Tell me in detail on subacute intestinal obstruction as there is case presentation in my hospital and i have to answer them all so give relavent description with images and from textbooks
Reading File
Finding Sources
Finding Sources
Searching Images
intestinal obstruction X-ray radiology bowel obstruction
Searching PubMed
"intestinal obstruction" AND "subacute" AND management
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Loading Image
Searching Images
subacute small bowel obstruction CT scan adhesions
Finding Sources
Loading Image
Loading Image
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Searching Images
intestinal obstruction pathophysiology causes adhesions hernia tumor
Reading File
Loading Image
Reading File
Reading File
Reading File
I now have all the comprehensive information needed. Let me compile the full detailed answer:
Subacute Intestinal Obstruction — Comprehensive Case Presentation Guide
1. Definition & Conceptual Framework
Subacute intestinal obstruction (also called partial or low-grade obstruction) represents an incomplete blockage of the intestinal lumen where some gas and fluid can still pass beyond the obstruction point. It occupies the clinical middle ground between:
| Feature | Acute/Complete | Subacute/Partial | Chronic |
|---|---|---|---|
| Onset | Sudden | Gradual / insidious | Weeks–months |
| Lumen occlusion | 100% | Partial (30–90%) | Variable |
| Flatus/stool passage | Absent | Present but reduced | Intermittent |
| Strangulation risk | High | Lower but present | Low |
| Emergency surgery | Often immediate | Watchful waiting ± surgery | Elective |
"Continued passage of flatus and/or stool beyond 6 to 12 hours after onset of symptoms is characteristic of partial rather than complete obstruction." — Schwartz's Principles of Surgery, 11th Ed.
2. Epidemiology
- SBO accounts for 2% of all ED presentations with abdominal pain, causing ~300,000 hospitalizations/year in the USA
- Mortality has fallen from ~60% in 1900 to <8% today due to imaging advances and better surgical care
- Adhesions remain the #1 cause across all age groups
- Recurrence rate is high: 40% after non-operative treatment, 27% after surgery
(Rosen's Emergency Medicine, 10th Ed.)
3. Causes & Relative Frequency
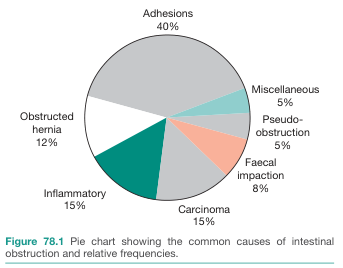
Figure 1. Common causes of intestinal obstruction and relative frequencies (Bailey & Love's Short Practice of Surgery, 28th Ed.)
Classification by anatomical site of obstruction:
| Category | Examples |
|---|---|
| Intraluminal | Gallstone ileus, bezoar, foreign body, meconium, fecal impaction |
| Intramural | Crohn's disease stricture, radiation stricture, primary intestinal tumor, hematoma, TB, ischemic stricture |
| Extrinsic | Adhesions (~40–75%), hernias (inguinal, femoral, internal), carcinomatosis, volvulus, intussusception |
Specific causes for subacute pattern:
- Adhesions from prior surgery (most common): intermittent partial obstruction is classic
- Crohn's disease strictures: chronic fibrotic narrowing, recurrent episodes
- Radiation enteritis: submucosal fibrosis causing progressive narrowing
- Intussusception in adults: often presents in a subacute manner with intermittent symptoms
- Malignancy: carcinomatosis causing multiple partial points; colon cancer; external compression
- Gallstone ileus: may present subacutely with tumbling obstruction (Rigler's triad)
- Superior mesenteric artery syndrome: compression of 3rd part of duodenum in young asthenic patients
(Schwartz's Principles of Surgery, 11th Ed.)
4. Pathophysiology
Partial luminal obstruction
↓
Gas & fluid accumulate proximal to obstruction
(swallowed air + stimulated intestinal secretions)
↓
Peristalsis increases → colicky pain + early loose stools
↓
Bowel distension → ↑ intraluminal & intramural pressure
↓
Intestinal motility gradually decreases
↓
Luminal flora shifts (normally sterile small bowel) → bacterial translocation
↓ [if untreated]
Intramural pressure exceeds microvascular perfusion pressure
↓
INTESTINAL ISCHEMIA → STRANGULATION → NECROSIS → PERFORATION
Key distinction in partial obstruction:
- The progression above occurs more slowly than in complete obstruction
- Strangulation is less likely but not impossible — closed-loop obstruction can still develop even in the setting of partial obstruction
(Schwartz's Principles of Surgery, 11th Ed.)
