Difference between subdural haemorrhage and subarachnoid haemorrhage
Reading File
Finding Sources
Searching the Web
subdural haemorrhage vs subarachnoid haemorrhage differences clinical features
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed for a thorough, well-illustrated comparison. Here is the full answer:
Subdural Haemorrhage vs Subarachnoid Haemorrhage
Understanding the difference starts with anatomy. The brain is wrapped in three meningeal layers - from outside in: dura mater, arachnoid mater, pia mater. Where blood collects defines the type of haemorrhage.
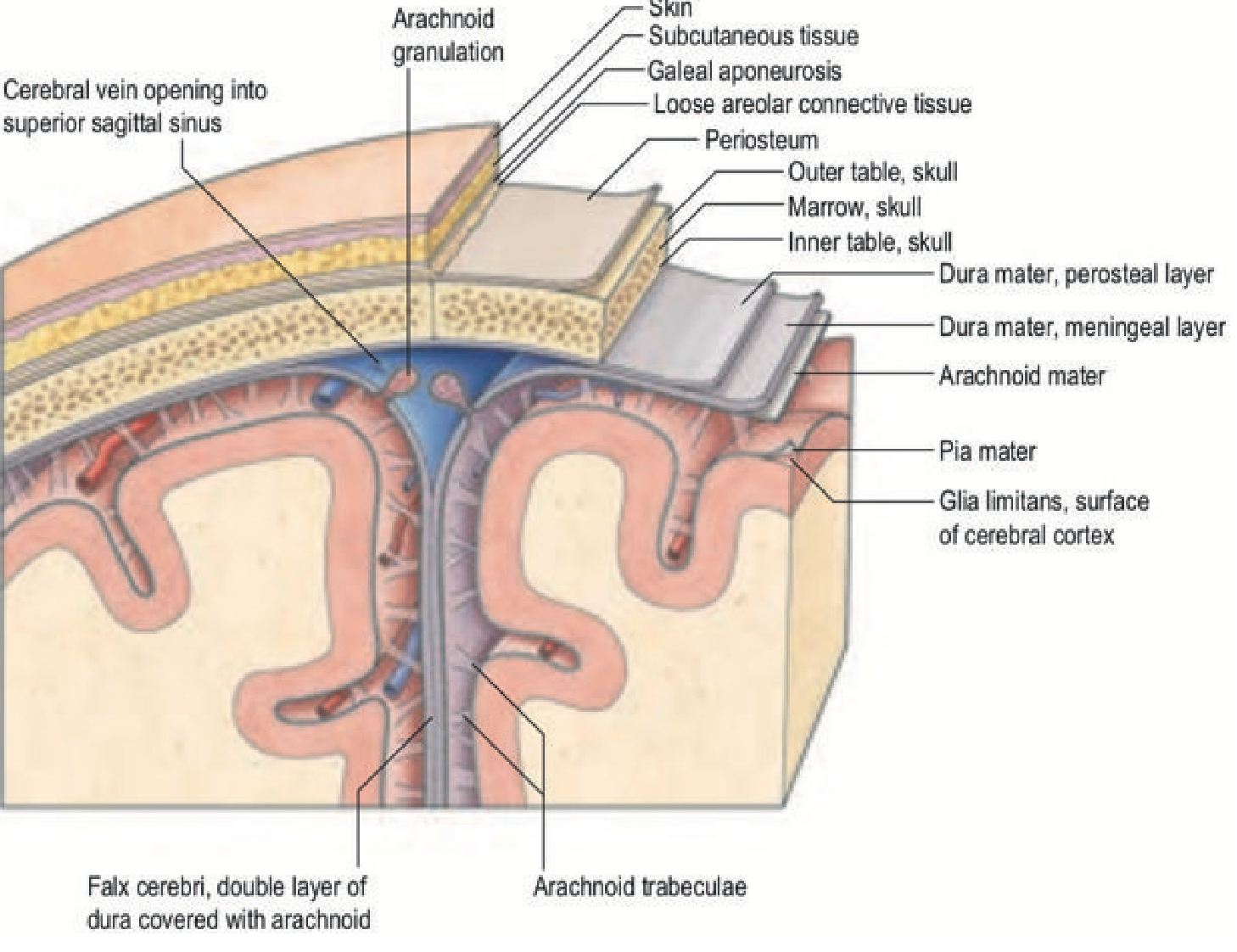
1. Location (Most Fundamental Difference)
| Feature | Subdural Haemorrhage (SDH) | Subarachnoid Haemorrhage (SAH) |
|---|---|---|
| Space | Between dura mater and arachnoid mater | Between arachnoid mater and pia mater |
| Normal space? | Potential space (not naturally present) | Subarachnoid space - contains CSF |
| Spread | Creeps over cerebral convexity, can extend to falx and tentorium | Fills basal cisterns and sulci; follows CSF pathways |
2. Aetiology and Source of Bleeding
Subdural Haemorrhage
- Almost always venous bleeding - from rupture of cortical bridging veins that extend from the cortical surface to the dural venous sinuses
- Usually traumatic (head injury, falls, acceleration-deceleration), even minor trauma in the elderly
- Risk factors: old age, cerebral atrophy (stretches bridging veins), anticoagulants, alcoholism, coagulopathy, shaken baby syndrome
- Occasionally spontaneous from a ruptured aneurysm (especially posterior communicating artery) or dural arteriovenous fistula
Subarachnoid Haemorrhage
- Usually arterial bleeding
- Spontaneous SAH: ~80% from rupture of a saccular (berry) aneurysm at arterial branch points in the circle of Willis; ~10% from non-aneurysmal perimesencephalic SAH (venous origin, excellent prognosis); remaining from AVMs, mycotic aneurysms, cocaine abuse, dissection
- Traumatic SAH is the most common cause overall, but is managed differently (conservatively, no vasospasm)
- Risk factors for aneurysmal SAH: hypertension, smoking, female sex, family history, polycystic kidney disease, Ehlers-Danlos, Marfan syndrome
"Spontaneous SAH is most commonly due to a vascular abnormality, with a ruptured aneurysm accounting for approximately 80% of SAH." - Bailey & Love's Surgery, 28th Ed.
