Diabetic retinopathy
Reading File
Finding Sources
Searching PubMed
"diabetic retinopathy"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Here is the complete, detailed response:
Diabetic Retinopathy
Overview
Diabetic retinopathy (DR) is the most common cause of new blindness in most industrialised countries, primarily due to delayed diagnosis and treatment. With effective screening and implementation of findings from the Early Treatment Diabetic Retinopathy Study (ETDRS) and anti-VEGF clinical trials, the risk of severe visual loss can be reduced to less than 5%. - Kanski's Clinical Ophthalmology, 10th ed.
Epidemiology and Risk Factors
- Overall prevalence of DR in people with diabetes is approximately 40%
- In type 2 diabetes: 67% prevalence by 10 years after diagnosis; 10% will develop proliferative disease
- DR is more common and more severe in type 1 than type 2 diabetes
Key risk factors (Kanski's):
| Factor | Notes |
|---|---|
| Duration of diabetes | Most important predictor; DR rarely develops within 5 years of onset or before puberty |
| Poor glycemic control | Higher HbA1c = greater risk; DCCT confirmed tight control prevents/delays DR |
| Hypertension | Very common in type 2 DM; target <140/80 mmHg; especially important for maculopathy |
| Nephropathy | Severe nephropathy worsens DR; renal transplantation may improve it |
| Pregnancy | Can cause rapid progression; ~5% with mild DR and ~33% with moderate DR progress to PDR |
| Hyperlipidaemia | Additional risk factor |
| Pioglitazone | Associated with worsening diabetic macular oedema |
| GLP-1 receptor agonists | When associated with marked glycemic improvement, increased risk of worsening DR |
Pathogenesis
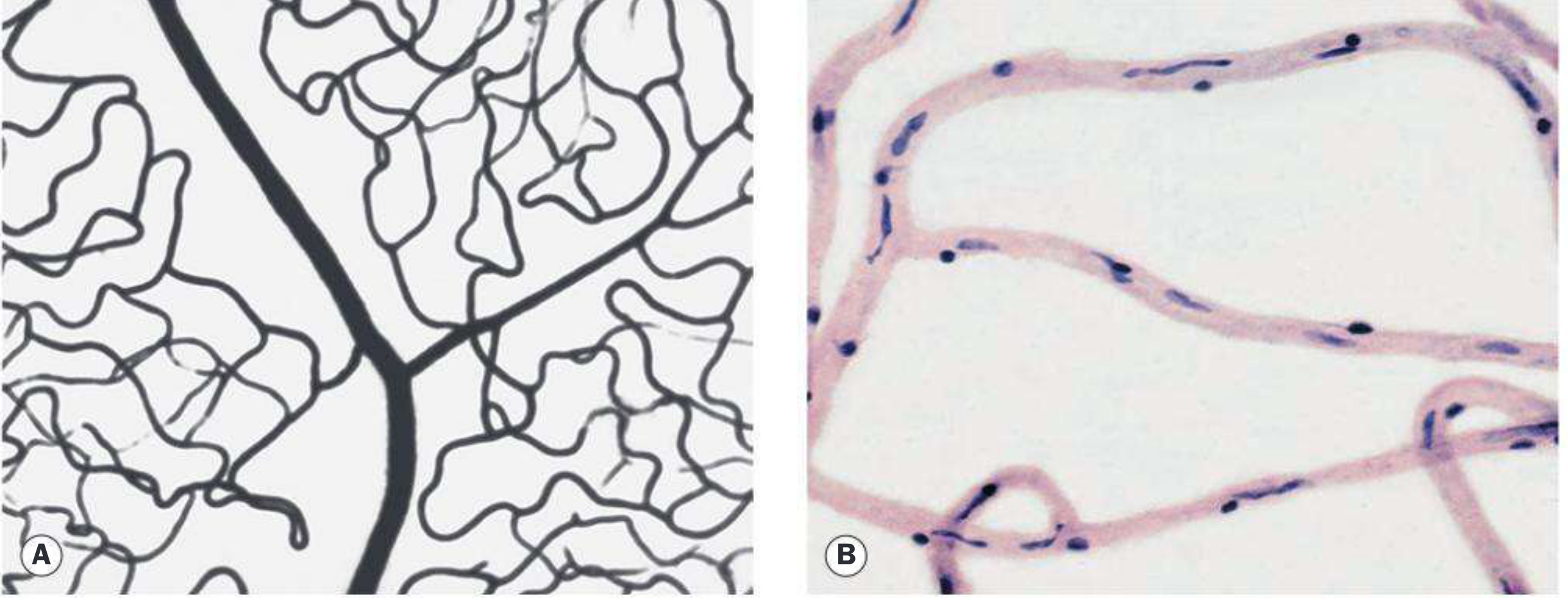
The key initial lesion is pericyte loss from retinal capillaries. Normally, pericytes (with rounded nuclei) wrap around retinal capillary endothelium (elongated nuclei), as shown below:
The sequence of pathological changes:
- Basement membrane thickening of retinal capillaries (microangiopathy)
- Pericyte loss - pericyte-to-endothelial cell ratio falls
- Microaneurysm formation - outpouchings from weakened capillary walls
- Blood-retinal barrier breakdown - driven by VEGF (originally named "vascular permeability factor"), leading to leakage and macular oedema
- Micro-occlusion - capillary non-perfusion creates retinal ischaemia
