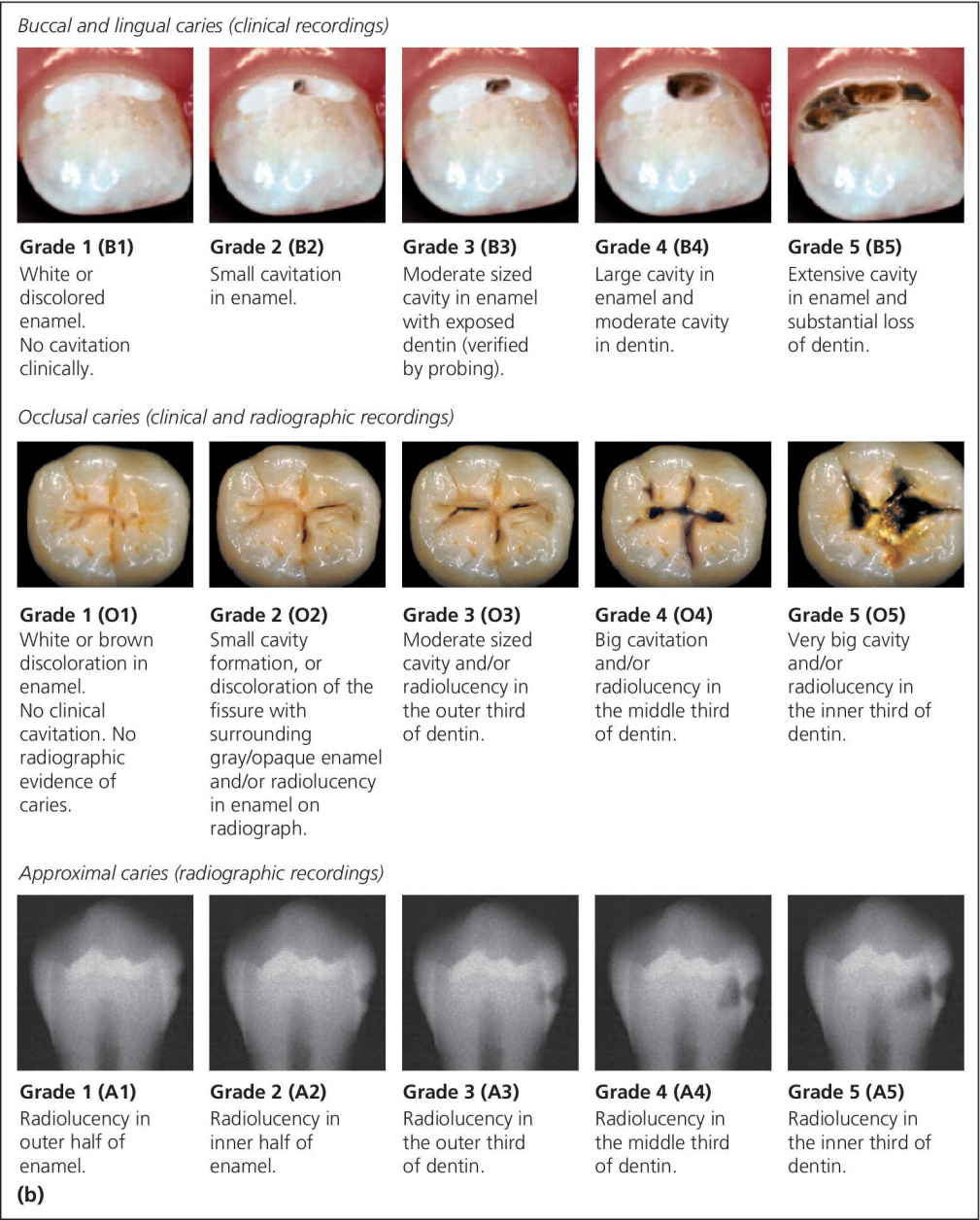
| Radiograph | Early: no radiolucency. Moderate: radiolucency in enamel or outer 1/3 of dentin |
The critical clinical clue
"Iceberg lesion" - The external appearance is deceptively small. Once you open the cavity, it has spread laterally at the DEJ and is much wider inside. Never judge pit/fissure caries by its surface appearance alone.
