Neuroraphy what's it principles usage indication and problems and disadvantages complete details with appropriate illustrative diagrams and images
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Searching the Web
neurorrhaphy principles techniques indications complications 2024
I now have comprehensive textbook content, high-quality diagrams, and web sources. Let me compile the complete, well-illustrated answer.
Neurorrhaphy - Complete Guide with Diagrams
What is Neurorrhaphy?
Neurorrhaphy (from Greek: neuron = nerve + rhaphy = suture) is the surgical repair of a severed or damaged peripheral nerve by suturing its cut ends together, with the goal of re-establishing anatomical continuity and allowing axonal regeneration to proceed into the distal nerve stump.
1. Anatomical Foundation
Understanding nerve structure is essential to understanding neurorrhaphy.
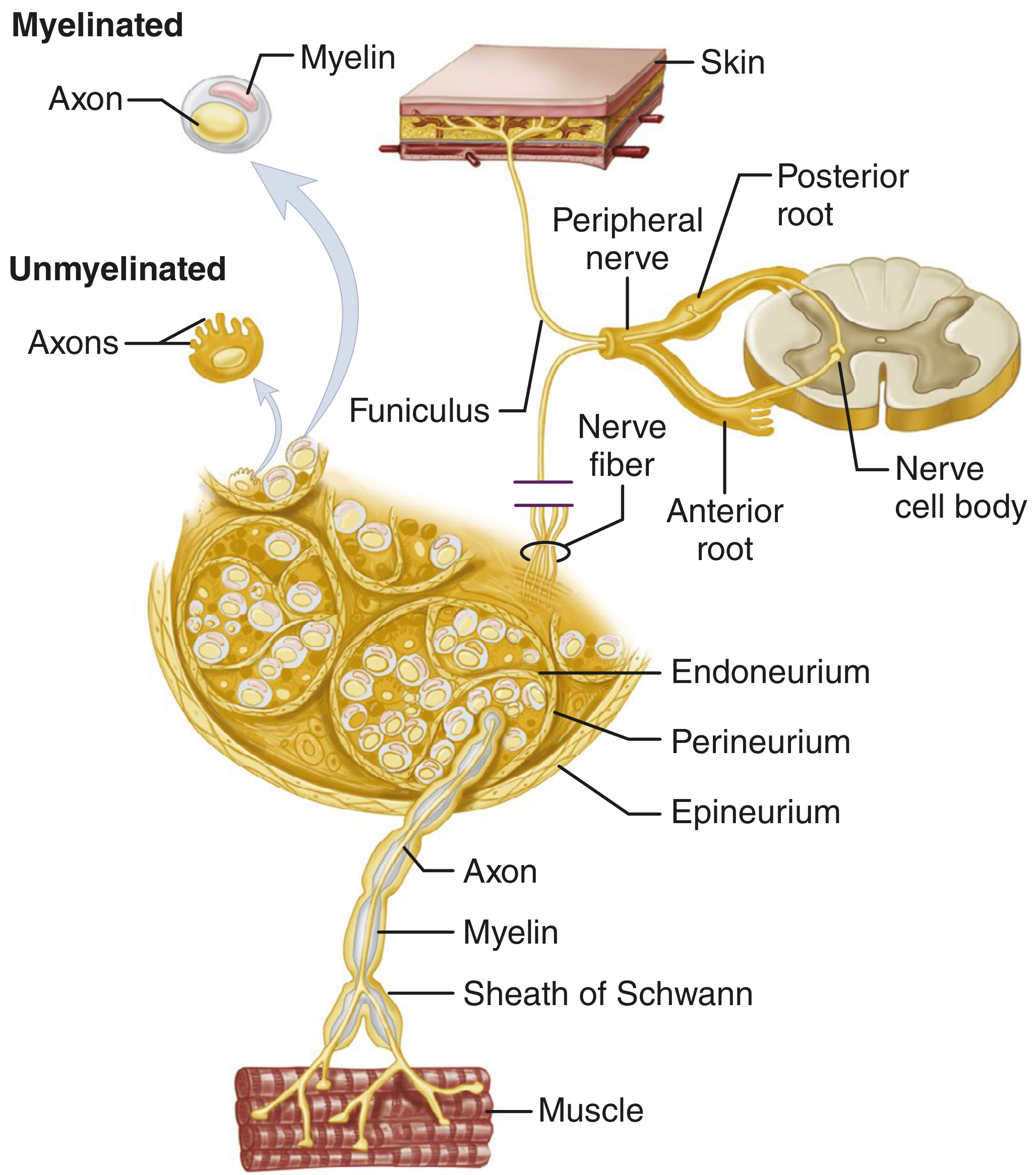
eFig 67.3 - Microscopic anatomy of peripheral nerve (Campbell's Operative Orthopaedics, 15th Ed)
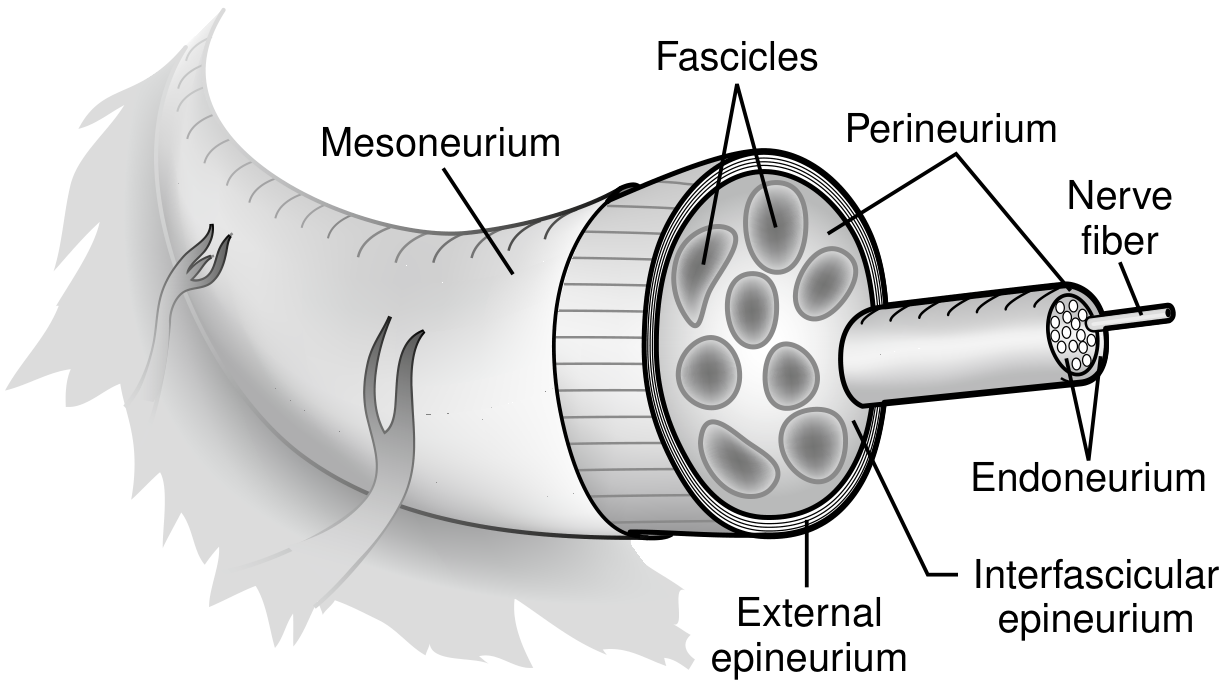
Fig 1 - Anatomy of a peripheral nerve (Current Surgical Therapy 14e)
Layers of the Peripheral Nerve (inner to outer):
| Layer | What it surrounds |
|---|---|
| Endoneurium | Individual axons (Schwann cell sheaths) |
| Perineurium | Each fascicle (a bundle of axons) |
| Interfascicular epineurium | Space between fascicles |
| External epineurium | The whole nerve trunk |
| Mesoneurium | Loose connective tissue carrying blood supply |
The mesoneurium provides the extrinsic vascular supply; the intrinsic longitudinal blood supply runs within the epi-, peri-, and endoneurium, allowing safe mobilization without complete devascularization.