5. Clinical Features
Symptoms (classic tetrad):
| Symptom | Subacute Pattern |
|---|---|
| Abdominal pain | Intermittent, crampy/colicky; may partially resolve spontaneously |
| Nausea & vomiting | Present; may be bilious (proximal obstruction) or feculent (long-standing, bacterial overgrowth) |
| Abdominal distension | Present; more prominent with distal lesions |
| Change in bowel habit | Reduced stool/flatus but NOT complete obstipation (key differentiator from complete obstruction) |
Physical Examination Signs:
- Abdominal distension with tympany on percussion
- High-pitched/tinkling bowel sounds (hyperactive early) → may become quiet in late stages
- Tenderness — diffuse mild-to-moderate; localized severe tenderness suggests strangulation
- Visible peristalsis — classic but subtle finding
- Hernia orifices — always examine groins, umbilicus, prior surgical scars carefully
- Peritoneal signs (rebound, guarding, rigidity) — absent in uncomplicated subacute obstruction; if present → strangulation/perforation
Red Flags → Suggest Strangulation (requires URGENT surgery):
- Pain disproportionate to exam findings
- Fever >38°C
- Tachycardia
- Marked leukocytosis (>15,000)
- Metabolic acidosis
- Localized peritonism
(Schwartz's Principles of Surgery, 11th Ed.; Rosen's Emergency Medicine, 10th Ed.)
6. Investigations
A. Laboratory
| Test | Findings |
|---|---|
| CBC | Mild leukocytosis (WBC 10,000–15,000); hemoconcentration |
| Electrolytes | Hypokalemia, hyponatremia, metabolic alkalosis (from vomiting) |
| BUN/Creatinine | ↑ (volume depletion) |
| Lactate | ↑ in strangulation/ischemia — critical marker |
| ABG | Metabolic acidosis in late/strangulated cases |
| LFTs, amylase | To exclude other causes of abdominal pain |
B. Imaging
Plain Abdominal X-Ray (Erect + Supine)
- Triad: dilated small bowel loops (>3 cm), air-fluid levels on erect film, paucity of colonic gas
- "Stepladder" pattern of air-fluid levels in central abdomen (valvulae conniventes/"keyboard" sign)
- Sensitivity: 70–80%; Specificity: low (ileus can mimic)
- In partial obstruction: gas may still be visible distal to the obstruction
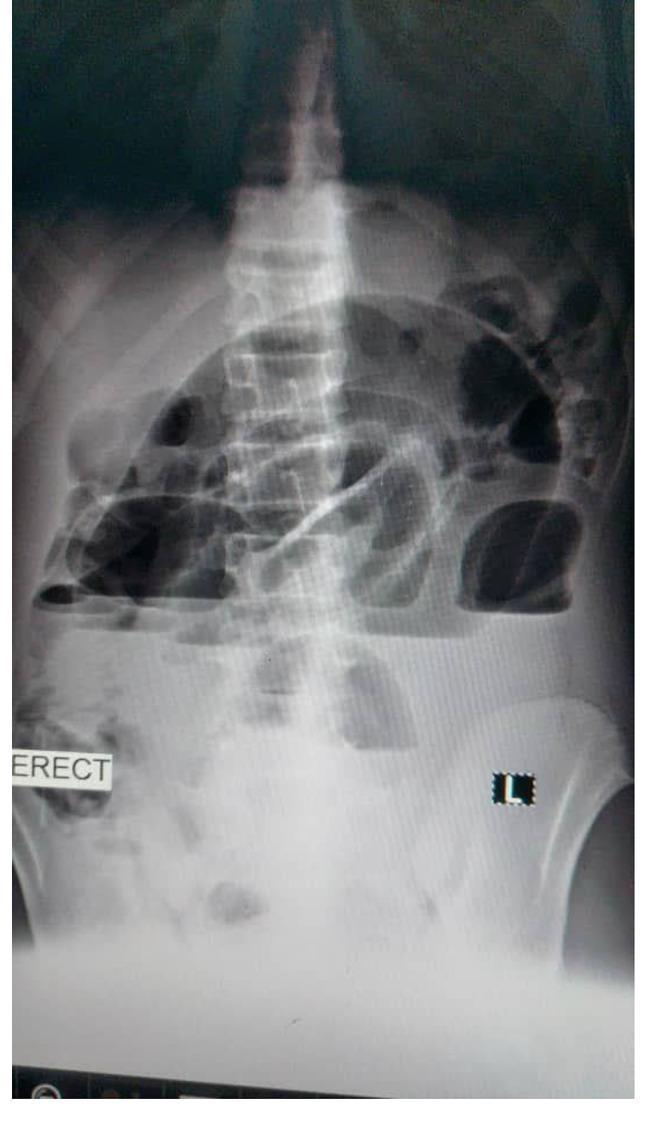
Figure 2. Erect abdominal X-ray showing multiple horizontal air-fluid levels ("stepladder") with distended central small bowel loops — hallmark of mechanical SBO.
