Tell me everything about renal anatomy and physiology from basics to clinicals. Also include diagrams and illustration
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Renal Anatomy and Physiology: Basics to Clinicals
PART 1 - GROSS ANATOMY
Position and Dimensions
The kidneys are paired retroperitoneal organs sitting on the posterior abdominal wall, on either side of the vertebral column at the level of T12-L3. The right kidney is positioned slightly lower than the left due to the liver. Each kidney is:
- Length: ~11 cm
- Width: ~6 cm
- Thickness: ~3 cm
- Weight: ~150 g (male), ~135 g (female)
The kidneys are surrounded by perinephric fat, enclosed in the renal (Gerota's) fascia, and lie anterior to the psoas major and quadratus lumborum muscles.
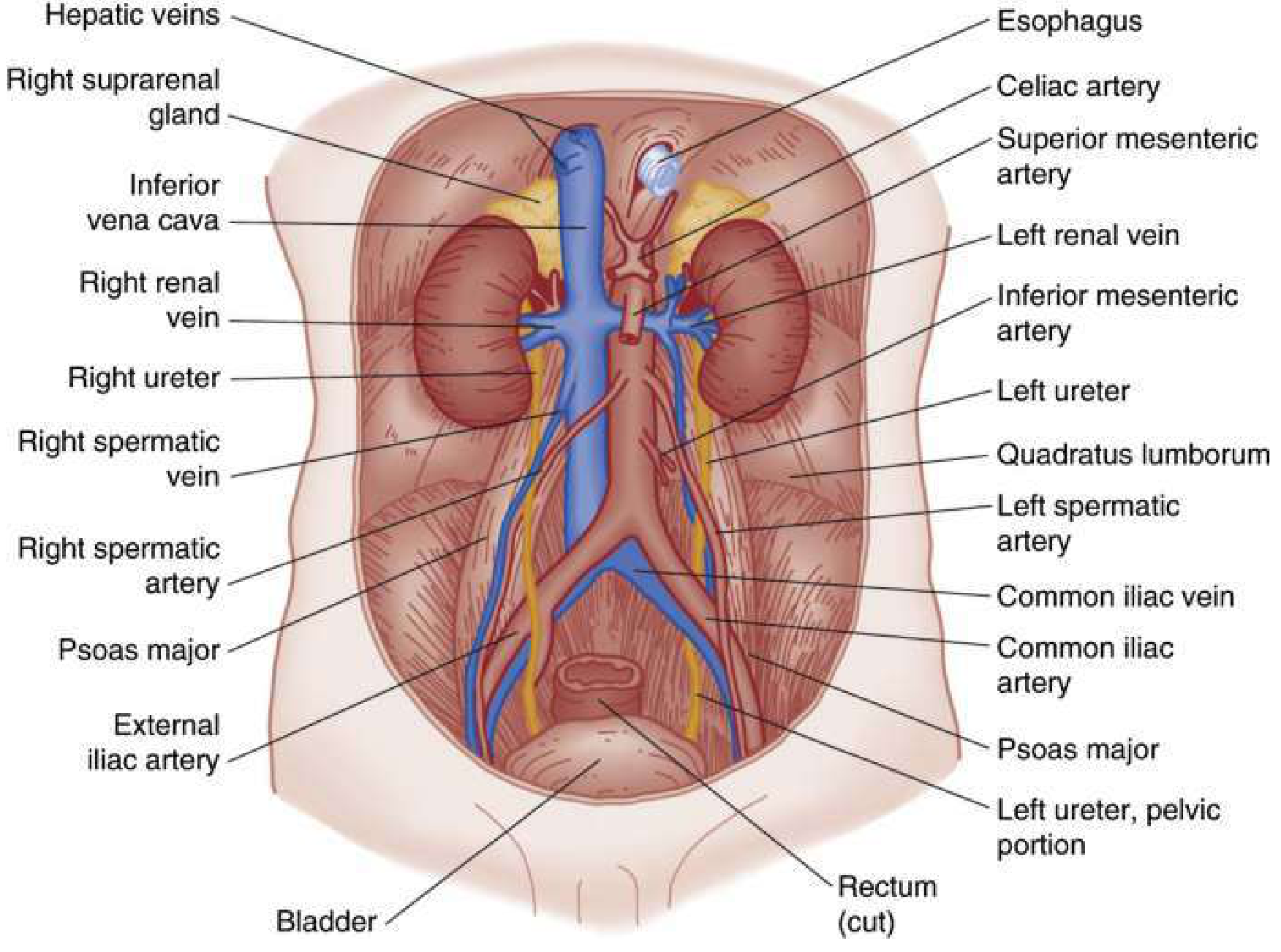
Retroperitoneal relations - anterior view:
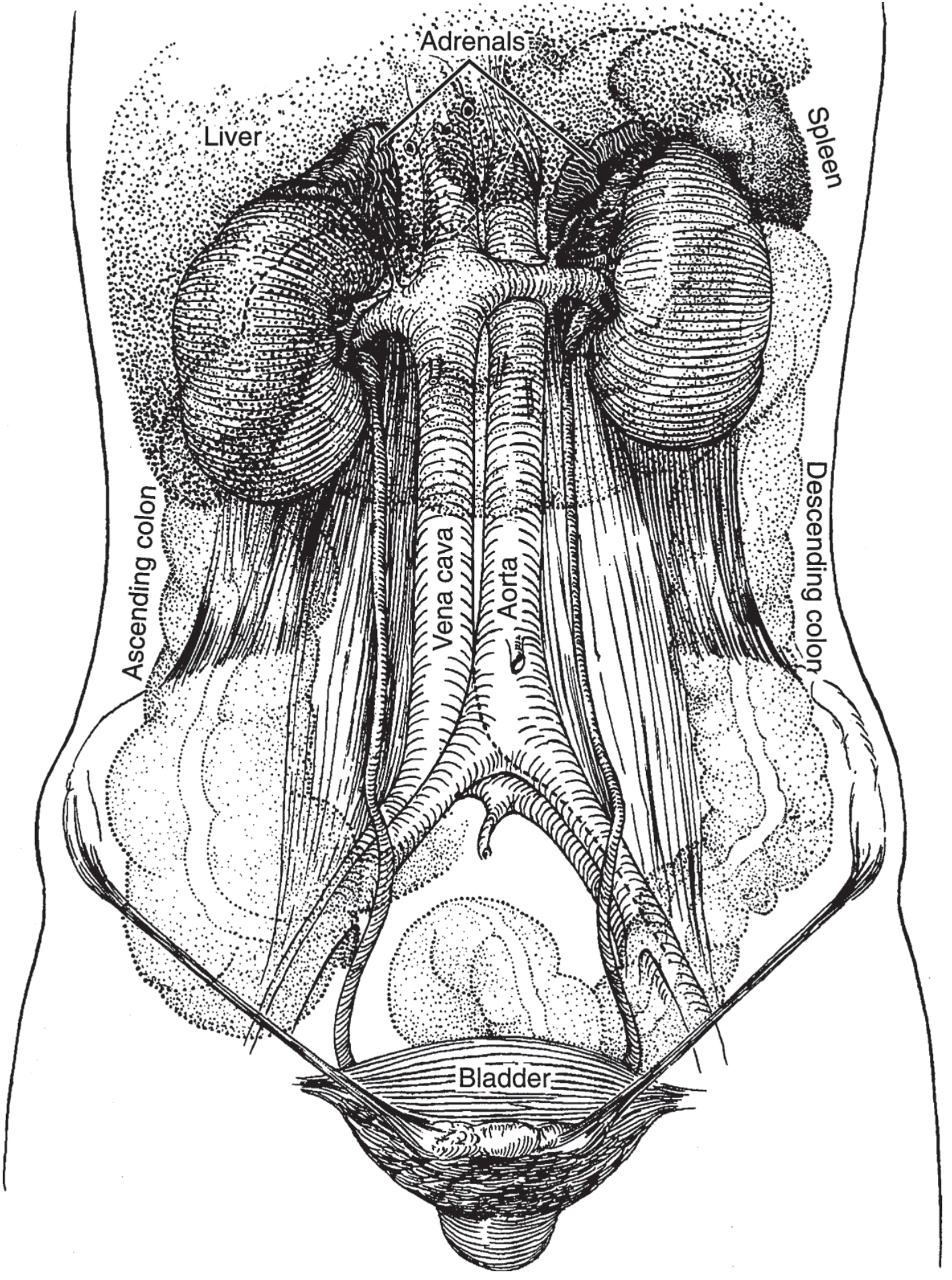
Detailed anterior relations with vasculature:
Internal Architecture
On longitudinal section, the kidney has three concentric zones:
- Cortex - outer, homogeneous. Contains glomeruli, proximal and distal convoluted tubules. Cortical columns (columns of Bertin) project inward between the pyramids.
- Medulla - inner, striated. Made up of 8-18 renal pyramids whose bases face the cortex and whose apices (papillae) project into the minor calyces.