2. Principles of Neurorrhaphy
Core Biological Principle - Nerve Regeneration
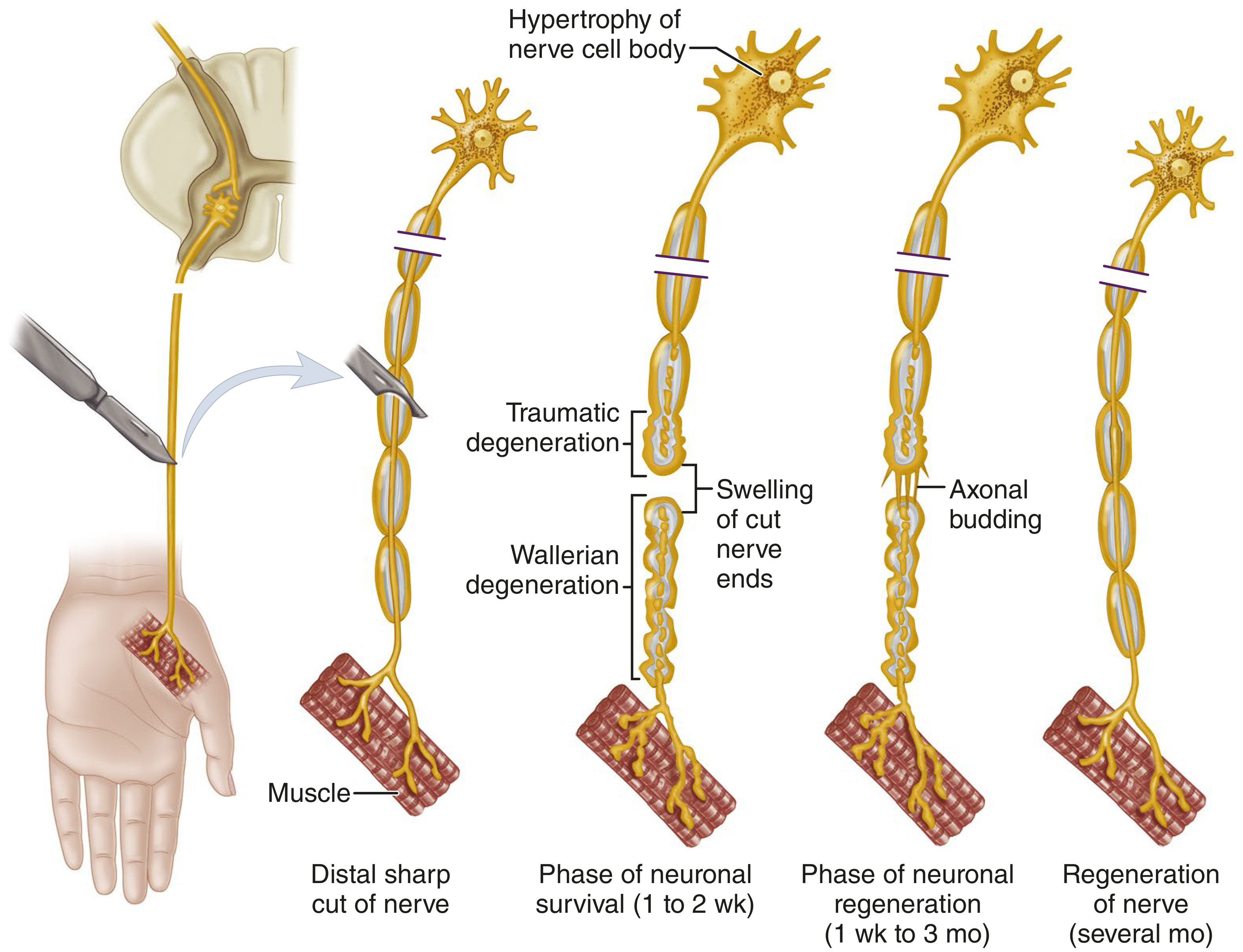
eFig 67.7 - Physiologic changes in regeneration of peripheral motor nerve axon after division (Campbell's Operative Orthopaedics)
When a nerve is divided:
- Wallerian (orthograde) degeneration proceeds distally from the cut - axon and myelin fragment, then are cleared by macrophages by days 15-30
- Retrograde degeneration occurs proximally back at least one internode; severe injury causes chromatolysis of the cell body
- Schwann cells divide (from day 7) and fill the endoneurial tubes, creating a scaffold
- Axonal sprouting begins within 24 hours from the proximal stump - multiple growth cones form
- Axons grow distally at approximately 1 mm/day (1 inch/month)
The goal of neurorrhaphy is to align the proximal and distal stumps with minimal gap and no tension, so regenerating axons can enter the correct endoneurial tubes in the distal stump.