Visual Reference: Occlusal Caries Grades (Clinical + Radiographic)
2. Deep Dental Decay (Deep Caries / Deep Dentinal Caries)
What it is
Clinical features
| Feature | Finding |
|---|---|
| Color | Dark brown to black discoloration; soft yellow/light brown infected dentin inside |
| Surface | Visible cavity - often moderate sized hole |
| Consistency | Soft/leathery dentin (infected outer layer) over harder but affected inner dentin |
| Pain | Significant - sharp pain to cold, sweet, and hot; pain may linger briefly but NOT spontaneous |
| Pulp vitality | Tooth is still vital; positive response to cold test |
| Radiograph | Radiolucency extending into the inner 1/3 to pulpal quarter of dentin but a clear band of dentin is still visible between the decay and pulp chamber |
| Key distinction | Pain is provoked (stimulus-dependent), NOT spontaneous. No swelling, no sinus tract |
Histological zones in deep caries dentin (from outer to inner):
- Necrotic/infected zone - soft, black/dark brown, full of bacteria - MUST be removed
- Contaminated zone - soft, lightly colored, bacteria present - debatable removal
- Demineralized/affected zone - leathery, few bacteria, CAN be remineralized - preserve if possible
- Translucent zone - firm, reparative dentin, sclerotic - closest to pulp - NEVER probe this
3. Gross Decay (Rampant / Extensive Caries)
What it is
Clinical features
| Feature | Finding |
|---|---|
| Color | Dark brown to black; may appear yellow-green if chronic |
| Surface | Large, open cavitation; significant loss of tooth structure |
| Consistency | Soft, mushy debris; frank pus if necrotic |
| Tooth structure | Crown largely or completely destroyed; may be reduced to a root stump |
| Pain | Often spontaneous, throbbing, continuous pain (irreversible pulpitis or pulp necrosis); OR paradoxically NO pain if pulp is necrotic |
| Pulp vitality | Negative response to cold/electric pulp test (necrosis) or exaggerated prolonged response (irreversible pulpitis) |
| Periapical signs | Tenderness to percussion, sinus tract, swelling, abscess |
| Radiograph | Radiolucency involving the entire pulp chamber and/or periapical rarefaction |
| Common in | Nursing bottle caries (children), xerostomia, methamphetamine use ("meth mouth"), radiation-induced xerostomia, neglected patients |
Side-by-Side Comparison Table
| Feature | Pit & Fissure Decay | Deep Dental Decay | Gross Decay |
|---|---|---|---|
| Depth | Enamel to outer/mid dentin | Inner 1/3 dentin, near pulp | Pulp involved or destroyed |
| Cavity size | Small opening, large internally | Moderate visible cavity | Large, crown destruction |
| Color | Brown stain, chalky white | Dark brown/black | Black, necrotic debris |
| Pain | Mild or none | Cold/sweet pain, provoked, brief | Spontaneous throbbing OR painless (necrosis) |
| Pulp vitality | Vital, normal response | Vital, may be hyperreactive | Absent (necrosis) or irreversible |
| Probing | Softened fissure | Soft/leathery dentin | Soft cavity with open pulp |
| Radiograph | No change to enamel radiolucency | Dentin radiolucency, thin pulp wall | Pulp involvement, periapical lesion |
| X-ray appearance | Normal or enamel shadow | Radiolucency stops before pulp | Radiolucency into/through pulp |
| Treatment | Composite/GIC filling ± sealant | Selective caries removal, indirect pulp cap, restoration | RCT or extraction |
| Emergency? | No | Usually no (unless acute pulpitis) | Often yes |
Tooth Decay Types by Surface Location

Key Differentiating Tests in the Clinic
1. Cold Test (Vitality)
- Pit/fissure caries: Normal brief response
- Deep caries: Sharp pain, fades within 5-10 seconds