- Collecting system - minor calyces (8-12) drain the papillae → major calyces (2-3) → renal pelvis → ureter.
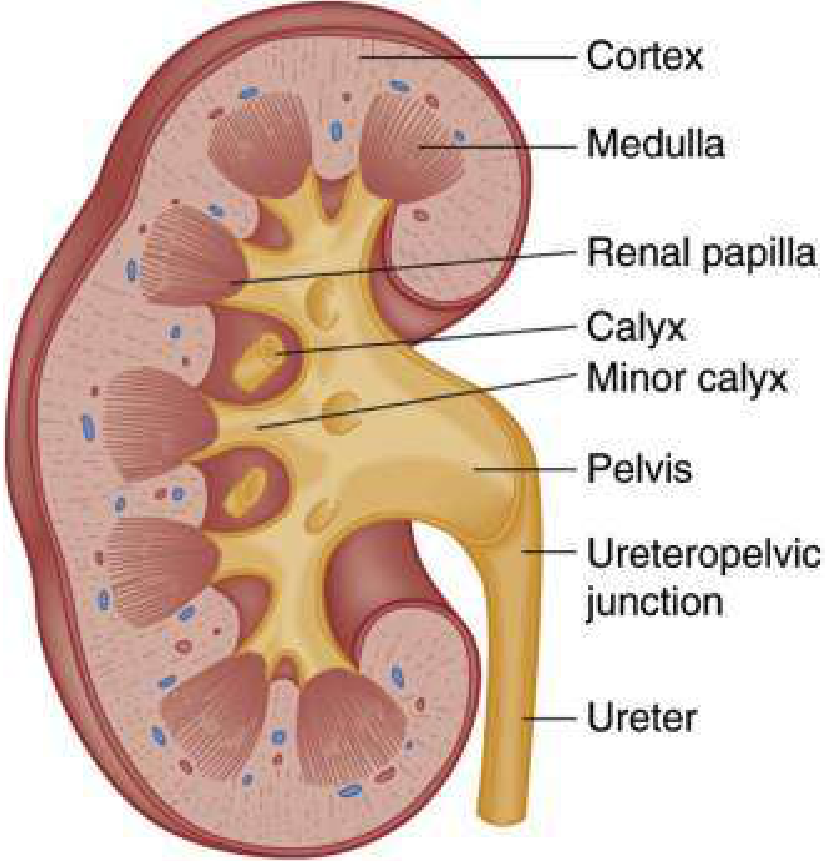
"On longitudinal section, the kidney is seen to be made up of an outer cortex, a central medulla, and the internal calices and pelvis. Portions of the cortex project toward the pelvis between the papillae — the columns of Bertin." - Smith & Tanagho's General Urology
Vascular Supply
The renal artery branches from the abdominal aorta at L1-L2. It divides at the hilum into:
- Segmental arteries (5 segments: superior, antero-superior, antero-inferior, inferior, posterior)
- Lobar arteries (1 per pyramid)
- Interlobar arteries (between pyramids)
- Arcuate arteries (run along corticomedullary junction)
- Interlobular/cortical radial arteries (ascend through cortex)
- Afferent arterioles (feed each glomerulus)
After filtration, blood exits via the efferent arteriole, which then forms either:
- Peritubular capillaries (cortical nephrons) - supply proximal and distal tubules
- Vasa recta (juxtamedullary nephrons) - descend into the medulla, critical for urine concentration
Venous drainage is roughly the mirror image: the renal vein drains into the inferior vena cava. Notably, the left renal vein is longer and crosses anterior to the aorta; the right gonadal vein drains into the IVC directly, while the left gonadal vein drains into the left renal vein.