Surgical Principles
- Tension-free repair - Excessive tension is the single most destructive force, causing intraneural fibrosis and blocking regeneration. If the gap cannot be closed with the main joint flexed 90°, nerve grafting is preferred.
- No rotation of nerve ends - Orientation sutures are placed in the epineurium before mobilization so ends are joined without axial rotation; longitudinal epineurial vessels can also guide alignment.
- Healthy nerve ends - Serial 1 mm cuts are made until normal fasciculi appear; all neuroma (proximal) and glioma (distal) must be excised.
- Meticulous technique - Operating microscope, small instruments (vessel loops, nerve miter box), non-reactive monofilament nylon suture (8-0, 9-0, or 10-0).
- Appropriate timing - Early repair shortens denervation time and fascicular alignment is better due to minimal excision required.
- Adequate exposure - Incisions must extend well proximal and distal; short incisions are the commonest cause of failed nerve surgery.
"In no type of surgery is the incision more important... Short incisions are probably the cause of more futile nerve operations than any other factor except surgeon inexperience."
- Campbell's Operative Orthopaedics, 15th Ed
3. Indications for Neurorrhaphy
Nerve exploration (and potentially neurorrhaphy) is indicated when:
- Sharp, clean laceration has obviously divided a nerve (knife, glass, razor) - primary repair within 6-8 hours, or delayed primary repair within 7-18 days
- Blunt/avulsion/blast wounds with unknown nerve status - for identification and end marking for later repair
- Blunt or closed trauma with nerve deficit and no clinical/electrophysiological evidence of regeneration after appropriate waiting period
- Penetrating wound (e.g., low-velocity gunshot) with persistent nerve deficit and no evidence of regeneration
Neurotmesis (Sunderland class V) - complete transection of all neural structures - always requires surgery. Sunderland class IV (perineurium disrupted, no spontaneous recovery) also requires surgical repair.
Injury Classification Relevant to Surgical Decision
| Seddon | Sunderland | Damage | Surgery? |
|---|---|---|---|
| Neurapraxia | I | Myelin only | No - spontaneous recovery |
| Axonotmesis | II | Axon + myelin | No - recovers spontaneously |
| Axonotmesis | III | + Endoneurium | Variable |
| Axonotmesis | IV | + Perineurium | Yes |
| Neurotmesis | V | All layers | Yes - always |
When to Delay Surgery
Delay is appropriate when:
- Progressive regeneration is evidenced by improving sensation, motor power, electrophysiology, or progression of the Tinel sign
- Wounds are contaminated, abraded, or crushed (delayed until soft-tissue equilibrium, usually 3-6 weeks)
- The extent of proximal/distal nerve damage cannot be delineated (wait for demarcation)
4. Techniques of Neurorrhaphy
Suture Material
Monofilament nylon (non-reactive, non-absorbable) has the widest application. Fibrin glue adjuncts ("nerve glues") reduce suture numbers and gapping tendency but do not increase repair strength and must not interpose between nerve ends.
Technique A: Epineurial Neurorrhaphy
The most widely used technique. Sutures are placed in the outer epineurium only.