- Gross/necrotic: No response (necrosis) or prolonged agonizing pain (irreversible pulpitis)
2. Percussion Test
- Pit/fissure: Negative
- Deep caries: Usually negative
- Gross/periapical: Positive (tender to tap) = periapical involvement
3. Radiograph (Bitewing for early; Periapical for deep/gross)
- Bitewing: best for detecting pit/fissure and approximal caries in dentin
- Periapical: needed for deep/gross to assess pulp and periapex
4. Probe Consistency
- Hard/resistant = sound enamel
- Slightly softened = early dentin caries
- Very soft/mushy = infected dentin (necrotic zone)
5. ICDAS Score Summary
| ICDAS Code | Clinical Description | Corresponds To |
|---|---|---|
| 0 | Sound | No caries |
| 1 | White/brown in dry fissure | Pit/fissure - initial |
| 2 | White/brown visible when wet | Pit/fissure - early enamel |
| 3 | Localized enamel breakdown | Pit/fissure - cavitated enamel |
| 4 | Underlying dark shadow | Dentin caries (moderate) |
| 5 | Cavity with visible dentin | Deep caries |
| 6 | Extensive cavity, >50% of surface | Gross/extensive caries |
Quick Clinical Memory Aid
PIT/FISSURE: Small dark stain, no/mild pain, vital tooth → FILL IT
"Small outside, big inside"
DEEP CARIES: Moderate cavity, cold pain (brief), vital → SELECTIVE
REMOVAL + indirect pulp cap + RESTORE
GROSS DECAY: Large destruction, spontaneous pain OR no pain,
periapical changes → RCT or EXTRACT
If I do mba after bds in iim colleges in India what would bey salary at begening
IIM MBA salary 2024 2025 placement average package IIM Ahmedabad Bangalore Calcutta
BDS MBA healthcare management salary India 2024 2025 IIM healthcare consulting
BDS MBA IIM career options healthcare management hospital administration pharma salary India
BDS + MBA from IIM - Starting Salary in India (2025-26 Data)
Important reality upfront
IIM Placement Data (2025) - What Freshers Actually Earn
| IIM | Average Starting Package | Highest Package |
|---|---|---|
| IIM Ahmedabad | ₹29-30 LPA | ₹1.46 CPA |
| IIM Bangalore | ₹35.31 LPA | ₹1.15 CPA |
| IIM Calcutta | ₹34.23 LPA | ₹1.45 CPA |
| IIM Lucknow | ₹32.2 LPA | ₹1.23 CPA |
| IIM Kozhikode | ₹28 LPA | ₹72 LPA |
| IIM Indore | ₹25.68 LPA | ₹1 CPA |
| IIM Mumbai | ₹34.5 LPA (median) | ₹71.4 LPA |
| IIM Udaipur / Raipur | ₹18-19 LPA | ₹42-48 LPA |
What BDS + IIM MBA Opens For You Specifically
1. Management Consulting (Healthcare Practice)
- Starting salary at MBB (McKinsey/BCG/Bain): ₹28-45 LPA (BCG India base: ₹28 LPA + ₹6-10 LPA bonus)
- Mid-tier consulting (Deloitte, KPMG, EY healthcare): ₹15-22 LPA
2. Pharma / Medical Devices Industry
- Product Manager / Brand Manager: ₹12-18 LPA starting
- Medical Affairs Manager: ₹14-20 LPA starting
3. Hospital Management / Healthcare Strategy
- Hospital Administrator / Operations Manager: ₹8-14 LPA starting
- Strategy / Business Development roles: ₹12-18 LPA starting
4. Health-Tech / Digital Health Startups
- Product Manager / Business Analyst: ₹15-25 LPA starting (equity may be additional)
5. General Management / Finance / FMCG
- Same as general IIM averages above
Realistic Starting Salary Summary (BDS + IIM MBA)
| IIM Tier | Sector | Expected Starting Salary |
|---|---|---|
| IIM A/B/C (Top 3) | Consulting (MBB) | ₹28-45 LPA |
| IIM A/B/C | General management / Finance | ₹20-30 LPA |
| IIM A/B/C | Pharma / Healthcare | ₹14-22 LPA |
| IIM L/I/K (Next tier) | Consulting / Pharma | ₹12-20 LPA |
| IIM L/I/K | Hospital management | ₹10-15 LPA |
| New IIMs (Udaipur, Raipur etc.) | Any sector | ₹8-14 LPA |
Key Points to Know
-
IIM A/B/C is a different league - if you crack CAT with a 99+ percentile and get into the top 3, your salary floor is very different from newer IIMs.
