Upper Motor neuron
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative neurology textbooks. Let me compile the full answer.
Upper Motor Neuron (UMN)
Definition
The Upper Motor Neuron (UMN) refers broadly to neurons originating in the motor cortex whose axons descend to synapse with Lower Motor Neurons (LMNs) in the brainstem nuclei and spinal cord anterior horn cells, which in turn innervate skeletal muscle.
Important distinction: The terms corticospinal, pyramidal, and upper motor neuron are NOT synonymous. The UMN system includes not only the corticospinal/pyramidal tract but also indirect descending pathways (rubrospinal, reticulospinal, vestibulospinal, tectospinal). - Adams and Victor's Principles of Neurology, 12th Ed.
Anatomy and Course
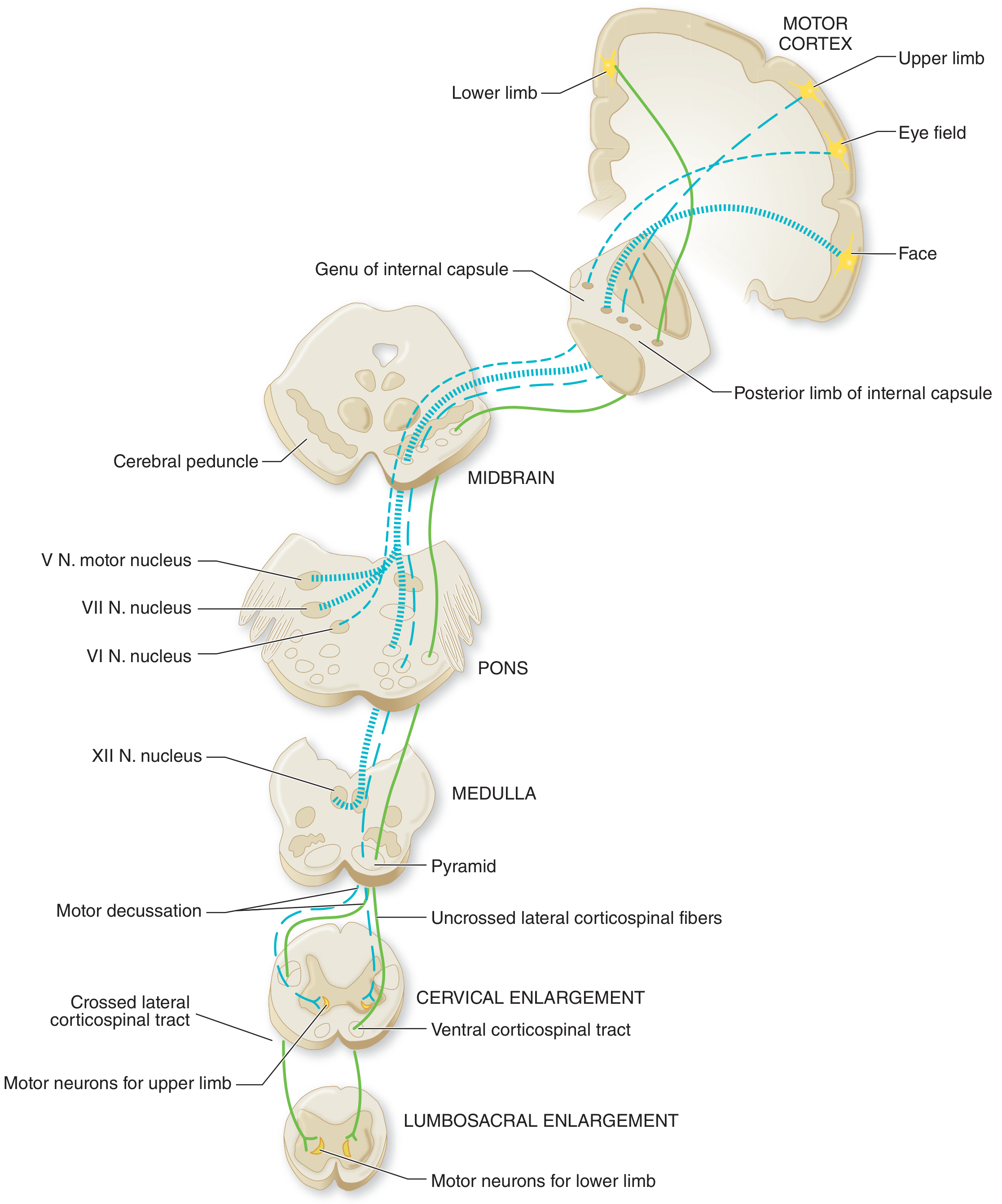
Figure: Corticospinal and corticobulbar tracts - from motor cortex origin to spinal cord termination
Corticospinal Tract (for limbs/trunk)
The tract descends through the following structures in order:
- Motor cortex (primary origin - Brodmann area 4, plus supplementary motor area 6, somatosensory areas 3/1/2, parietal areas 5/7)
- Subcortical white matter (corona radiata)
- Posterior limb of internal capsule
- Cerebral peduncle (midbrain)
- Basis pontis (ventral pons)
- Medullary pyramid (upper medulla)
- Motor decussation (lower medulla) - ~85-90% of fibers cross here
- Lateral funiculus of spinal cord (as the lateral corticospinal tract)
- Synapse on anterior horn LMNs
A small uncrossed component travels as the ventral corticospinal tract and crosses at segmental levels.