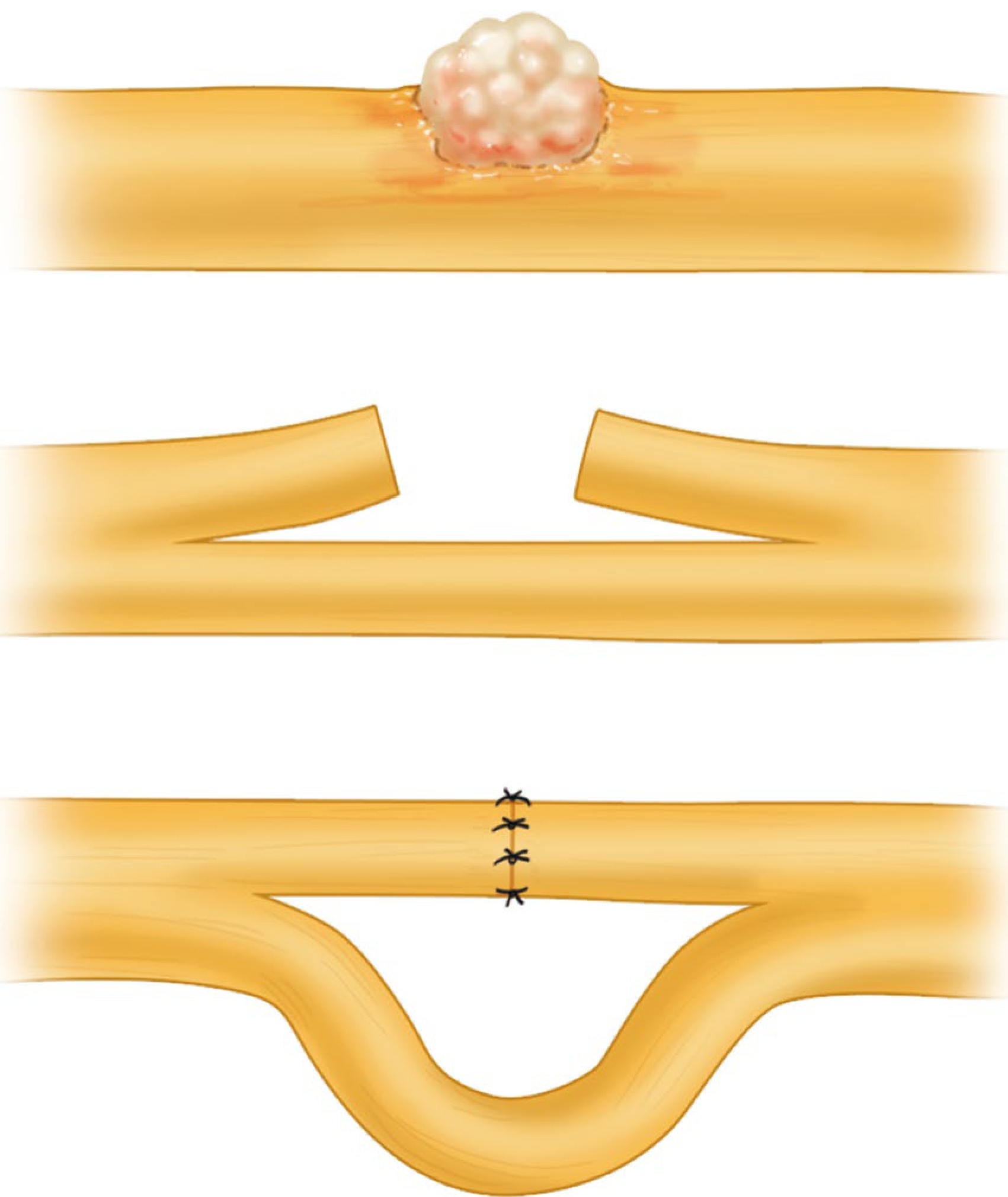
Fig 67.5 - Technique of partial neurorrhaphy (Campbell's Operative Orthopaedics 15th Ed)
Step-by-step (Technique 67.1):
- Expose nerve ends; confirm gap can be closed without tension
- Resect neuroma/glioma with sharp razor or diamond blade against a nerve miter box; make 1 mm serial cuts until normal fasciculi appear - use operating microscope; frozen sections if doubt remains
- Control bleeding with thrombin/gelatin sponge
- Place a traction (sling) suture of 7-0 or 8-0 nylon or steel needle fixation to stabilize nerve ends during repair
- Place an 8-0 nylon suture at the 12 o'clock position, leave long
- Place the corresponding 6 o'clock suture, leave long
- Using the long sutures as handles, assess rotation - align longitudinal epineurial vessels
- Place sutures at 3 and 9 o'clock
- Place additional interrupted 8-0 or 9-0 nylon sutures to produce satisfactory repair - confirm no kinking or fascicular deviation
- Before closure, remove sling sutures and assess positional tension through range of motion
Technique B: Perineurial (Fascicular) Neurorrhaphy
Sutures placed individually through the perineurium of matched fascicular groups.