- VEGF upregulation from ischaemic retina drives intraretinal angiogenesis (NPDR) and ultimately neovascularisation that breaches the internal limiting membrane (PDR)
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 1807
Classification (International Disease Severity Scale)
| Stage | Defining Features |
|---|---|
| No apparent retinopathy | Normal fundus |
| Mild NPDR | Microaneurysms only |
| Moderate NPDR | More than mild NPDR; may include cotton-wool spots (CWSs), venous beading, blot haemorrhages |
| Severe NPDR | Any one of: >20 intraretinal haemorrhages in all 4 quadrants, venous beading in ≥2 quadrants, or prominent intraretinal microvascular abnormalities (IRMA) in ≥1 quadrant. No PDR (the "4-2-1 rule") |
| PDR | Neovascularisation of iris (NVI), angle (NVA), disc (NVD), or elsewhere (NVE); and/or vitreous/preretinal haemorrhage |
| Diabetic macular oedema (DME) | May be present at any stage; center-involving DME threatening the fovea requires treatment |
- Wills Eye Manual, p. 811; Goldman-Cecil Medicine
Ophthalmic Complications of Diabetes (Full List)
Common: Maculopathy (DME, macular ischaemia), retinopathy with neovascularisation and vitreous haemorrhage, unstable refraction
Uncommon: Recurrent styes, xanthelasma, accelerated cataract, tractional retinal detachment, neovascular glaucoma (NVG), ocular motor nerve palsies, reduced corneal sensitivity
Rare: Diabetic papillopathy, Wolfram syndrome, acute-onset cataract, rhino-orbital mucormycosis
Clinical Features and Diagnosis
DR is largely asymptomatic even with severe proliferative disease. Symptoms (blurred vision, floaters, sudden vision loss) appear only with complications like vitreous haemorrhage, macular oedema, or traction retinal detachment. - Goldman-Cecil Medicine
Workup:
- Slit-lamp examination - gonioscopy for NVI/NVA before dilation
- Dilated fundus examination (90D or 60D lens + indirect ophthalmoscopy for periphery)
- FBG, HbA1c, lipid panel
- Blood pressure
- Fluorescein angiography (IVFA) - assesses perfusion, foveal ischaemia, microaneurysms, subclinical neovascularisation
- OCT - evaluates presence and extent of DME; OCT-A can detect central macular ischaemia
Screening schedule: In type 2 DM, start at diagnosis. In type 1 DM, start 5 years after diagnosis. Routine non-dilated exams are inadequate - requires dilated exam or retinal photography with remote reading.