Clinical point: Because the right renal vein is shorter, right-sided renal tumors carry higher risk of IVC invasion.
PART 2 - HISTOLOGY: THE NEPHRON
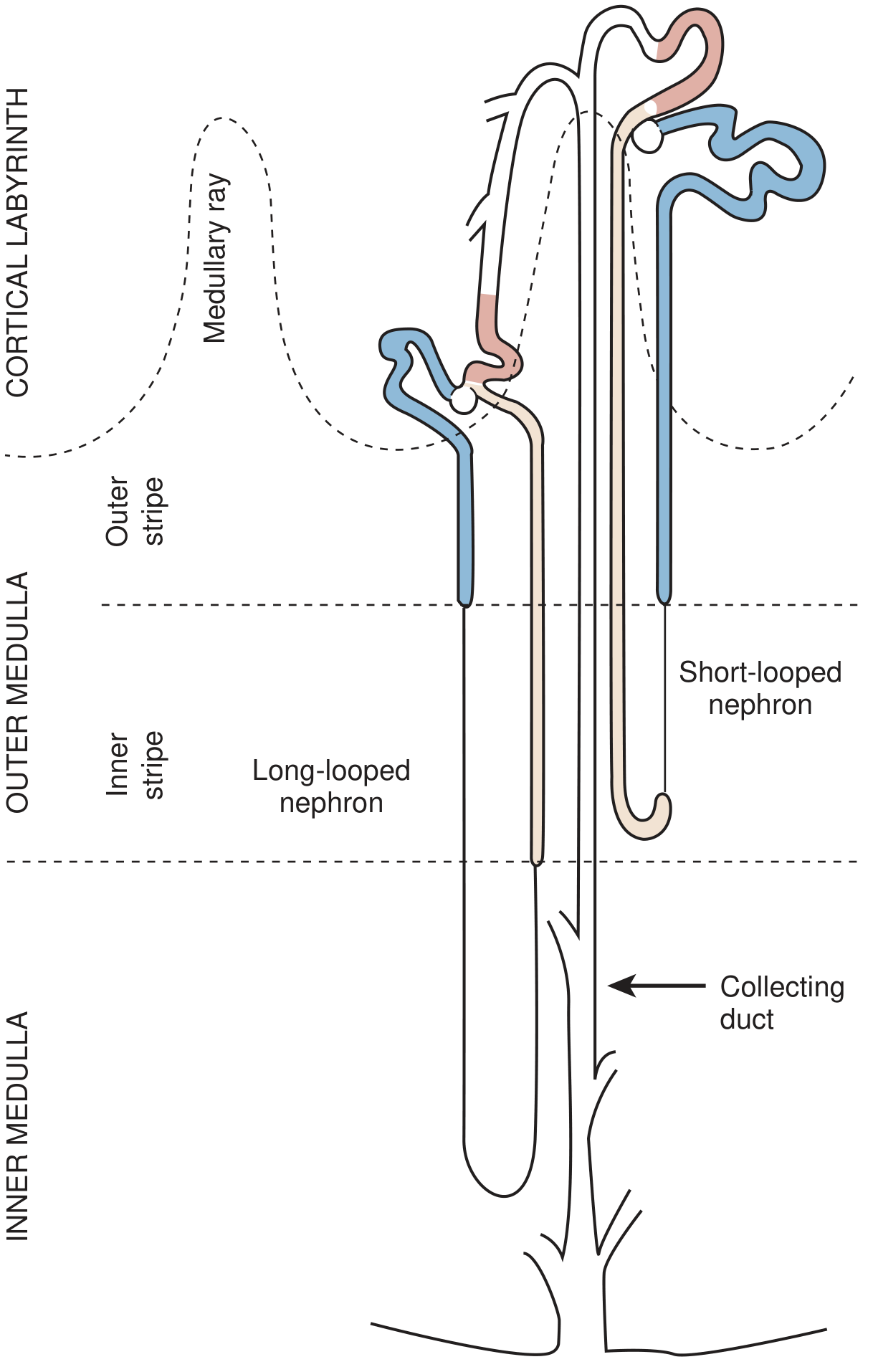
The nephron is the functional unit of the kidney. Each kidney contains approximately 1-1.2 million nephrons. The nephron has a secretory portion (mostly cortical) and an excretory portion (medullary).