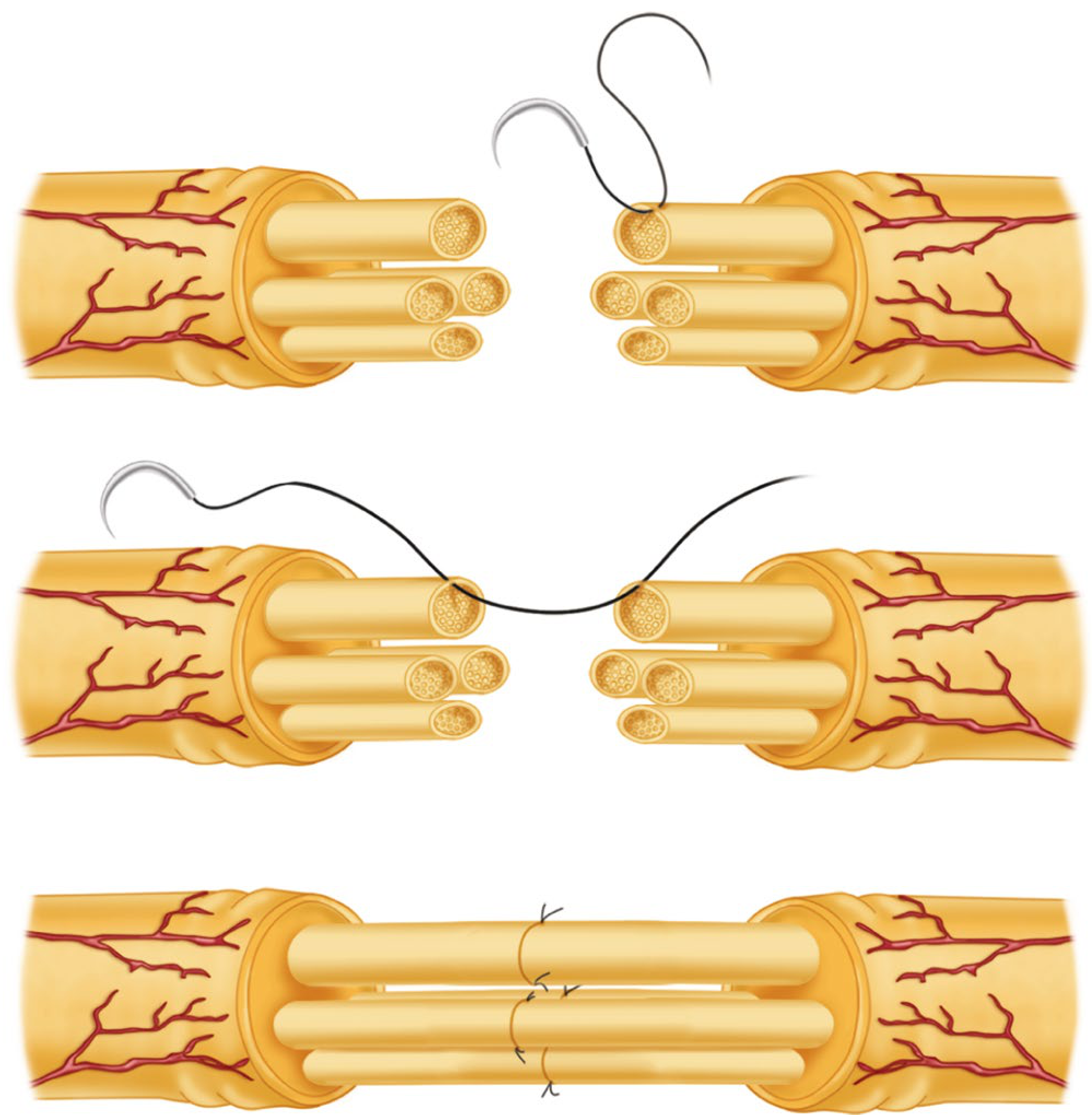
Fig 67.7 - Perineurial (fascicular) neurorrhaphy (Campbell's Operative Orthopaedics 15th Ed)
Step-by-step (Technique 67.2):
- Requires proficiency with operating microscope and 10-0 suture handling
- Resect ends as for epineurial repair
- Place nerve ends in proper rotation
- Under magnification, identify corresponding fascicular groups in proximal and distal stumps - diagram the arrangement on sterile paper
- Incise epineurium longitudinally proximally and distally; approximate fasciculi individually with interrupted 9-0 or 10-0 nylon
- Where multiple small fasciculi exist, group several together
- Close epineurium with interrupted nylon; or omit epineurial closure if repair is secure and tension-free (to reduce fibrosis)
Indications for fascicular repair (Sunderland's criteria):
- Fascicular groups are large enough to accept sutures
- Fascicular pattern predisposes to wasteful axon regeneration with epineurial repair alone
- Each fascicular group serves a specific identifiable branch - best seen in median and ulnar nerves at the wrist, and radial nerve just proximal to the elbow
Technique C: Partial Neurorrhaphy
Used when only part of the nerve is severed (common in large nerves - sciatic, brachial plexus trunks).
- Intact fascicles are dissected out and protected
- Injured portion is resected to normal tissue
- End-to-end repair of just the injured fascicles is performed
- Epiperineural or perineural sutures are used if epineurium is inadequate
Decision making: If motor response to stimulation is good, do not risk good motor fascicles just to restore sensation to a small area (e.g., dorsum of foot in peroneal, little finger in ulnar).
Technique D: Epiperineurial (Combined) Repair
The preferred approach at many centers: epiperineurial sutures at the periphery combined with perineurial fascicular sutures for large identifiable fascicular groups within the nerve.
5. Factors Influencing Outcome
A. Age of the Patient
- Children have the best results; elderly the worst
- Median nerve repair: two-point discrimination correlates with age - ~30 mm at 20-40 years; ~15 mm at 11-20 years; ~10 mm at <10 years
- Thought to relate to central nervous system plasticity and adaptation
B. Gap Between Nerve Ends / Mechanism of Injury
- Sharp lacerations (knife, razor): minimal proximal/distal damage, small gap, best prognosis
- High-velocity missile or road abrasion: extensive proximal/distal damage, large gap, worse prognosis
- Gap >2.5 cm historically associated with deteriorating results
- Closing the gap: nerve mobilization > nerve transposition > joint flexion > nerve grafts > bone shortening