CT Abdomen (Gold Standard — with oral contrast)
- Sensitivity 80–90%, Specificity 70–90%
- Key findings:
- Discrete transition zone (dilated bowel proximal → decompressed distal)
- Intra-luminal contrast not passing beyond transition zone
- "Small bowel feces sign" — mottled bubbly material in dilated loop — classic for subacute/chronic obstruction
- Mesenteric vascular changes, ascites → suggests malignant cause
- Smooth transition + smooth bowel wall → benign (adhesion)
- Abrupt transition + mass + irregular thickening → malignant
Note: CT has <50% sensitivity for low-grade partial obstruction — a subtle transition zone can be missed. Small bowel follow-through or CT enteroclysis is more sensitive for low-grade SBO.
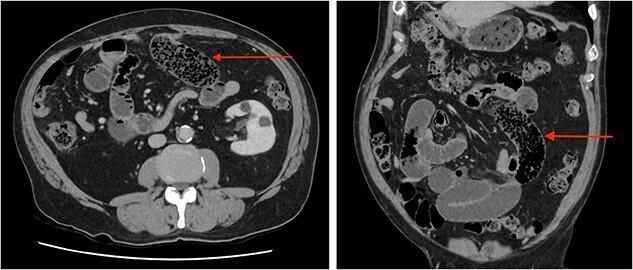
Figure 3. Axial and coronal CT demonstrating the "small bowel feces sign" (red arrows) — mottled bubbly content in dilated small bowel loops — seen characteristically in subacute or chronic partial obstruction, typically due to adhesions. (Source: PMC clinical imaging library)
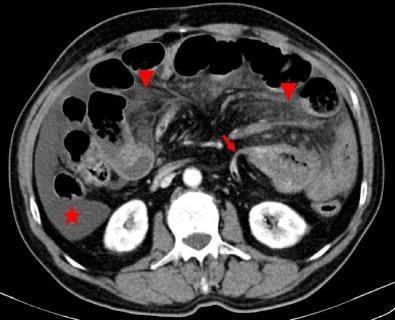
Figure 4. Axial CT showing SBO secondary to adhesion: abrupt angulation at transition point (red arrow), mesenteric fat stranding (arrowheads), and free peritoneal fluid (star) — signs of complicated obstruction. (PMC clinical imaging library)
CT Signs of Strangulation to Actively Look For:
| CT Finding | Implication |
|---|---|
| Bowel wall thickening | Edema, ischemia |
| Pneumatosis intestinalis | Air in bowel wall — ischemia |
| Portal venous gas | Severe ischemia / necrosis |
| Mesenteric haziness/fat stranding | Vascular congestion |
| Poor contrast uptake in bowel wall | Ischemic bowel |
| U/C-shaped loop + radial mesenteric vessels | Closed-loop obstruction |
(Schwartz's Principles of Surgery, 11th Ed.)
Small Bowel Follow-Through / Enteroclysis
- Best modality for detecting low-grade partial obstruction (higher sensitivity than CT for subtle lesions)
- Water-soluble contrast (Gastrografin): therapeutic + prognostic value
- Appearance of contrast in colon within 24 hours = predicts nonoperative resolution with sensitivity 92%, specificity 93%
7. Management Algorithm
Suspected Subacute Intestinal Obstruction
↓
History, Examination, Labs, Plain X-Ray
↓
CT Abdomen (oral + IV contrast)
↓
┌─────────────────────────────┐
│ Red flags present? │
│ (peritonism, fever, │
│ tachycardia, ↑ lactate, │
│ strangulation on CT) │
└──────────┬──────────────────┘
│ YES → URGENT SURGERY
│
NO
↓
CONSERVATIVE MANAGEMENT (48–72 hrs)
- NBM / bowel rest
- IV fluid resuscitation (isotonic crystalloid)
- NG tube (if significant vomiting/distension)
- Urinary catheter (monitor UO)
- Antiemetics
- Correct electrolytes
- Serial abdomen examinations
↓
Water-soluble contrast (Gastrografin) challenge
— monitor for passage to colon in 24 hrs
↓
┌──────────────────────────────┐
│ Improving within 48 hrs? │
└──────────┬───────────────────┘
│ YES → Gradual oral intake, discharge plan
│
NO → SURGICAL CONSULTATION
→ Laparoscopy / Open adhesiolysis
→ Resection if strangulated/necrotic
Non-operative Management (Mainstay for Partial/Subacute SBO):
- Success rate: 65–81% for partial SBO
- Only 5–15% do not improve within 48 hours of initiating conservative therapy
- The "sun should never rise and set on a complete obstruction" — but for partial obstruction, a 48-hour watchful waiting period is safe and appropriate
- NG decompression: reasonable for persistent vomiting; not mandatory for simple adhesive SBO where nausea can be controlled with antiemetics (ondansetron 4 mg IV q6–8h; metoclopramide 10 mg IV q6–8h)
Surgical Indications:
- Evidence of strangulation or ischemia (any stage)
- Failure of conservative management after 48–72 hours
- Complete obstruction
- Closed-loop obstruction on imaging
- Peritonitis
(Schwartz's Principles of Surgery, 11th Ed.; Rosen's Emergency Medicine, 10th Ed.)
