Heart anatomy and physiology
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Loading Image
I now have all the information needed for a comprehensive, well-illustrated response. Let me compile everything.
Heart Anatomy and Physiology
Sources: Guyton and Hall Textbook of Medical Physiology; Goldman-Cecil Medicine; Costanzo Physiology 7th Ed; Gray's Anatomy for Students; Barash Clinical Anesthesia 9th Ed
1. Gross Anatomy
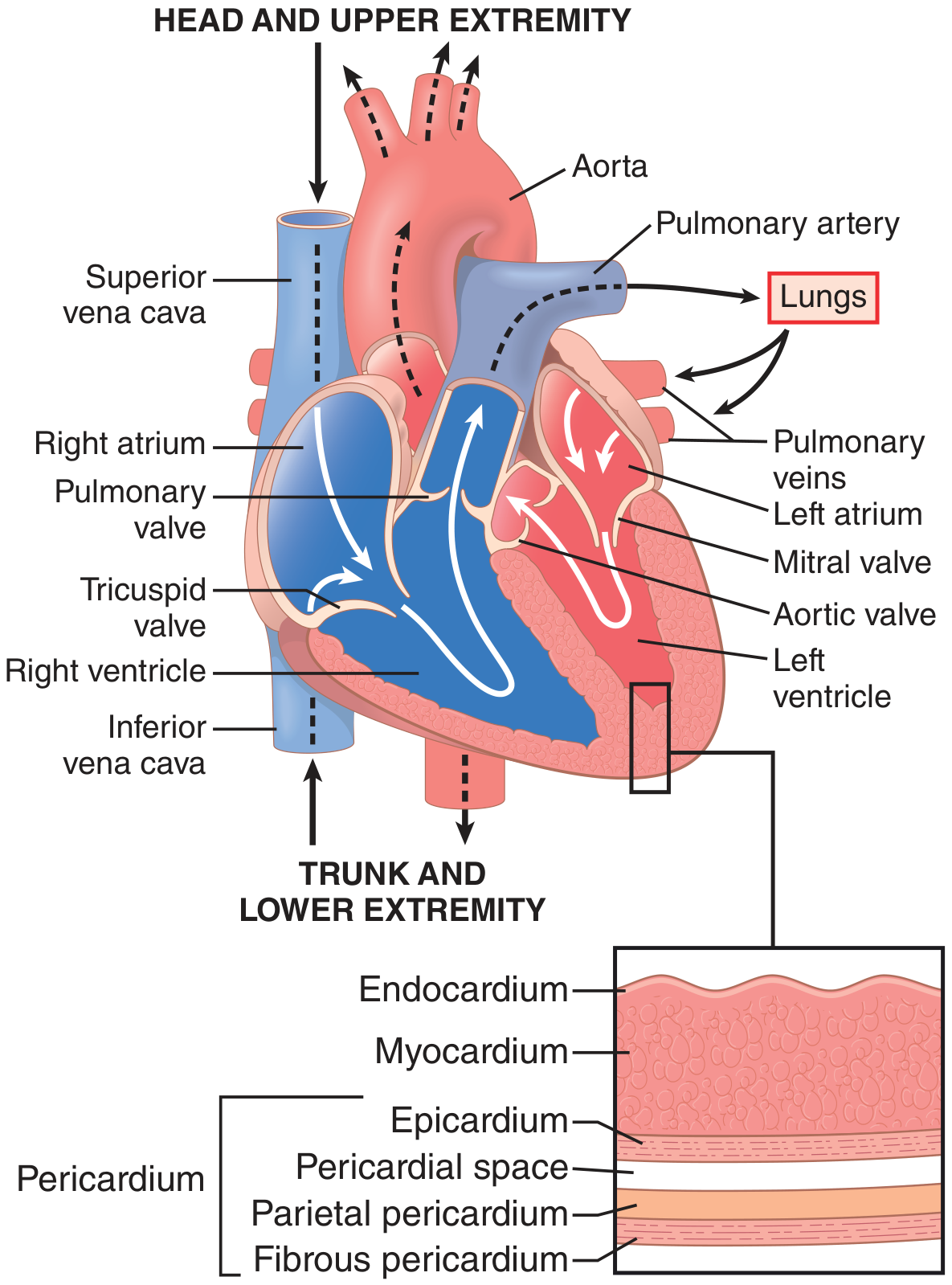
The heart is a four-chambered muscular pump enclosed within the pericardium, which has two layers - a fibrous outer layer and a serous inner layer (parietal and visceral/epicardium) with a pericardial space in between. The heart wall itself consists of three layers:
- Endocardium - inner smooth lining
- Myocardium - the contractile muscle bulk
- Epicardium - outer visceral pericardial layer
Chambers
| Chamber | Wall | Function |
|---|---|---|
| Right atrium | Thin | Receives deoxygenated blood from SVC, IVC, coronary sinus |
| Right ventricle | Thin | Pumps blood to lungs via pulmonary artery |
| Left atrium | Thin | Receives oxygenated blood from 4 pulmonary veins |
| Left ventricle | Thick | Pumps blood into systemic circulation via aorta |
The interventricular septum divides the two ventricles. The left ventricle is the primary pumping chamber, composed of billions of cardiomyocytes connected end-to-end through gap junctions. - Goldman-Cecil Medicine
The LV has a unique double-helix muscle fiber architecture: subepicardial fibers spiral leftward, subendocardial fibers spiral rightward. This creates a wringing/twisting (torsion) motion during systole, pulling the base toward the apex. At end-systole the ventricle is like a loaded spring and recoils during diastole to rapidly fill. - Guyton & Hall, p.122
Valves
| Valve | Location | Opens During |
|---|---|---|
| Tricuspid (3 leaflets) | Right AV junction | Ventricular diastole |
| Mitral/Bicuspid (2 leaflets) | Left AV junction | Ventricular diastole |
| Pulmonary (semilunar) | RV-pulmonary artery | Ventricular systole |
| Aortic (semilunar) | LV-aorta junction | Ventricular systole |
AV valves are tethered to papillary muscles via chordae tendineae, which prevent leaflet prolapse (regurgitation) during ventricular contraction. The pressure gradient between ventricles and atria opens and closes the AV valves.