Nephron types:
| Type | Location of glomerulus | Loop of Henle depth |
|---|---|---|
| Cortical (85%) | Outer/mid-cortex | Short loop (stays in outer medulla) |
| Juxtamedullary (15%) | Deep cortex near corticomedullary junction | Long loop (descends deep into inner medulla) - KEY for urine concentration |
Segments of the Nephron
1. Renal Corpuscle (Bowman's capsule + Glomerulus)
- The glomerulus is a tuft of fenestrated capillaries enclosed in Bowman's capsule
- Filtration barrier = fenestrated endothelium + glomerular basement membrane (GBM) + podocyte foot processes with slit diaphragms
- Parietal epithelium of Bowman's capsule is continuous with the proximal convoluted tubule
2. Proximal Convoluted Tubule (PCT)
- Lined with tall, brush-border columnar cells (abundant microvilli for surface area)
- Reabsorbs ~65-70% of filtered Na⁺, water, K⁺, HCO₃⁻, glucose (100%), amino acids, phosphate, and uric acid
- Site of active secretion of organic acids and bases
- Highly susceptible to ischemic injury (AKI) due to high metabolic demand and dependence on aerobic metabolism
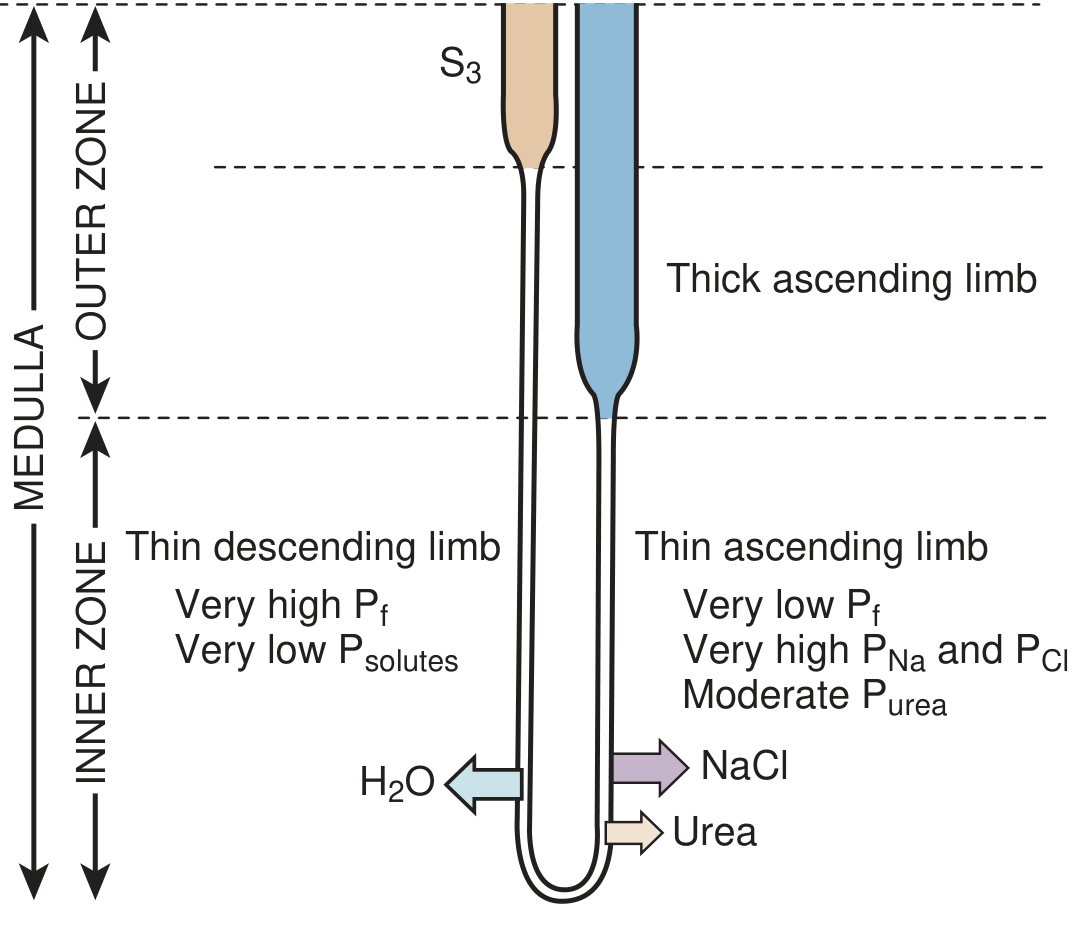
3. Loop of Henle
- Thin descending limb: highly water-permeable, poorly permeable to solutes - water exits by osmosis as tubular fluid descends into the hypertonic medullary interstitium
- Thin ascending limb: water-impermeable, NaCl diffuses out passively
- Thick ascending limb (TAL): water-impermeable; Na⁺-K⁺-2Cl⁻ cotransporter (NKCC2) actively reabsorbs NaCl - the diluting segment; site of action of loop diuretics (furosemide)
4. Distal Convoluted Tubule (DCT)
- Reabsorbs NaCl via Na⁺-Cl⁻ cotransporter (NCC) - site of action of thiazide diuretics
- Responds to PTH (phosphate excretion, Ca²⁺ reabsorption) and aldosterone
- Contains the macula densa cells (part of the juxtaglomerular apparatus - see below)
5. Collecting Duct
- Passes from cortex through medulla to papilla
- Two cell types:
- Principal cells: Na⁺ reabsorption (ENaC), K⁺ secretion; regulated by aldosterone; site of action of K⁺-sparing diuretics (amiloride, spironolactone)
- Intercalated cells (A and B type): H⁺ secretion and HCO₃⁻ reabsorption (type A) or H⁺ reabsorption and HCO₃⁻ secretion (type B) - acid-base regulation
- Water reabsorption via aquaporin-2 (AQP2) channels, regulated by ADH/vasopressin (V2 receptors)
Full nephron and renal vasculature illustrated:
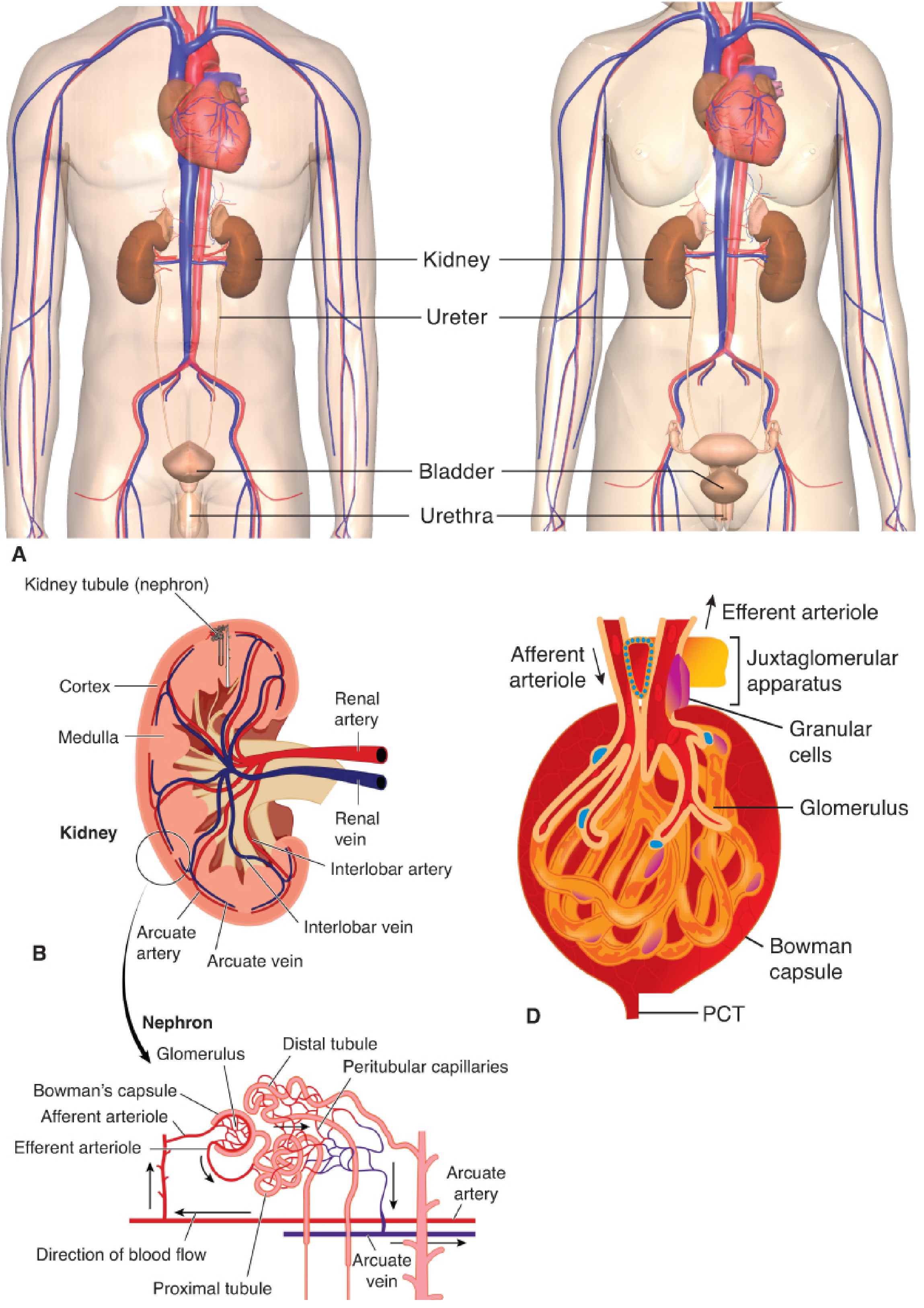