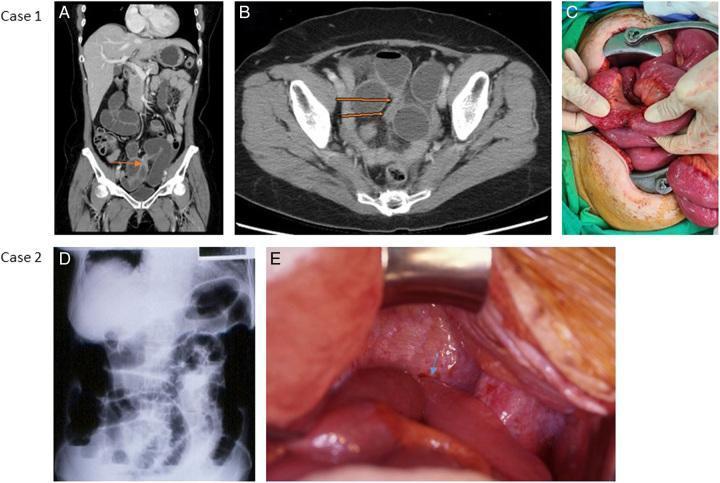
Figure 5. Multi-modal SBO correlation: (A,B) Coronal and axial CT showing transition zone in pelvis with proximal dilation; (C) Intraoperative adhesive band confirmed; (D) Plain X-ray with classic air-fluid levels; (E) Incarcerated terminal ileum with volvulus and adhesions. (PMC clinical imaging library)
8. Special Situations in Subacute Obstruction
Malignant Obstruction (Advanced Cancer)
- Peritoneal carcinomatosis → multiple partial obstruction sites (colon, ovarian, gastric cancers)
- Onset is usually insidious with colicky pain
- Prognosis poor: median survival 3–4 months after first episode
- Management options:
- Self-expanding metal stents (colorectal, gastroduodenal)
- Venting gastrostomy (for nausea/vomiting palliation)
- Octreotide 300 mcg/day IV (reduces GI secretions, decreases obstructive symptoms)
- Glucocorticoids (anti-inflammatory, may aid resolution)
- Metoclopramide (only for incomplete/functional obstruction — contraindicated in complete)
(Harrison's Principles of Internal Medicine, 22nd Ed.)
Crohn's Disease Stricture
- Fibrotic strictures → chronic partial obstruction → episodic subacute flares
- May respond to conservative treatment initially
- Endoscopic balloon dilation for short strictures
- Surgery: strictureplasty or resection
Intussusception in Adults
"It may occur in the small or large intestine and often presents in a subacute manner, with symptoms occurring for a prolonged period." — Sleisenger & Fordtran's Gastrointestinal and Liver Disease
- Unlike children, adult intussusception usually has a lead point (tumor, polyp, Meckel's diverticulum) — requires resection
- CT is diagnostic
9. Differential Diagnosis
| Condition | Key Differentiating Features |
|---|---|
| Paralytic ileus | No mechanical barrier; follows surgery/peritonitis; diffuse bowel dilatation; no transition point on CT |
| Ogilvie's syndrome (pseudo-obstruction) | Large bowel distension; no mechanical obstruction; elderly/bedridden |
| Acute mesenteric ischemia | Severe disproportionate pain, rapid deterioration, ↑ lactate early |
| Acute pancreatitis | ↑ amylase/lipase; localized "sentinel loop"; epigastric radiation to back |
| Volvulus | "Coffee-bean" sign (sigmoid) or Rigler's triad on plain film |
| Perforation | Free gas under diaphragm; peritonitis |
| Gastroenteritis | Watery diarrhea, no mechanical obstruction features |
10. Complications
| Complication | Mechanism |
|---|---|
| Dehydration + shock | Vomiting + fluid sequestration in bowel wall |
| Metabolic alkalosis | Loss of HCl from proximal obstruction |
| Hypokalemia | Vomiting + ileus |
| Strangulation → necrosis | ↑ intramural pressure → ischemia |
| Perforation → peritonitis | Necrosis of bowel wall |
| Sepsis | Bacterial translocation, perforation |
| Short bowel syndrome | After extensive bowel resection |
| Wound infection, recurrence | Post-surgical complications |
11. Prognosis & Recurrence
- Non-operative success rate: 65–81% for partial SBO
- Recurrence: 40% after non-operative management vs. 27% after surgery
- For malignant obstruction: median survival 3–4 months
- 2-day watchful waiting before surgery is safe and does not increase mortality or postoperative morbidity
Key Teaching Points for Case Presentation
- Subacute = partial = incomplete — gas/stool still passes; onset is insidious
- The "small bowel feces sign" on CT is highly characteristic of subacute/chronic obstruction
- Always distinguish partial vs. complete and simple vs. strangulated — this drives management
- Adhesions are the #1 cause (up to 75% of cases); always ask for prior surgery history
- 48-72 hours of conservative management is safe for partial obstruction without ischemic features
- Gastrografin challenge has both diagnostic (predicts resolution) and possible therapeutic value
- Any lactate rise, fever, tachycardia, or peritonism = abandon conservative management → OR
- In malignant partial obstruction: octreotide + stenting are key non-operative tools
- CT sensitivity for low-grade partial obstruction is <50% — use small bowel follow-through if CT is negative but clinical suspicion persists
- Recurrence is common — discuss long-term follow-up with patients
Sources:
- Schwartz's Principles of Surgery, 11th Edition — Chapter 28 (Small Bowel)
- Rosen's Emergency Medicine, 10th Edition — Chapter 78 (Small Bowel Obstruction)
- Harrison's Principles of Internal Medicine, 22nd Edition — Intestinal Obstruction
- Sleisenger & Fordtran's Gastrointestinal and Liver Disease — Acute/Chronic SBO, Intussusception
- Bailey & Love's Short Practice of Surgery, 28th Edition — Figure 78.1
With detailed hopi as case presentation
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
I now have the key textbook material including the comparison table of three hypothetical patients. Let me now compile the comprehensive case presentation with a full HOPI.
