VAS score properly
Reading File
Searching the Web
VAS visual analogue scale pain score how to use properly
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a complete guide on how to use the VAS score properly:
Visual Analogue Scale (VAS) - Proper Use
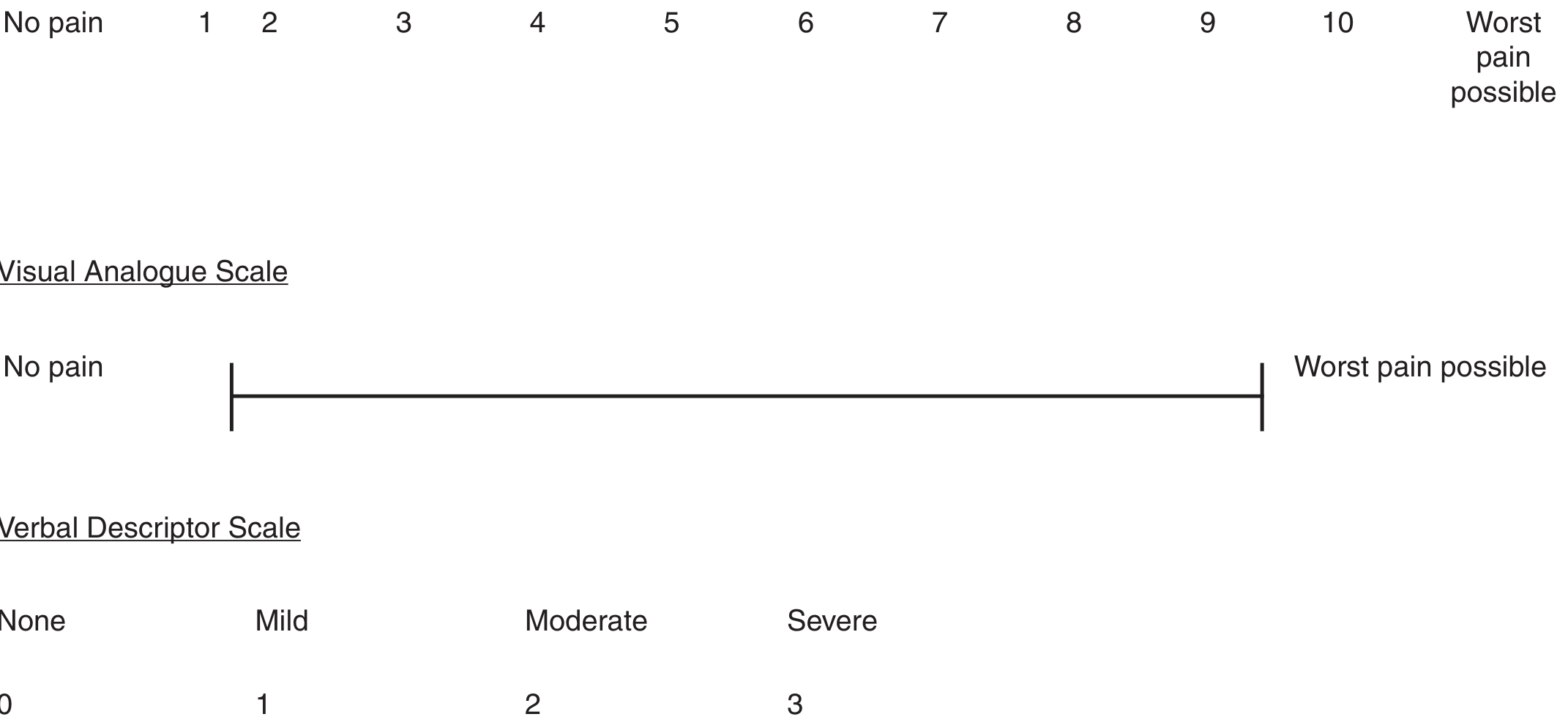
Pain scales from Rosen's Emergency Medicine - NRS (top), VAS (middle), Verbal Descriptor Scale (bottom)
What is the VAS?
The VAS is a unidimensional instrument for subjective rating of pain intensity. It consists of a 10 cm (100 mm) horizontal straight line with two anchor points:
- Left end (0): "No pain"
- Right end (100 mm / 10): "Worst pain possible"
There are no numbers or intermediate markings on the line itself - this is what distinguishes it from the Numerical Rating Scale (NRS).
How to Administer It Properly
Step 1 - Present the scale
Show the patient the 10 cm line on paper (or a printed card). Do not show the back (where the measurement is). The line must have no intermediate labels or tick marks.
Step 2 - Give clear instructions
Tell the patient: "Please make a mark on this line to show how much pain you are feeling right now. The left end means no pain at all. The right end means the worst pain you can possibly imagine."
Step 3 - Patient marks their pain
The patient places a single vertical mark anywhere on the line corresponding to their current pain.
Step 4 - Measure and record
Using a ruler, measure the distance in millimeters from the left (zero) end to the patient's mark. That number (0-100 mm) is the VAS score.
Scoring Interpretation
| VAS Score | Pain Category |
|---|---|
| 0-4 mm | No pain |
| 5-44 mm | Mild pain |
| 45-74 mm | Moderate pain |
| 75-100 mm | Severe pain |
Note: These category cutoffs are conventional but somewhat arbitrary and do not always perfectly reflect an individual patient's meaning.
Key Rules for Proper Use
- Paper only - The standard VAS must be administered on paper, not verbally. Verbal administration defeats the purpose of the visual/continuous format.
- No intermediate numbers or labels on the line (that becomes an NRS).
- One mark only - instruct the patient to make a single vertical line.
- Measure in mm - not cm, not a 0-10 conversion. The raw mm score (0-100) is the VAS score.
- Current pain - ask the patient to rate pain "right now," unless you specifically want average or worst pain over a period.
- Treat sequentially - after analgesic intervention, re-administer and track change. A clinically meaningful change is generally considered ≥13-15 mm on the 0-100 scale.
VAS vs. NRS - Key Distinction
| Feature | VAS | NRS (Numeric Rating Scale) |
|---|---|---|
| Format | Blank 10 cm line | 0-10 numbered scale |
| Administration | Paper only | Verbal or written |
| Data type | Continuous | Discrete (integers) |
| Research utility | Higher (continuous data) | Practical in clinical setting |
| Cognitive demand | Slightly higher | Lower |
As Rosen's Emergency Medicine notes: "Visual analogue scales...are frequently used in research to provide continuous data for analysis. These scales offer little practical advantage over verbal reports in the clinical setting."
Special Populations
- Children < 7 years: Use the FACES Pain Scale (cartoon faces from happy to distressed) - the VAS is too abstract.
- Cognitively impaired / preverbal: Use observer-derived scales (CHEOPS, CRIES, M-PEPPS).
- Elderly or cognitively limited adults: The NRS (verbal 0-10) is often better tolerated.
Treatment Targeting
Pain treatment should aim to reduce the VAS score by 50%, bring it below 40/100, or shift it into the mild category - rather than chasing a specific analgesic dose. Re-assess after every intervention.
- Rosen's Emergency Medicine, Concepts and Clinical Practice
- Harrison's Principles of Internal Medicine, 22nd Edition
- Scott-Brown's Otorhinolaryngology, Head & Neck Surgery
This is a shared conversation. Sign in to Orris to start your own chat.