-
BDS actually helps you, not hurts you - at interviews for pharma, healthcare consulting, or health-tech roles, your clinical understanding is a genuine advantage. Use it as your differentiator.
-
Work experience matters - If you do 1-2 years at a hospital, dental clinic, CRO (clinical research org), or pharma company before your MBA, you will get better shortlists and higher packages.
-
The "average" hides a wide range - At IIM Ahmedabad, the top 10% earn ₹50+ LPA while the bottom 10% may get ₹16-18 LPA. Your placement depends heavily on your interview performance and sector choice.
-
Healthcare management is growing fast - India's healthcare market is projected to reach $638 billion by 2025. BDS + MBA from IIM positions you perfectly ahead of this curve.
Quick Verdict
A BDS + MBA from IIM A/B/C gives you a realistic starting salary of ₹20-35 LPA in most roles, with healthcare consulting potentially reaching ₹30-45 LPA. From a mid-tier IIM, expect ₹12-20 LPA to start, with strong upward growth within 3-5 years.
What is the salary growth after 5 yrs in healthcare management if above mentioned iims
IIM MBA healthcare management salary after 5 years career growth India 2024 2025
healthcare consultant manager salary India 5 years experience senior manager pharma hospital IIM MBA
Salary Growth After 5 Years - BDS + IIM MBA in Healthcare Management
The Core Trajectory
Year-by-Year Salary Growth Chart
| Years Post-MBA | Role/Level | IIM A/B/C Graduate | IIM L/I/K Graduate | New IIMs |
|---|---|---|---|---|
| Year 0 (Fresher) | Analyst / Associate | ₹20-35 LPA | ₹12-20 LPA | ₹8-14 LPA |
| Year 1-2 | Senior Analyst / AM | ₹22-38 LPA | ₹14-22 LPA | ₹10-16 LPA |
| Year 3 | Manager / Consultant | ₹28-45 LPA | ₹18-28 LPA | ₹13-20 LPA |
| Year 4-5 | Senior Manager / Sr. Consultant | ₹35-60 LPA | ₹22-35 LPA | ₹16-25 LPA |
| Year 7-10 | Director / Principal / AVP | ₹50-90 LPA | ₹35-55 LPA | ₹25-40 LPA |
Sector-Wise Salary at 5 Years (BDS + IIM MBA)
1. Healthcare Consulting (McKinsey / BCG / Bain / EY / Deloitte)
| Stage | Role | Salary |
|---|---|---|
| Starting | Associate / Analyst | ₹28-45 LPA |
| 3 years | Engagement Manager / Consultant | ₹45-65 LPA |
| 5 years | Senior Consultant / Project Leader | ₹55-80 LPA |
| 7-10 years | Principal / Associate Partner | ₹80-1.2 CPA |
2. Pharma / Medical Devices (Sun Pharma, Abbott, J&J, Roche, Novartis)
| Stage | Role | Salary |
|---|---|---|
| Starting | Brand Manager / Product Manager | ₹14-20 LPA |
| 3 years | Senior Brand Manager | ₹20-28 LPA |
| 5 years | Group Product Manager / Regional Manager | ₹28-40 LPA |
| 7-10 years | Marketing Head / Business Unit Head | ₹45-65 LPA |
3. Hospital Management / Healthcare Strategy (Apollo, Fortis, Max, Narayana)
| Stage | Role | Salary |
|---|---|---|
| Starting | Operations Executive / Strategy Associate | ₹10-16 LPA |
| 3 years | Assistant Manager / Operations Manager | ₹15-22 LPA |
| 5 years | Senior Manager / Cluster Head | ₹22-35 LPA |
| 7-10 years | COO / Regional Director | ₹40-60 LPA |
4. Health-Tech / Digital Health (Practo, 1mg, PharmEasy, Niramai, startups)
| Stage | Role | Salary |
|---|---|---|
| Starting | Product Manager / Business Analyst | ₹15-25 LPA |
| 3 years | Senior PM / Lead | ₹25-35 LPA |
| 5 years | Product Head / VP Operations | ₹35-55 LPA (+ ESOPs) |
| Startup exit | Equity can multiply total wealth 5-10x | Variable |
5. Health Insurance / BFSI Healthcare (Star Health, Niva Bupa, ICICI Lombard)
| Stage | Role | Salary |
|---|---|---|
| Starting | Manager | ₹12-18 LPA |
| 5 years | Senior Manager / Regional Head | ₹20-30 LPA |
| 10 years | VP / National Head | ₹35-50 LPA |