Subacute Intestinal Obstruction — Full Case Presentation with Detailed HOPI
CASE PRESENTATION
IDENTIFYING DATA
Patient: Mr. Ramesh Kumar (fictitious name)
Age: 52 years
Sex: Male
Occupation: Farmer
Residence: Rural district
Date of Admission: [Insert date]
Referred from: Primary Health Centre
Informant: Patient himself (reliable)
CHIEF COMPLAINTS
- Colicky abdominal pain — 7 days
- Abdominal distension — 5 days
- Nausea and vomiting — 5 days
- Reduced passage of stool and flatus — 4 days
HISTORY OF PRESENT ILLNESS (HOPI)
(This is the most critical section — explore using SOCRATES for pain + systematic review of associated symptoms)
Symptom 1: Abdominal Pain
Mr. Ramesh Kumar, a 52-year-old male, was apparently well until 7 days prior to admission, when he developed pain in the abdomen.
Site: Initially diffuse, predominantly periumbilical, later shifting to the central and lower abdomen.
Onset: Gradual, insidious. The pain started mildly and worsened over several days. The patient denies any precipitating factor such as trauma, heavy lifting, or dietary excess. (In acute obstruction onset is sudden — in subacute it is gradual and escalating over days.)
Character: Distinctly colicky in nature — described as crampy, gripping waves of pain. Each episode lasts 2–5 minutes, followed by a brief pain-free interval of 5–15 minutes, then recurs. The patient instinctively doubles over or presses his abdomen during attacks.
Radiation: No radiation to the back, groin, or shoulder.
Severity: Initially 3–4/10; escalated to 6–7/10 by day 5. Pain is intermittent but the episodes are becoming more frequent and the pain-free intervals are shortening. (Shortening pain-free intervals suggests progressive obstruction.)
Aggravating factors: Eating any food — even small amounts trigger a severe colicky episode within 30–60 minutes. (Postprandial worsening is classic for partial mechanical obstruction.)
Relieving factors: Partial relief with lying still, vomiting, and passage of flatus. (Passage of flatus/stool differentiates this from complete obstruction.)
Associated with: The pain is preceded by loud, audible gurgling bowel sounds (borborygmi) that the patient notices himself.
Symptom 2: Abdominal Distension
Onset: Started 5 days ago, approximately 2 days after the pain began.
Progression: Gradually increasing, more prominent towards evening and after meals. The patient noticed his clothes becoming tight around the waist.
Character: Diffuse, symmetrical distension. No localized lump or swelling noticed by the patient.
Associated with: Feeling of fullness, a sense of incomplete bowel emptying, and audible bowel sounds.
Symptom 3: Nausea and Vomiting
Onset: 5 days ago, appearing alongside the distension.
Frequency: 3–5 episodes per day.
Character of vomitus:
- Initially — yellowish-green (bilious) in colour, non-projectile, partially digested food
- Over the last 2 days — vomitus has become brownish with a foul/feculent odour, suggesting bacterial overgrowth in stagnant intestinal contents — a sign of more established and prolonged partial obstruction
- No blood in vomitus (haematemesis absent)
Volume: Approximately 200–400 mL per episode.
Relief: Vomiting provides temporary relief from distension and pain.
Timing: Often triggered by eating; also occurs spontaneously.
"Feculent vomitus with bacterial overgrowth suggests a more established obstruction." — Schwartz's Principles of Surgery, 11th Ed.
Symptom 4: Altered Bowel Habits
Prior to illness: Regular bowel habits — one soft stool per day, brown in colour.