Juxtaglomerular Apparatus (JGA)
The JGA is a specialized structure at the vascular pole of each glomerulus composed of:
- Macula densa - specialized cells in the thick ascending limb/early DCT that sense luminal NaCl concentration
- Juxtaglomerular (granular) cells - modified smooth muscle cells in the afferent arteriole wall; synthesize and store renin
- Extraglomerular mesangial (Lacis) cells - connect the two; precise function unclear
Function: When NaCl delivery to the macula densa falls (low GFR or low blood volume), renin is released → activates RAAS → angiotensin II → efferent arteriolar constriction → maintains GFR. This is tubuloglomerular feedback.
PART 3 - PHYSIOLOGY
3.1 Glomerular Filtration
The kidneys receive 25% of cardiac output (~1.2 L/min), despite comprising only 0.4% of body weight. Of the renal plasma flow (~650 mL/min), approximately 20% is filtered at the glomerulus = GFR ~120-125 mL/min in a healthy adult.
Determinants of GFR (Starling forces across the glomerulus):
GFR = Kf × (Pₐc - Pbs - πₐc + πbs)
Where:
- Kf = ultrafiltration coefficient (permeability × surface area)
- Pₐc = glomerular capillary hydrostatic pressure (~55 mmHg) - promotes filtration
- Pbs = Bowman's space hydrostatic pressure (~15 mmHg) - opposes filtration
- πₐc = glomerular capillary oncotic pressure (~30 mmHg) - opposes filtration
- πbs = Bowman's space oncotic pressure (~0 mmHg) - promotes filtration
- Net filtration pressure ≈ 10 mmHg
Afferent vs. efferent arteriolar tone:
- Afferent dilation / efferent constriction → ↑ GFR
- Afferent constriction (angiotensin II, intense sympathetics) → ↓ GFR
- NSAIDs block prostaglandin-mediated afferent dilation → ↓ GFR (especially dangerous in low-flow states)
- ACE inhibitors / ARBs dilate efferent arteriole → ↓ efferent resistance → ↓ GFR (important in bilateral renal artery stenosis)
3.2 Autoregulation of Renal Blood Flow
The kidney maintains relatively constant RBF and GFR over a wide range of mean arterial pressures (approximately 70-170 mmHg) via two mechanisms:
- Myogenic reflex - increased pressure stretches afferent arteriolar wall → reflex constriction
- Tubuloglomerular feedback - macula densa senses ↓ chloride delivery → signals afferent arteriole to dilate → ↑ GFR
Clinical implication: Below MAP of ~50-70 mmHg, autoregulation fails and GFR falls linearly - this is why severe hypotension causes acute kidney injury.