Corticobulbar Tract (for cranial nerve motor nuclei)
- Fibers peel off at each brainstem level to innervate cranial nerve motor nuclei (V, VII, IX, X, XI, XII)
- Most cranial motor nuclei receive bilateral UMN input (hence facial/jaw/pharyngeal muscles are relatively spared in unilateral UMN lesions)
- The lower face and tongue are predominantly contralaterally innervated - so UMN lesions cause contralateral lower facial weakness
Origin of Pyramidal Tract Fibers
- Only ~25,000-35,000 Betz cells exist, yet the medullary pyramid contains ~1 million axons
- Origins: ~40% from parietal cortex (areas 1, 3, 5, 7), ~30% from motor area 4, ~30% from premotor area 6
UMN Lesion Signs vs. LMN Lesion Signs
| Sign | UMN Lesion | LMN Lesion |
|---|---|---|
| Weakness | Yes | Yes |
| Atrophy | No (disuse atrophy may occur late) | Yes (prominent, early) |
| Fasciculations | No | Yes |
| Reflexes | Increased (hyperreflexia) | Decreased (hyporeflexia/areflexia) |
| Tone | Increased (spasticity) | Decreased (flaccidity) |
| Babinski sign | Present (positive/extensor) | Absent |
| Hoffmann sign | Present | Absent |
| Clonus | Present | Absent |
Source: Neuroanatomy through Clinical Cases, 3rd Ed.
Key Pattern of Weakness in UMN Lesions
- Affects groups of muscles (never single muscles)
- Proximal > distal involvement
- Upper limb extensors disproportionately affected (flexors relatively spared) - causes pronator drift, arm flexion posture
- Lower limb flexors disproportionately affected (extensors relatively spared) - causes leg extension/circumduction gait
- Bilateral movements (eyes, jaw, forehead, pharynx) are relatively spared due to bilateral innervation (Broadbent's law)
- Fine motor deficits (e.g., finger tapping) are prominent
Acute vs. Chronic UMN Lesions
A critical clinical point: acute UMN lesions do NOT immediately cause spasticity.
- Acute phase: Flaccid paralysis, decreased tone, decreased reflexes ("spinal shock" or "cerebral shock")
- Chronic phase: Gradual development of spasticity, hyperreflexia, and pathological reflexes over hours to months
The mechanism: spasticity results from damage to descending inhibitory pathways that travel alongside the corticospinal tract (not from corticospinal damage itself). Loss of these inhibitory influences leads to increased anterior horn motor neuron excitability.
Localization of UMN Lesions by Pattern
| Pattern | Likely Location |
|---|---|
| Restricted arm/leg weakness only | Cortex or subcortex (somatotopic lesion) |
| Hemiparesis (face + arm + leg) | Posterior limb of internal capsule or brainstem |
| Hemiparesis + cortical signs (aphasia, neglect, seizure) | Cerebral cortex |
| Ipsilateral CN signs + contralateral hemiparesis (crossed syndrome) | Brainstem |
| Hemiparesis without facial weakness | Cervical spinal cord (above C5) |
| Paraparesis | Thoracic spinal cord |
| Quadriparesis | Cervical spinal cord |
UMN Disorders (Clinical Examples)
- Stroke (most common) - hemiplegia/hemiparesis
- Spinal cord injury - para/quadriplegia
- Multiple sclerosis - demyelination of corticospinal tracts
- Amyotrophic Lateral Sclerosis (ALS) - combined UMN + LMN degeneration
- Primary Lateral Sclerosis - pure UMN syndrome
- Hereditary Spastic Paraplegia - genetic UMN degeneration
- Cerebral palsy - perinatal UMN injury
UMN vs. LMN: Clinical Memory Aid
| Feature | UMN ("Upper = Up-regulated") | LMN ("Lower = Less everything") |
|---|---|---|
| Reflexes | Up (hyperreflexia) | Down (hyporeflexia) |
| Tone | Up (spastic) | Down (flaccid) |
| Atrophy | Absent/late | Present/early |
| Babinski | Positive | Negative |
| Fasciculations | No | Yes |
Sources:
- Adams and Victor's Principles of Neurology, 12th Ed. - anatomic/physiologic basis of the UMN
- Neuroanatomy through Clinical Cases, 3rd Ed. - UMN vs LMN comparison table and clinical localization
- Frameworks for Internal Medicine - UMN definition, patterns of weakness, and lesion localization
This is a shared conversation. Sign in to Orris to start your own chat.