3. Clinical Presentation
| Feature | SDH | SAH |
|---|---|---|
| Headache | Gradual, progressive | Sudden "thunderclap" headache - worst of life, often during exertion |
| Onset | Hours to weeks (depending on type) | Instantaneous ("like a bat hitting the head") |
| LOC | Gradual deterioration, confusion, drowsiness | ~50% brief unresponsiveness at ictus |
| Vomiting | Can occur | Very common (~70%) |
| Meningism | Absent (no blood in CSF space) | Present - neck stiffness, photophobia (develops over hours) |
| Seizure | Can occur | ~10% at ictus |
| Focal deficits | Common (mass effect on adjacent cortex) | May be present if poor grade; 3rd nerve palsy with PComm aneurysm |
| Prodromal symptoms | Personality change (chronic SDH) | "Sentinel headache" (aneurysm growth/minor leak) |
| Fundoscopy | Usually normal | Subhyaloid haemorrhages; Terson's syndrome (vitreous + SAH) in 15-20% |
The classic SDH presentation is a gradually worsening course after head trauma. The classic SAH presentation is a sudden, explosive headache that is qualitatively unlike any previous headache.
4. Classification (SDH specific)
SDH is uniquely classified by timing:
- Acute (<3 days): typically after high-energy trauma; urgent evacuation by craniotomy
- Subacute (3-21 days)
- Chronic (>21 days): common in elderly with cerebral atrophy; osmotic expansion of a degrading clot over weeks; burr hole drainage preferred
5. CT Imaging Appearances
SDH on CT:
- Crescentic (concave-convex) hyperdensity conforming to brain surface - no anatomical constraint because the subdural space is open
- Can extend along falx, tentorium, and floor of cranial fossae
- Acute SDH: hyperdense (white)
- Subacute SDH: isodense (hard to see, may need MRI)
- Chronic SDH: hypodense (dark), may have fluid levels or mixed density if re-bled
- May NOT have associated skull fracture (unlike extradural haematoma)
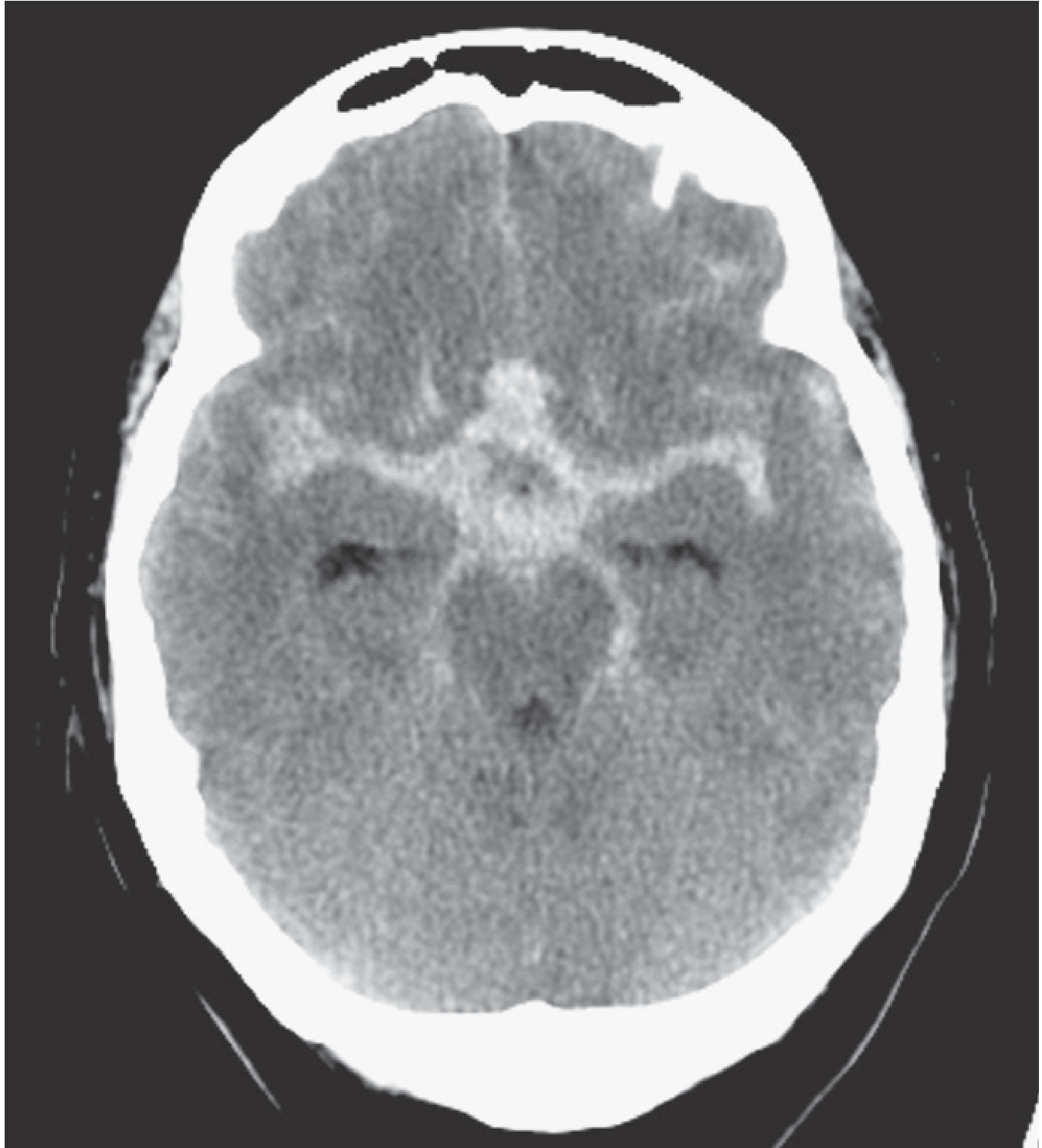
SAH on CT:
- Hyperdense blood in sulci, basal cisterns, Sylvian fissures - follows the CSF spaces