3.3 Tubular Function: Reabsorption and Secretion
Of the ~180 L of filtrate produced per day, only ~1.5-2 L becomes urine. The tubular system reabsorbs over 99% of the filtrate.
Summary of tubular transport by segment:
| Segment | Key reabsorbed substances | Key secreted | Diuretic target |
|---|---|---|---|
| PCT | 65% Na⁺, H₂O; 100% glucose/amino acids; 80% HCO₃⁻; uric acid | H⁺, organic acids/bases, drugs | Carbonic anhydrase inhibitors (acetazolamide) |
| Thin descending loop | H₂O (via AQP1) | - | - |
| Thick ascending loop | Na⁺-K⁺-2Cl⁻ (no water) | - | Loop diuretics (furosemide) |
| DCT | NaCl (NCC) | - | Thiazides |
| Collecting duct | Na⁺ (ENaC, aldosterone), H₂O (ADH/AQP2) | K⁺, H⁺ | Aldosterone antagonists, amiloride |
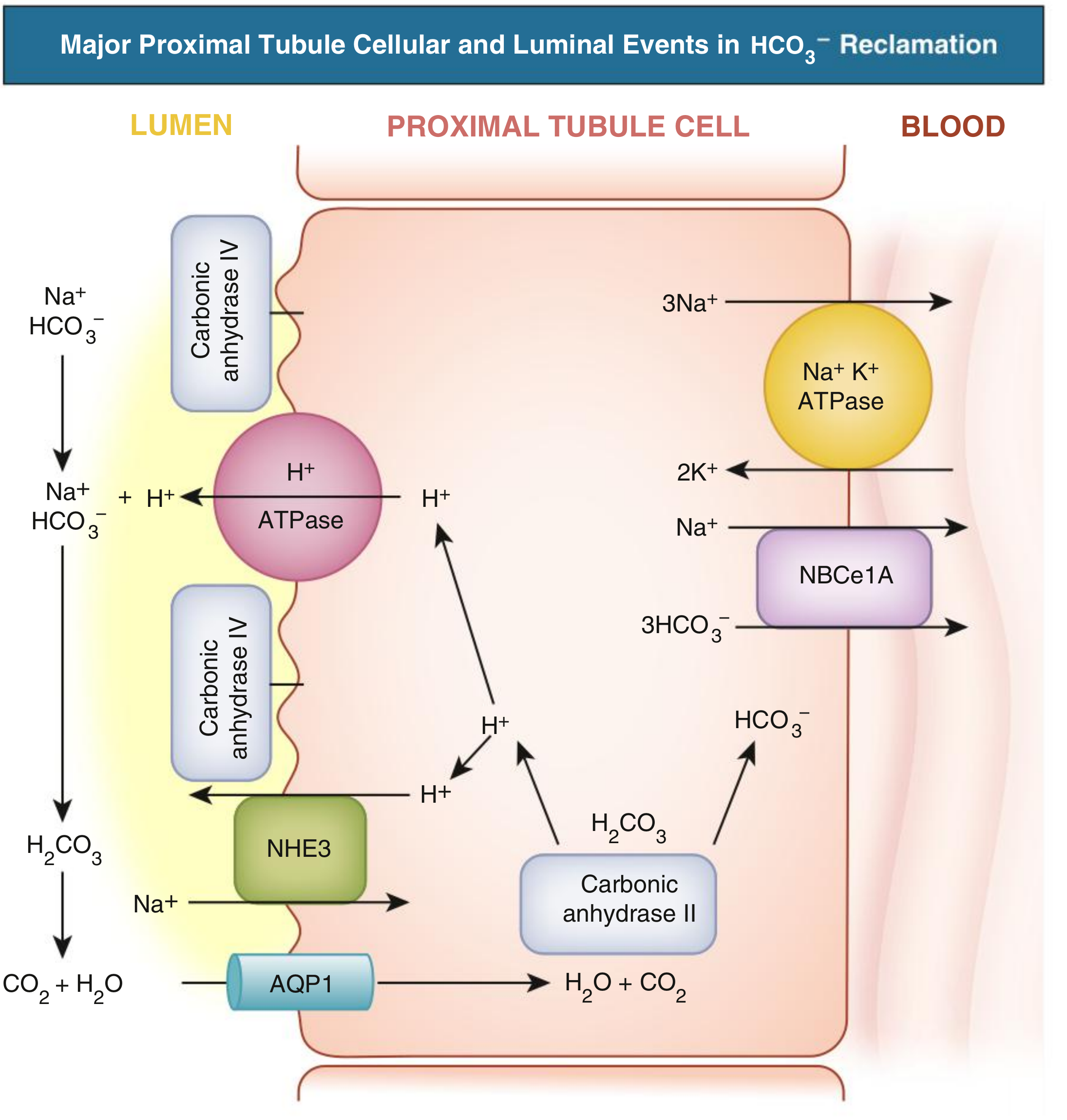
3.4 Proximal Tubular HCO₃⁻ Reclamation (Acid-Base)
About 80% of filtered HCO₃⁻ is reclaimed in the PCT via H⁺ secretion through the Na⁺/H⁺ exchanger (NHE3). The secreted H⁺ combines with luminal HCO₃⁻ → H₂CO₃ → CO₂ + H₂O (catalyzed by luminal carbonic anhydrase IV). CO₂ enters the cell via AQP1, and intracellular carbonic anhydrase II regenerates HCO₃⁻, which exits the basolateral membrane via the electrogenic NBCe1A cotransporter.