C. Delay Between Injury and Repair
- 1% of recoverable nerve function is lost for each week of delay beyond 3 weeks (Omer)
- Motor recovery suffers most - significant loss of motor endplates and muscle fibrosis by 18 months
- Timing categories:
- Primary: within 6-8 hours (clean sharp wounds)
- Delayed primary: 7-18 days (still clean wound, better definition of injury extent)
- Secondary (delayed): 3-6 weeks+ (contaminated, crushed, blasted wounds)
D. Level of Injury
- More proximal injury = more incomplete recovery, especially in distal muscles
- Reasons: greater retrograde neuronal injury, higher proportion of cross-section occupied by proximal muscle fibers, greater chance of axonal disorientation during long regeneration path
E. Condition of the Nerve Ends
- Distal stump shrinks to 30-40% of normal fascicular cross-sectional area by ~4 months (due to Wallerian degeneration and Schwann cell/collagen changes)
- Intraneural plexus formation makes fascicular alignment progressively harder
- Scar, foreign material, or necrotic tissue impairs axonal regeneration
- A satisfactory external appearance does not guarantee optimal internal fascicular alignment - fascicular malalignment is common
6. Contraindications and When NOT to Repair
- Active infection or septic wound
- Progressive spontaneous regeneration (Tinel sign advancing, improving motor/sensory tests) - observe
- Neurapraxia or Sunderland class I-II injuries - no surgery needed
- Irreversible distal muscle fibrosis (>18-24 months denervation without repair) - nerve repair may not restore meaningful function
- Insufficient surgical expertise or equipment
7. Complications and Disadvantages
Biological Complications
| Problem | Mechanism |
|---|---|
| Excessive intraneural fibrosis | Repair under tension; foreign suture material; scar ingrowth at repair site |
| Fascicular malalignment | Even meticulous technique cannot guarantee motor axons reinnervate motor targets |
| Neuroma formation | Axonal sprouts that fail to enter endoneurial tubes form a disorganized neuroma |
| Painful dysesthesias / neuropathic pain | Aberrant regeneration, cross-innervation, or failure of axons to reach targets |
| Synkinesis | Motor axons reinnervating wrong muscles (especially problematic in facial nerve, proximal nerves) |
| Failed regeneration | Axons may not traverse the repair site at all, especially with tension or dense scar |
Technical Disadvantages
- Intraneural suture material - even 10-0 nylon causes local tissue reaction and scarring inside the nerve, potentially blocking axon growth
- Tension - even mild tension at the suture line causes ischemia and fibrotic scarring; the nerve ends experience 90° joint position during healing