During illness:
- Days 1–3: Loose watery stools (2–3/day) — this is characteristic of early SBO where increased peristalsis to overcome the obstruction causes diarrhoea even in the presence of obstruction
- Days 4–7: Bowel frequency has reduced significantly — passing small amounts of flatus and minimal soft stool once in 2 days
- Key point: Patient has NOT had complete cessation of flatus/stool — this confirms partial (subacute) rather than complete obstruction
- No blood in stool (no melaena, no haematochezia)
- No mucus in stool
"Continued passage of flatus and/or stool beyond 6–12 hours after onset of symptoms is characteristic of partial rather than complete obstruction." — Schwartz's Principles of Surgery, 11th Ed.
Directly Pertinent Negatives (Important to Ask and Document)
| Feature | Status | Significance |
|---|---|---|
| Complete obstipation (no flatus at all) | Absent | Confirms partial, not complete obstruction |
| Fever / chills | Absent (so far) | No strangulation/peritonitis currently |
| Haematochezia / melaena | Absent | No intraluminal bleed |
| Haematemesis | Absent | |
| Jaundice | Absent | |
| Urinary symptoms | Absent | Excludes urological cause |
| Cough, dyspnoea | Absent | Excludes referred pain |
| Weight loss / anorexia | Mild anorexia (eating very little for 7 days) | Important — raises malignancy flag |
| Significant weight loss >5 kg | Patient uncertain — wife reports clothes looser | Needs formal assessment |
| Passage of blood/mucus per rectum | Absent | |
| Previous similar episodes | Yes — one mild episode 6 months ago that resolved spontaneously over 2 days | Suggests recurrent partial obstruction from adhesions |
Temporal Summary of Symptom Evolution
Day 1–2: Vague periumbilical colicky pain (mild, 3/10)
No vomiting yet; loose stools 2–3 times/day (early peristaltic response)
Day 3–4: Pain worsens (5/10), becomes more frequent and colicky
Nausea begins; bilious vomiting starts (2–3 episodes/day)
Distension appears; audible borborygmi
Day 5–6: Distension worsens; vomiting becomes more frequent & feculent
Stool frequency decreasing — small amounts only with effort
Still passing flatus (confirms partial obstruction)
Patient unable to eat
Day 7: Patient seeks hospital admission
Pain 6–7/10, colicky; marked distension
Feculent vomiting; minimal flatus
No fever, no peritoneal signs
PAST HISTORY
Surgical History:
- Underwent appendicectomy 12 years ago (open, right iliac fossa incision) for acute appendicitis at a district hospital
- (This is CRITICAL — prior abdominal surgery is the #1 risk factor for adhesive SBO, accounting for up to 75% of cases)
- No other abdominal surgeries
Medical History:
- Hypertension — on Tab. Amlodipine 5 mg OD for 3 years (well-controlled)
- No known diabetes mellitus
- No history of tuberculosis (document specifically — TB strictures are a cause of SBO in endemic regions)
- No history of inflammatory bowel disease
Drug History:
- Tab. Amlodipine 5 mg OD
- No NSAIDs, steroids, or anticoagulants
- No history of chemotherapy or radiation (rules out radiation enteritis and chemo-related ileus)
Allergies: No known drug allergies.
FAMILY HISTORY
- Father: Diabetes mellitus
- No family history of colorectal cancer, inflammatory bowel disease, or malignancy
- No similar illness in family members
PERSONAL HISTORY
- Farmer by occupation — moderate physical activity
- Diet: Predominantly vegetarian; irregular meals; high-fibre diet
- Appetite: Markedly reduced over the past 7 days (anorexia secondary to obstruction)
- Bowel habits: As described above — previously regular; now reduced
- Bladder habits: Normal micturition; urine output appears reduced in last 2 days (suggesting dehydration)
- Sleep: Disturbed due to colicky pain
- Addictions:
- Tobacco: Bidi smoking — 5 bidis/day for 20 years (10 pack-years) (relevant for overall surgical risk)
- Alcohol: Occasional social drinker; no significant alcohol use
- Marital status: Married, 2 children
SOCIOECONOMIC HISTORY
- Lives in a rural area; moderately built home
- Comes from a lower-middle-income family
- No access to clean piped water
- Works as a farmer — manual labour
REVIEW OF SYSTEMS (Systematic enquiry — pertinent to the case)
| System | Findings |
|---|---|
| General | Mild weight loss (uncertain), anorexia for 7 days, fatigue |
| CVS | No chest pain, no palpitations; known hypertensive |
| Respiratory | No dyspnoea, no cough |
| GIT | As detailed in HOPI |
| Genitourinary | Reduced urine output last 2 days; no dysuria |
| Musculoskeletal | No joint pains |
| Neurological | No altered sensorium |
| Skin | No jaundice, pallor uncertain |
PHYSICAL EXAMINATION FINDINGS (Expected on presentation)