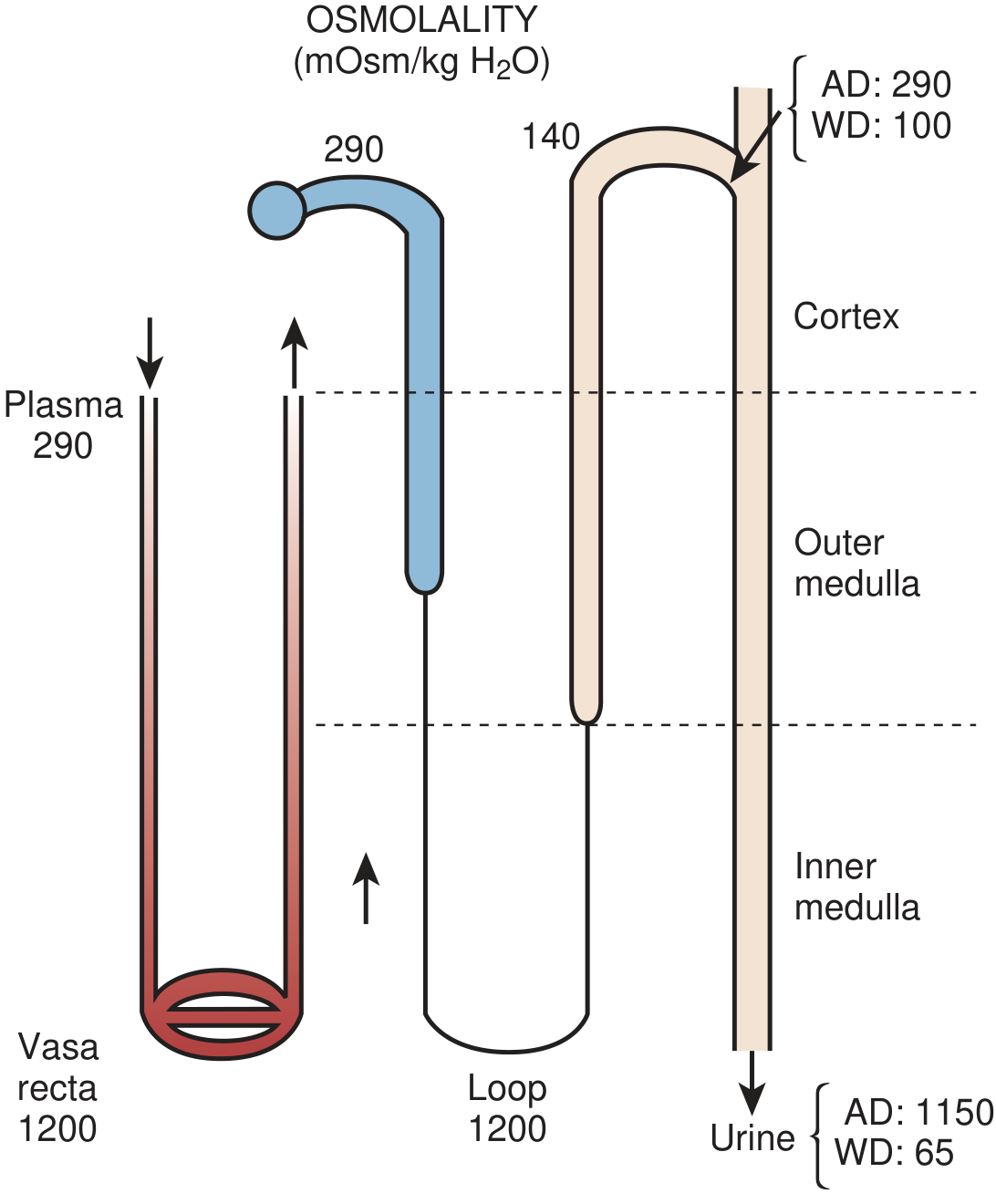
3.5 Urine Concentration: The Countercurrent System
The ability to concentrate urine (up to 1200 mOsm/kg in antidiuresis vs. ~50 mOsm/kg in water diuresis) depends on:
- Countercurrent multiplication by the loop of Henle - builds a hyperosmotic medullary interstitium (gradient from ~300 mOsm at the corticomedullary junction to ~1200 mOsm at the papilla)
- Countercurrent exchange by vasa recta - preserves the interstitial gradient
- ADH-mediated water reabsorption in the collecting duct via AQP2
The thick ascending limb pumps NaCl out without water → dilutes tubular fluid → builds interstitial hypertonicity → collecting duct fluid equilibrates with this concentrated interstitium (only when ADH opens AQP2).
Urea recycling in the inner medulla also contributes ~400-500 mOsm to the papillary interstitium.