Differential Diagnosis
For NPDR:
- CRVO - disc swelling, more dilated/tortuous veins, NFL hemorrhages, usually unilateral
- BRVO - haemorrhages along a vein, do not cross horizontal raphe
- Hypertensive retinopathy - fewer flame-shaped haemorrhages, rare microaneurysms, AV nicking
- Ocular Ischaemic Syndrome (OIS) - midperipheral haemorrhages, pain, iris NV
For PDR:
- Sickle cell retinopathy - peripheral "sea fan" neovascularisation
- CRAO/CRVO/BRVO neovascular complications
- Sarcoidosis - "candle-wax dripping" exudates, uveitis
Treatment
1. Prevention and Systemic Control (First Priority)
- Intensive glycemic control (DCCT evidence): prevents/delays development and progression
- Note: during the first 6-12 months of improved control, established DR may transiently worsen - this is temporary
- Blood pressure control (<140/80 mmHg) - especially beneficial in type 2 maculopathy
- Fenofibrate (for elevated triglycerides) - may reduce DR progression
- Aspirin therapy does not influence the natural history of DR
- Harrison's Principles of Internal Medicine, 22nd ed.
2. Diabetic Macular Oedema (DME)
| Step | Treatment |
|---|---|
| First-line | Anti-VEGF agents (FDA-approved: ranibizumab, aflibercept; off-label: bevacizumab) for center-involving DME |
| Second-line | Intravitreal corticosteroids: FDA-approved dexamethasone implant or fluocinolone acetonide implant (for suboptimal anti-VEGF response; caution: cataract + raised IOP) |
| Alternative | Focal macular laser for extrafoveal microaneurysms; also for patients where injections are contraindicated |
3. Proliferative Diabetic Retinopathy (PDR)
Panretinal photocoagulation (PRP) is indicated for any high-risk characteristic:
- NVD > 1/4 to 1/3 disc area
- Any NVD with preretinal haemorrhage or vitreous haemorrhage (VH)
- NVE > 1/2 disc area with preretinal or VH
- Any NVI or NVA
Anti-VEGF therapy - alternative to PRP; preferred initial therapy when:
- DME co-exists
- View to peripheral retina is limited by VH
- Caution: patients lost to follow-up have worse outcomes without PRP
A 2025 meta-analysis (PMID 39128789) found anti-VEGF injections and PRP to have comparable visual outcomes for PDR, informing ongoing debate about first-line choice.
4. Vitrectomy
Indicated for:
- Dense, non-clearing or recurrent VH with significant vision loss
- Traction retinal detachment involving or progressing in the macula
- Macular epiretinal membranes or vitreomacular traction
- Dense premacular haemorrhage
- Chronic DME unresponsive to other treatment
- Severe NV with fibrous proliferation unresponsive to laser/anti-VEGF
Note: Young patients with type 1 DM tend to have more aggressive PDR and may benefit from earlier vitrectomy, laser, or anti-VEGF. B-scan ultrasound is needed to rule out traction detachment when VH obscures fundus view.
Semaglutide / GLP-1 RA Warning (2025 Update)
A 2025 systematic review (PMID 40810985) in JAMA Ophthalmology specifically evaluated ocular adverse events with semaglutide and found an increased risk of worsening diabetic retinopathy with GLP-1 receptor agonists when rapid glycemic improvement occurs. This aligns with the known "early worsening" phenomenon and is now explicitly flagged in Harrison's 22nd edition (2025) when choosing glycemic agents.
Screening Summary
| Diabetes Type | When to Start Screening | Frequency |
|---|---|---|
| Type 2 DM | At diagnosis | Annually (or more often based on severity) |
| Type 1 DM | 5 years after diagnosis | Annually |
| Pregnancy (type 1 or 2) | Before and during pregnancy | Up to every 2 weeks if DR present |
Sources:
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition
- Wills Eye Manual, Office and Emergency Room Diagnosis and Treatment of Eye Disease
- Goldman-Cecil Medicine, International Edition
- Harrison's Principles of Internal Medicine, 22nd Edition (2025)
- Robbins, Cotran & Kumar Pathologic Basis of Disease
This is a shared conversation. Sign in to Orris to start your own chat.