Can u make a flow chart of cerebral Palsy in peadiatrics
A detailed medical flowchart titled "Cerebral Palsy in Paediatrics" with a clean clinical design on a white background. The flowchart should follow this exact structure top to bottom: START BOX (blue): "Child presents with motor delay / abnormal tone / movement disorder" Arrow down to DEFINITION BOX (dark blue): "CEREBRAL PALSY (CP) - Group of permanent, non-progressive disorders of movement & posture due to disturbance in developing fetal or infant brain" Arrow down to DIAGNOSTIC CRITERIA BOX (dark teal, 5 bullet points): "Diagnosis requires ALL of: • Disorder of movement/posture (onset <2 years) • Evidence of fetal/infant brain disturbance • Non-progressive over time • Significant functional limitation • Expected to persist lifelong" Arrow down to AETIOLOGY box (orange, 3 columns): "PRENATAL (80%): Hypoxia-ischaemia, Infection (TORCH), Stroke, Brain malformations, Genetic PERINATAL: Birth asphyxia, Prematurity, Low birth weight, Periventricular leukomalacia POSTNATAL: Meningitis, Encephalitis, Head injury, Hypoglycaemia" Arrow down to CLASSIFICATION heading Then the flowchart splits into TWO parallel paths: LEFT PATH - PHYSIOLOGICAL TYPE (green box): Split into 4 branches: 1. SPASTIC (most common, 70-80%): pyramidal tract, hypertonicity, brisk reflexes, Babinski+ 2. DYSKINETIC (10-15%): extrapyramidal - Dystonic (sustained muscle contractions) | Choreoathetoid (involuntary writhing) 3. ATAXIC (5-10%): cerebellar involvement, unsteady gait, intention tremor 4. MIXED: combinations of above RIGHT PATH - TOPOGRAPHIC DISTRIBUTION (purple box): Split into 4 branches: 1. HEMIPLEGIA (30%): one side, UE > LE 2. DIPLEGIA (50%, most common): all 4 limbs, LE > UE, common in prematurity 3. QUADRIPLEGIA: all 4 limbs equally, severe cognitive deficits common 4. TOTAL BODY: quadriplegia + loss of head/neck control Both paths rejoin into GMFCS CLASSIFICATION box (dark navy): "Gross Motor Function Classification System (GMFCS) Level I: Walks without restrictions Level II: Walks with limitations Level III: Walks with assistive device Level IV: Self-mobility limited (may use powered chair) Level V: Fully dependent, transported in manual wheelchair" Arrow down to INVESTIGATIONS box (grey): "• MRI brain (method of choice) - identifies lesion • EEG if seizures suspected • Metabolic/genetic workup if red flags • Ophthalmological & audiological assessment • Developmental assessment" Arrow down to MANAGEMENT (wide red-orange box) with 5 columns: "PHYSIOTHERAPY: Tone management, stretching, gait training | PHARMACOLOGICAL: Baclofen (spasticity), Botulinum toxin A, Diazepam, Trihexyphenidyl (dystonia) | ORTHOPAEDIC: AFOs/splints, Tendon lengthening, SDR (selective dorsal rhizotomy), Hip surveillance | NEUROLOGICAL: Seizure management (AEDs), ITB (intrathecal baclofen pump) | MULTIDISCIPLINARY: Speech therapy, OT, Psychology, Dietitian, School support" Arrow down to OUTCOMES & MONITORING box (light blue): "• Most children with diplegia walk by age 4 • GMFCS level predicts ambulation & hip dislocation risk • Adults with CP outnumber children 3:1 • Regular orthopaedic & neurological surveillance lifelong" Use color-coded boxes, clean arrows, professional clinical style with legible fonts at least 11pt. Flowchart should be tall and well-organised, approximately A3 portrait orientation.