3.6 RAAS - The Renin-Angiotensin-Aldosterone System
| Step | Location | Signal |
|---|---|---|
| Renin release (JG cells) | Afferent arteriole | ↓ perfusion pressure, ↓ NaCl at macula densa, ↑ sympathetics (β₁) |
| Angiotensinogen → Angiotensin I | Liver | Always present |
| Angiotensin I → Angiotensin II | Lung (ACE) | Constant conversion |
| Angiotensin II effects | Multiple | Efferent vasoconstriction, PCT Na⁺ reabsorption, aldosterone release, ADH release, vasoconstriction, thirst |
| Aldosterone effects | Collecting duct principal cells | ↑ ENaC, ↑ Na⁺-K⁺-ATPase → Na⁺ retention, K⁺ secretion |
3.7 Vasodilator Mechanisms (opposing RAAS)
- Atrial Natriuretic Peptide (ANP): released by atria with volume overload → ↑ GFR, ↓ Na⁺ reabsorption in collecting duct, ↓ renin, ↓ aldosterone
- Nitric oxide (NO): produced in renal vasculature → opposes angiotensin II vasoconstriction, promotes natriuresis
- Prostaglandins (PGE₂, PGI₂): dilate afferent arteriole → maintain RBF during stress; NSAIDs block this, explaining their nephrotoxicity in low-flow states
PART 4 - ENDOCRINE FUNCTIONS OF THE KIDNEY
| Hormone | Synthesized in | Stimulus | Target | Effect |
|---|---|---|---|---|
| Erythropoietin (EPO) | Peritubular fibroblasts (cortex/outer medulla) | Hypoxia | Bone marrow | ↑ Red blood cell production |
| 1,25-dihydroxyvitamin D₃ (Calcitriol) | Proximal tubule (1α-hydroxylase) | ↓ Ca²⁺, ↓ PO₄, ↑ PTH | Gut, bone, kidney | ↑ Ca²⁺ and PO₄ absorption |
| Renin | JG cells | ↓ BP, ↓ NaCl, ↑ sympathetics | Angiotensinogen | Activates RAAS |
PART 5 - MEASUREMENT OF KIDNEY FUNCTION
GFR
Normal average GFR: ~130 mL/min/1.73 m² in young men; ~120 mL/min/1.73 m² in young women. GFR declines approximately 10% per decade after age 30.
CKD staging (GFR-based):
| Stage | GFR (mL/min/1.73 m²) | Description |
|---|---|---|
| G1 | ≥ 90 | Normal/high |
| G2 | 60-89 | Mildly decreased |
| G3a | 45-59 | Mildly-moderately decreased |
| G3b | 30-44 | Moderately-severely decreased |
| G4 | 15-29 | Severely decreased |
| G5 | < 15 | Kidney failure |
Clinical note: A GFR below 60 mL/min meets criteria for CKD; below 15 mL/min is associated with uremic symptoms and may require dialysis.
Creatinine
- Produced by skeletal muscle from creatine at a constant rate
- Freely filtered; small amount secreted by tubules (so creatinine clearance slightly overestimates true GFR by ~10-15%)
- eGFR calculated from serum creatinine using CKD-EPI or MDRD equations, adjusted for age, sex, race
Cystatin C
- Freely filtered, not secreted; better marker than creatinine for early CKD and muscle-wasting states
PART 6 - CLINICAL CORRELATIONS
Acute Kidney Injury (AKI)
Classified by mechanism:
- Pre-renal: ↓ perfusion (hypovolemia, sepsis, heart failure) → RAAS activation, oliguria; FENa < 1%, BUN:Cr > 20:1; responds to volume
- Intrinsic renal: ATN (PCT most vulnerable - ischemia/contrast/aminoglycosides), glomerulonephritis, AIN; FENa > 2%, muddy brown casts in urine
- Post-renal: obstruction (stones, BPH, tumor); bilateral obstruction causes hydronephrosis
Nephrotic vs. Nephritic Syndrome
| Feature | Nephrotic | Nephritic |
|---|---|---|
| Proteinuria | > 3.5 g/day | < 3.5 g/day (subnephrotic) |
| Hematuria | Minimal | Prominent (RBC casts) |
| Edema | Massive | Mild |
| BP | Variable | Hypertension |
| Mechanism | Podocyte / GBM permeability | Inflammatory glomerulonephritis |
| Examples | MCD, FSGS, membranous nephropathy | IgA nephropathy, post-strep GN, RPGN |
CKD Consequences
Following from the physiology above, CKD causes predictable hormonal failures:
- Anemia (↓ EPO)
- Renal osteodystrophy (↓ calcitriol → ↓ Ca²⁺ absorption → secondary hyperparathyroidism → bone resorption; also ↑ FGF-23 → phosphaturia)
- Metabolic acidosis (↓ NH₄⁺ excretion, loss of acid-secreting nephron mass)
- Hyperkalemia (↓ K⁺ secretion in DCT/collecting duct)
- Hypertension (volume retention, ↑ RAAS)
- Uremia (accumulation of nitrogenous waste: urea, creatinine, uremic toxins)
Drug Dosing in Renal Failure
Since many drugs are renally cleared (aminoglycosides, vancomycin, digoxin, metformin, most beta-lactams), GFR must be assessed before prescribing. Key nephrotoxins to avoid in renal impairment include:
- NSAIDs (block prostaglandin-mediated afferent dilation)
- IV contrast (vasoconstriction + direct tubular toxicity)
- Aminoglycosides (proximal tubular accumulation)
- Metformin (risk of lactic acidosis when GFR < 30)
Summary Diagram Reference
| Diagram | What it shows |
|---|---|
| Longitudinal kidney section | Cortex, medulla, papillae, calyces, pelvis, UPJ |
| Retroperitoneal anatomy | Kidney relations to aorta, IVC, adrenals, ureters |
| Full nephron + vasculature | Glomerulus, Bowman's capsule, tubule segments, arterioles |
| Nephron organization | Short vs. long loops, cortical labyrinth, medullary ray |
| Loop of Henle anatomy | Thin/thick limbs, H₂O vs. NaCl/urea permeability |
| Countercurrent diagram | Osmolality gradient, vasa recta, antidiuresis vs. diuresis |
| Proximal tubule HCO₃⁻ reclamation | NHE3, CAII, CAIV, AQP1, NBCe1A transporters |
Sources:
- Smith & Tanagho's General Urology, 19e - Gross anatomy and nephron histology
- Barash's Clinical Anesthesia, 9e - Glomerular filtration, autoregulation, RAAS
- Campbell-Walsh-Wein Urology - Nephron organization and loop of Henle diagrams
- NKF Primer on Kidney Diseases, 8e - GFR measurement and CKD staging
- Comprehensive Clinical Nephrology, 7e - Proximal tubule HCO₃⁻ transport
- Brenner & Rector's The Kidney - Advanced physiology and clinical correlates
This is a shared conversation. Sign in to Orris to start your own chat.