General Examination
| Parameter | Finding |
|---|---|
| Conscious | Yes, alert, oriented to time-place-person |
| Built & Nourishment | Moderately built, mildly malnourished |
| Pallor | Mild (chronic poor intake) |
| Icterus | Absent |
| Cyanosis | Absent |
| Clubbing | Absent |
| Lymphadenopathy | Absent |
| Oedema | Absent |
| Dehydration | Mild — dry tongue, slightly reduced skin turgor, sunken eyes |
Vital Signs
| Parameter | Finding | Interpretation |
|---|---|---|
| Pulse | 96/min, regular, low volume | Tachycardia — dehydration |
| BP | 104/72 mmHg | Mild hypotension (volume depleted) |
| Temperature | 37.2°C (afebrile) | No fever — no strangulation yet |
| RR | 18/min | Normal |
| SpO2 | 98% on room air |
Abdominal Examination
Inspection:
- Distension — moderate, generalised, symmetrical; more prominent in the central abdomen and flanks
- Umbilicus central and inverted (no eversion — rules out significant ascites)
- Visible peristaltic waves — seen in the central abdomen during colicky episodes (classic sign)
- Scar: Healed right iliac fossa scar from previous appendicectomy (oblique, 7 cm, well-healed) — key operative history confirmed
- No visible hernial orifices at rest
Auscultation (done before palpation):
- Hyperactive, high-pitched, tinkling bowel sounds — with audible metallic rushes coinciding with pain episodes (peristaltic rushes trying to overcome the obstruction)
- No absence of bowel sounds (which would suggest ileus or peritonitis)
Palpation:
- Abdomen is soft (not rigid — peritonism absent)
- Mild generalised tenderness — diffuse, without specific localisation; no rigidity
- No guarding, no rebound tenderness (absence of peritoneal signs rules out strangulation/perforation at this point)
- No palpable mass
- Hernia orifices: No inguinal, femoral, or umbilical hernia palpable
Percussion:
- Generalised tympany — due to gas in distended bowel loops
- Liver and splenic dullness preserved
- No shifting dullness (no ascites)
Digital Rectal Examination (DRE) — Essential:
- Anal sphincter tone normal
- Rectum empty — no faecal impaction
- No mass palpable in the rectum
- No blood on the examining finger
(An empty rectum with obstruction above suggests mechanical SBO; faecal impaction would suggest a different aetiology)
PROVISIONAL DIAGNOSIS
Subacute (partial) mechanical small bowel obstruction, likely due to adhesions from previous appendicectomy
Differential Diagnoses:
- Adhesive partial SBO (most likely — prior appendicectomy, recurrent episode)
- Crohn's disease stricture (younger age group more common; no prior IBD history — less likely)
- Intestinal tuberculosis (endemic region, must exclude; no constitutional TB symptoms but still order)
- External hernia (none found on examination — excluded clinically)
- Internal hernia (no prior bariatric surgery — less likely but possible)
- Malignancy (age 52, anorexia, weight loss — cannot fully exclude; needs CT + scope)
- Gallstone ileus (no jaundice, no prior biliary symptoms — less likely)
- Paralytic ileus (no recent surgery, no peritonitis, no metabolic cause — clinical picture favours mechanical)
INVESTIGATION PLAN
Bedside / Immediate:
| Investigation | Expected finding |
|---|---|
| Blood glucose | Rule out hypoglycaemia as confound |
| Urine dipstick | Rule out UTI |
| ECG | Pre-op baseline; rule out MI causing ileus |
Blood Tests:
| Test | Expected/Rationale |
|---|---|
| CBC | Mild leukocytosis (WBC 11–14k), haemoconcentration (↑Hct) |
| Serum electrolytes | Hypokalemia, hyponatraemia (from vomiting) |
| BUN/Creatinine | ↑ (prerenal AKI from dehydration) |
| Serum lactate | Normal in uncomplicated; ↑ if ischaemia developing |
| ABG | Metabolic alkalosis (from vomiting) |
| Serum albumin | Nutritional status |
| LFTs | Baseline; exclude hepatic cause |
| Serum amylase/lipase | Rule out pancreatitis |
| Blood group & cross-match | Pre-operative preparation |
| CEA, CA19-9 | If malignancy suspected |
| Mantoux / IGRA | If TB enteritis suspected |
Imaging:
| Study | Priority | Expected Finding |
|---|---|---|
| Erect X-ray abdomen + chest | IMMEDIATE | Dilated small bowel loops, air-fluid levels ("stepladder"), paucity of colonic gas; no free gas under diaphragm |
| Supine X-ray abdomen | Immediate | Dilated central loops with valvulae conniventes visible ("coiled spring") |
| CECT abdomen (oral + IV contrast) | Within 4–6 hours | Transition zone, dilated proximal loops, "small bowel feces sign," no pneumatosis |
| Ultrasound abdomen | If CT unavailable | Fluid-filled loops, dilated bowel, peristalsis |
| Small bowel follow-through | If CT inconclusive | Map site of partial obstruction; Gastrografin has therapeutic value |
| Colonoscopy | If large bowel cause suspected |