- CT sensitivity is 98% within 12 hours of ictus, falling to <75% after 24 hours
- If CT is negative but clinical suspicion high: lumbar puncture (xanthochromia) or CT angiography
6. Complications
| Complication | SDH | SAH |
|---|---|---|
| Raised ICP / mass effect | Yes - main concern | Yes, from hydrocephalus |
| Vasospasm | Not typical | Major complication (days 4-14); causes delayed ischaemic deficit |
| Hydrocephalus | Uncommon | Common (blood blocks CSF reabsorption) |
| Rebleeding | Possible (chronic SDH re-expands) | High risk if aneurysm not secured (up to 30% within 30 days) |
| Herniation | Yes, from expanding haematoma | Yes, from raised ICP |
7. Management
SDH:
- Reverse anticoagulation
- Acute SDH: urgent craniotomy
- Chronic SDH: burr hole drainage (can be done under LA even in elderly); corticosteroids for small/asymptomatic bleeds
- Conservative management for small bleeds with headache only
SAH:
- Immediate CT; if positive - CT angiography or formal digital subtraction angiography to identify aneurysm
- Aneurysm secured by neurosurgical clipping or endovascular coiling
- Nimodipine (calcium channel blocker) to reduce vasospasm
- Treat hydrocephalus (external ventricular drain if needed)
- Mortality approaches 50%; post-ictus dependency ~30%
- About one-third of SAHs are missed at initial presentation - a significant diagnostic pitfall
Summary Table
| Feature | SDH | SAH |
|---|---|---|
| Space | Dura-arachnoid | Arachnoid-pia |
| Bleeding source | Bridging veins (venous) | Aneurysm (arterial) |
| Cause | Trauma, falls | Aneurysm rupture, trauma |
| Headache | Gradual/chronic | Thunderclap |
| Meningism | No | Yes |
| CT shape | Crescent | Fills sulci/cisterns |
| Vasospasm | No | Yes |
| Treatment | Burr hole / craniotomy | Coiling / clipping + nimodipine |
| Prognosis | Variable (chronic better) | ~50% mortality |
Sources: Grainger & Allison's Diagnostic Radiology; Bailey & Love's Short Practice of Surgery, 28th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.