Generate a flowchart for examination of patient for heart murmurs
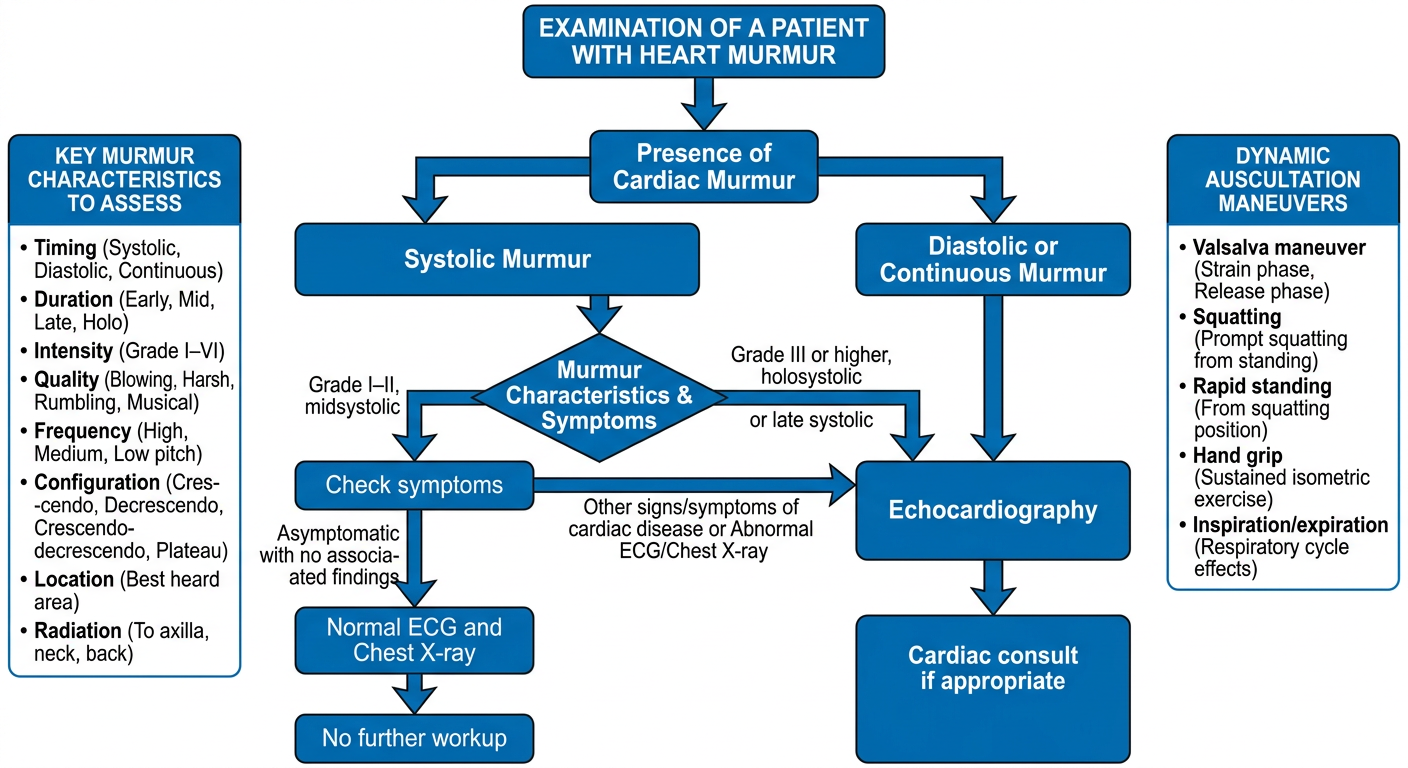
A detailed clinical flowchart titled "Examination of a Patient with Heart Murmur" showing the complete diagnostic approach. The flowchart starts at the top with "Presence of Cardiac Murmur" and branches into two main paths: Systolic Murmur (left) and Diastolic or Continuous Murmur (right). For Systolic Murmur, it further branches into: - Grade I–II, midsystolic → check symptoms → if Asymptomatic with no associated findings → Normal ECG and Chest X-ray → No further workup - Grade III or higher, holosystolic or late systolic → leads to Echocardiography If Other signs/symptoms of cardiac disease or Abnormal ECG/Chest X-ray → leads to Echocardiography → Cardiac consult if appropriate For Diastolic or Continuous Murmur: always leads directly to Echocardiography → Cardiac consult if appropriate Include a side box listing key murmur characteristics to assess: Timing, Duration, Intensity (Grade I–VI), Quality, Frequency, Configuration, Location, Radiation. Include another side box for Dynamic Auscultation maneuvers: Valsalva, Squatting, Rapid standing, Hand grip, Inspiration/expiration. Clean, professional medical flowchart style with blue and white color scheme, clear arrows, and labeled boxes.