- Rotation errors - even small axial rotational mismatch misdirects sensory and motor fibers to wrong targets
- Fascicular pattern mismatch - fascicular patterns change over the nerve's length; matched patterns seen after clean transection become more dissimilar with any gap (especially proximal nerves)
- Requirement for specialized equipment - operating microscope, microinstruments, trained microsurgeon; results are highly surgeon-dependent
- Recovery is slow and incomplete - regeneration at 1 mm/day means months to years before function returns; proximal injuries (e.g., brachial plexus) may never fully recover
- Denervated muscle atrophy - even with successful repair, muscle may be irreversibly fibrosed if reinnervation is delayed >18 months
- Second donor site morbidity (when grafting needed) - if gap is too large for direct repair and grafting is required, the donor nerve (commonly sural nerve) leaves sensory deficit
Specific Disadvantages of Each Technique
Epineurial repair:
- Does not guarantee fascicular alignment - relies on external landmarks
- Mismatch of motor/sensory fibers is common
Fascicular repair:
- Requires greater surgical skill and time
- More suture material inside the nerve = more fibrosis potential
- Cannot be done accurately in every case (Sunderland): fascicular patterns may not correspond, numbers of funiculi may not match, small fasciculi cannot take sutures without trauma
8. Summary Table
| Aspect | Key Points |
|---|---|
| Definition | Surgical suture repair of a divided peripheral nerve |
| Principle | Tension-free end-to-end apposition to guide axonal regeneration through endoneurial tubes |
| Best indication | Neurotmesis (Sunderland V); sharp clean laceration; primary or delayed primary setting |
| Main techniques | Epineurial, fascicular (perineurial), partial, combined epiperineurial |
| Suture material | Monofilament nylon 8-0 to 10-0; operating microscope mandatory |
| Golden rule | No tension - if gap >2.5 cm or cannot close with 90° joint flexion, use nerve graft |
| Rate of recovery | ~1 mm/day axon growth; months to years for clinical return |
| Best prognostic factors | Young age, distal injury, sharp mechanism, short delay, small gap |
| Worst prognostic factors | Elderly, proximal injury, blast/crush, long delay, large gap |
| Main complications | Fibrosis, malalignment, neuroma, neuropathic pain, synkinesis, failed regeneration |
Sources: Campbell's Operative Orthopaedics 15th Ed 2026; Current Surgical Therapy 14e; Cummings Otolaryngology - Head and Neck Surgery
This is a shared conversation. Sign in to Orris to start your own chat.