MANAGEMENT PLAN
Immediate (Emergency):
- NPO — nothing by mouth
- IV access — two large-bore cannulas; commence IV fluids (Normal saline or Ringer's lactate)
- Nasogastric tube (Ryles tube, 14–16 Fr) — attach to low intermittent suction; monitor hourly output and character
- Urinary catheter — strict input-output charting; target urine output >0.5 mL/kg/hr
- Electrolyte correction — IV KCl supplementation in 500 mL NS once urine output confirmed
- Antiemetics — Ondansetron 4 mg IV q8h / Metoclopramide 10 mg IV q8h
- Analgesia — IV Tramadol 50 mg slow infusion PRN (use carefully; avoid opioids that worsen ileus if possible; Buscopan for antispasmodic effect)
- Serial abdominal examination every 4–6 hours
Monitoring — Signs of Deterioration (Indicating need for surgery):
| Sign | Action |
|---|---|
| Fever >38°C | Urgent surgical review |
| Tachycardia (HR >100) | Reassess; lactate |
| Peritoneal signs (rebound/guarding) | Immediate surgery |
| ↑ Serum lactate | Strangulation — urgent OR |
| Failure to improve in 48 hrs | Surgical intervention |
| Complete cessation of flatus | Suggests progression to complete obstruction |
Water-Soluble Contrast Challenge (Gastrografin):
- Administer 50–100 mL Gastrografin via NG tube at 24–48 hours after admission if no improvement
- Monitor with plain X-ray at 4 hours and 24 hours
- Appearance of contrast in colon within 24 hours = 92% sensitivity, 93% specificity for non-operative resolution
- Has both diagnostic AND therapeutic value
Surgical Management (if conservative fails or red flags develop):
- Laparoscopic adhesiolysis — preferred approach for adhesive SBO
- Open laparotomy — if laparoscopy not feasible, perforation, or dense adhesions
- Resection + primary anastomosis if strangulated or non-viable bowel found
- Resection + stoma if bowel unprepared, contaminated, or patient unstable
PATIENT COUNSELLING POINTS (for case presentation Q&A)
- Why is this subacute and not acute? — Gradual onset over 7 days, still passing some flatus/stool, no peritonism, moderate (not severe) systemic compromise
- Why do we still pass stool in partial SBO? — The lumen is not 100% occluded; liquid and gas can still squeeze past the narrowing
- Why is early peristaltic diarrhoea seen? — The bowel tries to overcome the obstruction by increasing peristaltic activity, pushing downstream contents past the partial block in the early phase
- Why does vomitus become feculent? — Bacterial overgrowth in stagnant small bowel contents (normally the small bowel is near-sterile); feculent vomiting = established, prolonged obstruction
- What is the 48-hour rule? — Conservative management is appropriate for 48 hrs in partial SBO; if no improvement, surgery is indicated. A 2-day watchful-waiting period does not increase mortality
- What triggers strangulation? — Rising intramural pressure exceeds microvascular perfusion pressure → ischaemia → necrosis. Closed-loop obstruction does this most rapidly
CASE SUMMARY (For formal presentation)
A 52-year-old male farmer with a history of open appendicectomy 12 years ago presented with a 7-day history of gradually worsening colicky periumbilical and central abdominal pain, 5 days of progressive abdominal distension and bilious-to-feculent vomiting, and 4 days of markedly reduced stool and flatus — though not complete obstipation. He reported a similar mild self-resolving episode 6 months ago. On examination he was afebrile, mildly tachycardic (96/min), hypotensive (104/72), and mildly dehydrated, with a soft distended abdomen, generalised tympany, visible peristalsis, high-pitched tinkling bowel sounds, and no peritoneal signs. An appendicectomy scar was present in the right iliac fossa. No hernia was palpable. DRE showed an empty rectum. Findings are consistent with subacute (partial) mechanical small bowel obstruction, most likely secondary to post-appendicectomy adhesions. He was admitted for IV fluid resuscitation, NG decompression, electrolyte correction, and 48-hour trial of conservative management with close monitoring for signs of strangulation and Gastrografin contrast challenge at 24 hours.
Textbook Sources:
- Schwartz's Principles of Surgery, 11th Ed. — Epidemiology, Pathophysiology, Clinical Presentation, Therapy
- Mulholland & Greenfield's Surgery, 7th Ed. — Clinical Presentation & Three-Patient Comparison Table
- Rosen's Emergency Medicine, 10th Ed. — ED Management, Conservative approach
- Harrison's Principles of Internal Medicine, 22nd Ed. — Malignant obstruction, Differential
- Bailey & Love's Short Practice of Surgery, 28th Ed. — Causes frequency chart
This is a shared conversation. Sign in to Orris to start your own chat.