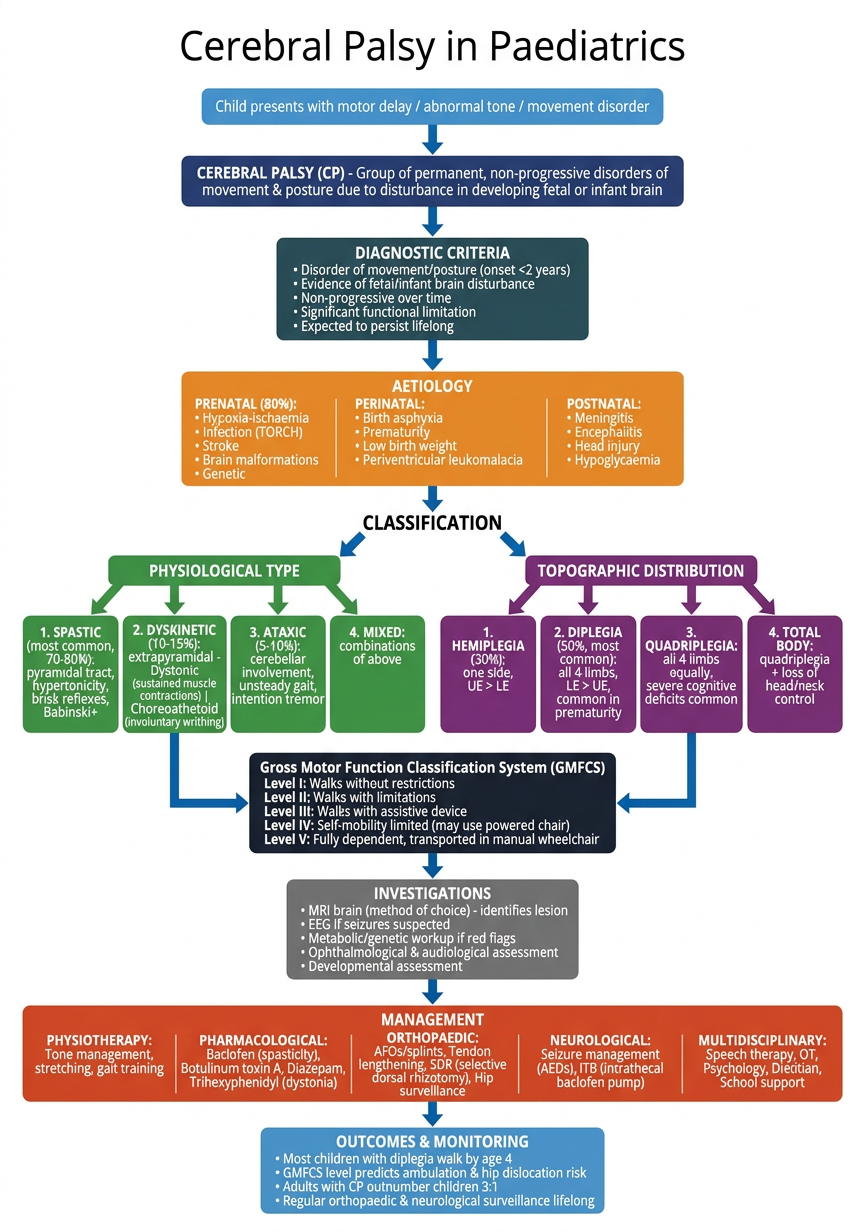
- Presentation - child with motor delay, abnormal tone, or movement disorder
- Definition - permanent, non-progressive disorders of movement/posture due to fetal/infant brain disturbance (Rosenbaum et al., 2007 consensus definition)
- Diagnostic Criteria - all 5 must be met (onset <2 yrs, non-progressive, functional limitation, expected lifelong, brain disturbance evidence)
- Aetiology - split into Prenatal (80%), Perinatal, and Postnatal causes
- Classification (dual pathway):
- Physiological type - Spastic (70-80%), Dyskinetic (dystonic/choreoathetoid), Ataxic, Mixed
- Topographic distribution - Hemiplegia (30%), Diplegia (50%), Quadriplegia, Total body
- GMFCS - Levels I-V grading motor function by age
- Investigations - MRI brain (gold standard), EEG, metabolic/genetic workup, developmental assessment
- Management - Physiotherapy, Pharmacological (Botox-A, Baclofen, ITB pump), Orthopaedic surgery, Neurological (AEDs), and full MDT
- Outcomes - monitoring, ambulation prognosis, lifespan care