What Drives Faster Salary Growth After 5 Years
| Factor | Impact |
|---|---|
| IIM A/B/C pedigree | Opens doors at MBB, global pharma - your ceiling is much higher |
| BDS clinical background | Differentiates you in healthcare consulting, pharma - companies pay a premium for this |
| Getting into consulting early | Consulting career tracks promote quickly - 2 promotions in 5 years is normal |
| Moving to a startup as an early employee | Base may be lower but equity at exit can be massive |
| International exposure / overseas posting | Global pharma companies pay 40-60% more for India-posted expats |
| MBA + Clinical Research / Regulatory background | CROs, medical devices companies pay ₹25-40 LPA at 5 years |
Honest Comparison: BDS Only vs BDS + IIM MBA (at 5 years)
| Path | Typical Role at 5 Years | Salary at 5 Years |
|---|---|---|
| BDS only (private practice) | Dentist (own clinic) | ₹6-15 LPA (depends on practice) |
| BDS only (corporate hospital) | Associate Dentist | ₹6-10 LPA |
| BDS + MBA (non-IIM) | Hospital Manager | ₹10-18 LPA |
| BDS + MBA (IIM L/I/K) | Senior Manager / Consultant | ₹22-35 LPA |
| BDS + MBA (IIM A/B/C) | Senior Consultant / Manager | ₹35-60 LPA |
The 10-Year Picture (Quick Preview)
- Year 0: ₹28-35 LPA
- Year 5: ₹50-70 LPA
- Year 10: ₹80 LPA - ₹1.5 CPA (Director/Partner level)
Is there a management quota in iim india for mba
IIM India management quota MBA admission 2024 2025
do IIMs have management quota donation seat MBA admission India
No - IIMs Do NOT Have Management Quota
The Direct Answer
Why IIMs Have No Management Quota
| Reason | Explanation |
|---|---|
| Government institutions | All IIMs are set up under the IIM Act 2017 - they are centrally funded institutions and cannot legally offer paid/donated seats |
| Regulated by Ministry of Education | They follow strict government admission norms - no scope for discretionary seats |
| Reputational model | Their entire global brand and placement value is built on merit selectivity - management quota would destroy that |
| No private ownership | Management quota exists only where private promoters/trusts own the college and need to recover investment |
The Only Way Into IIMs (Legitimate Routes)
Route 1 - CAT (Most Common)
- Common Admission Test - held every November
- Scores used by all 20 IIMs
- For BDS graduates: you are fully eligible
- Minimum 99+ percentile for IIM A/B/C; 95-97+ for IIM L/I/K
- After CAT: Written Ability Test (WAT) + Personal Interview (PI) round
Route 2 - GMAT/GRE (For Executive/International Programs)
- IIM Ahmedabad PGPX (1-year Executive MBA) - accepts GMAT, needs 5+ years work experience
- IIM Bangalore EPGP - accepts GMAT, needs 5+ years work experience
- IIM Calcutta PGPEX - similar
- These are legitimate alternatives if you have work experience and a good GMAT score
Route 3 - Non-CAT Specialized Programs
- IIM Bodh Gaya's MBA in Hospital & Healthcare Management - accepts CAT/CMAT/MAT
- IIM Jammu's healthcare program - CAT/CMAT accepted
- These have lower cutoffs than general MBA programs
What About "Direct Admission in IIM Management Quota" Websites?
Bottom Line for You (BDS Aspirant)
- Crack CAT - start preparing seriously (6-12 months minimum)
- Target IIM healthcare programs (Bodh Gaya, Jammu) which accept CMAT and have lower cutoffs - ideal entry for healthcare professionals
- Build work experience first - 1-2 years in a hospital/CRO/pharma strengthens your PI profile significantly
- Consider PGPX/Executive MBA after 5 years of work - GMAT route, less competition than CAT, and BDS + work experience is a strong profile