Approach to Examination of a Patient with Heart Murmur
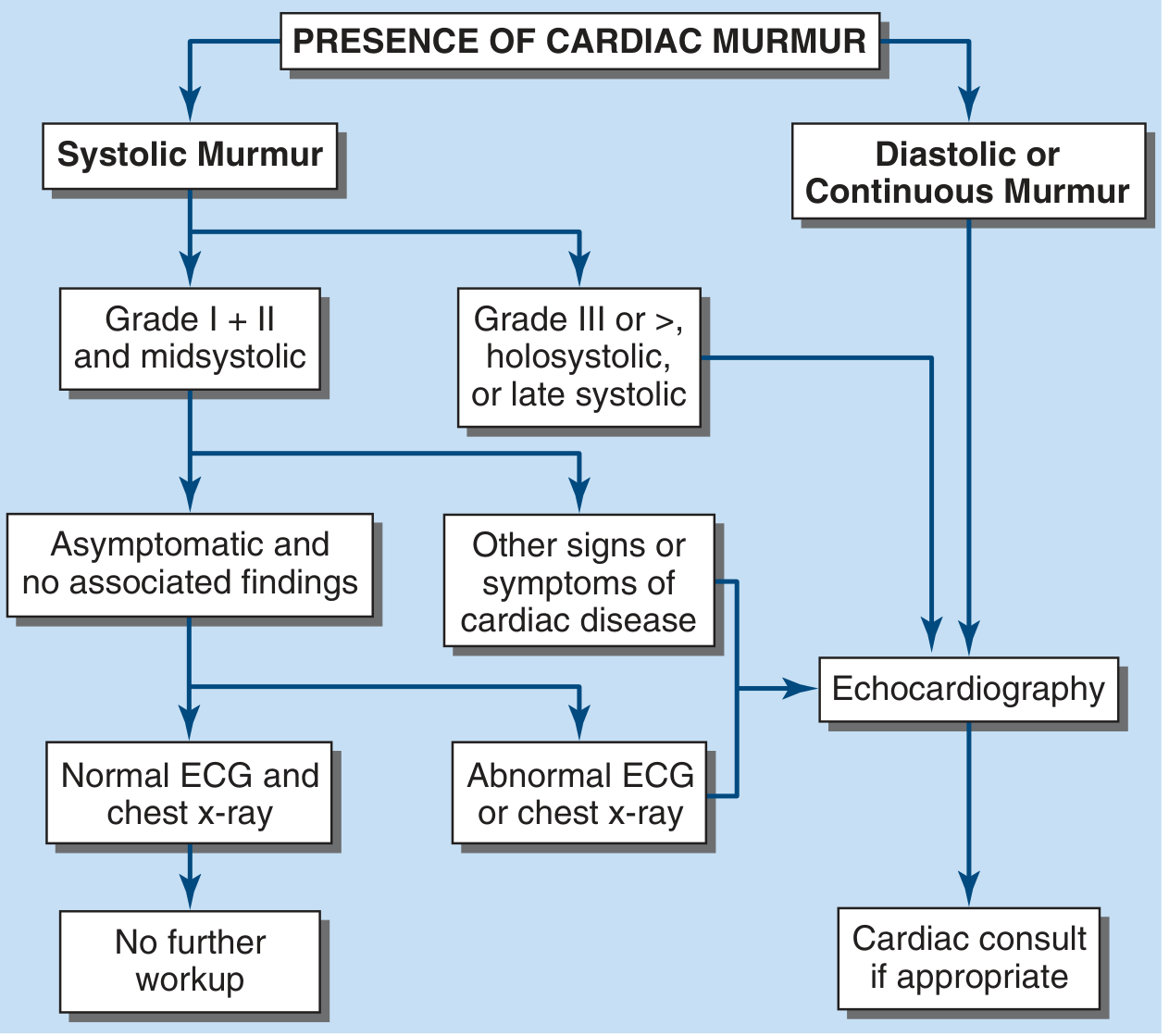
Official Diagnostic Flowchart (Harrison's Principles of Internal Medicine, 22nd Ed.)
Enhanced Clinical Flowchart
Key Clinical Framework
Step 1 — Characterize the Murmur
| Attribute | What to Assess |
|---|---|
| Timing | Systolic, diastolic, or continuous |
| Duration | Ejection (crescendo-decrescendo), holosystolic, early/mid/late |
| Intensity | Grade I–VI (Levine scale) |
| Quality | Harsh, blowing, rumbling, musical |
| Frequency | High, medium, low pitched |
| Location | Apex, LLSB, RUSB, LUSB |
| Radiation | Axilla (MR), carotids (AS), back (PR/AS) |
Step 2 — Systolic vs. Diastolic/Continuous
- Grade I–II, midsystolic in an asymptomatic child or young adult with no other cardiac findings → likely benign (innocent) → ECG + CXR; if normal, no further workup needed
- Grade ≥III, holosystolic, or late systolic → Echocardiography indicated
- Any systolic murmur with other signs/symptoms of cardiac disease (dyspnea, syncope, chest pain, thrills, abnormal S2) → Echocardiography
- Abnormal ECG or CXR → Echocardiography → Cardiology referral
- Always pathological — Echocardiography indicated in all cases → Cardiology consult
Step 3 — Dynamic Auscultation Maneuvers
| Maneuver | Effect | Interpretation |
|---|---|---|
| Inspiration | ↑ right-sided murmurs | Tricuspid/pulmonary lesions louder |
| Valsalva (strain) | ↓ most murmurs; ↑ MVP & HOCM | Identifies MVP, HOCM |
| Squatting | ↑ preload/afterload → MVP click moves later | HOCM murmur softer |
| Rapid standing | ↓ preload → MVP click moves earlier | HOCM murmur louder |
| Hand grip | ↑ LV afterload → ↑ MR, VSD, AR | Distinguishes MR from AS |
| Post-PVC beat | ↑ AS murmur, no change in MR | Gallavardin differentiation |
Step 4 — Grading (Levine Scale)
| Grade | Description |
|---|---|
| I | Barely audible, requires concentration |
| II | Soft but easily heard |
| III | Moderately loud, no thrill |
| IV | Loud + thrill present |
| V | Very loud, heard with stethoscope partially off chest |
| VI | Audible without stethoscope |
A murmur accompanied by a thrill = Grade IV or higher and is always pathological.