2. Conduction System
The conduction system initiates and coordinates contraction in a precise unidirectional sequence. - Gray's Anatomy for Students
SA Node → Atrial muscle → AV Node → Bundle of His
→ Right & Left Bundle Branches → Purkinje Fibers → Ventricular myocardium
-
Sinoatrial (SA) node - the primary pacemaker, located at the junction of the superior vena cava and right atrium (crista terminalis). Discharges spontaneously at 60-100 bpm.
-
Atrioventricular (AV) node - near the opening of the coronary sinus, close to the septal cusp of the tricuspid valve. Introduces a delay (~0.12 s) allowing atrial contraction to complete before ventricular activation.
-
Bundle of His - direct continuation of the AV node, travels along the lower border of the membranous interventricular septum before splitting into right and left bundle branches.
-
Right and left bundle branches - travel down respective sides of the interventricular septum toward the apex.
-
Purkinje fibers - subendocardial plexus with the most functional contacts to working myocardium. Ensure rapid, near-simultaneous activation of ventricular muscle from apex to base.
The conduction pathway is insulated from surrounding myocardium by connective tissue to prevent premature activation. Coronary artery disease can disrupt the blood supply to these cells and cause dysrhythmias. - Gray's Anatomy for Students
3. Cardiac Action Potentials

Ventricular/Atrial action potential (phases 0-4):
- Phase 0 - rapid upstroke; fast Na+ channels open
- Phase 1 - early rapid repolarization; transient K+ outflow
- Phase 2 - plateau; slow L-type Ca2+ channels open (balanced by K+ outflow) - unique to cardiac muscle, prevents tetanic contraction
- Phase 3 - rapid repolarization; K+ channels open
- Phase 4 - resting potential (-85 to -90 mV)
SA node action potential - no fast Na+ channels; slow spontaneous diastolic depolarization (Phase 4 "funny current" via If channels + T-type Ca2+), followed by upstroke via L-type Ca2+ channels. Resting potential only around -55 to -65 mV.
The ventricular refractory period lasts 0.25-0.30 s (matching the plateau duration), preventing re-excitation and tetanus - physiologically essential so the heart can relax and fill between beats. - Guyton & Hall
4. Excitation-Contraction Coupling
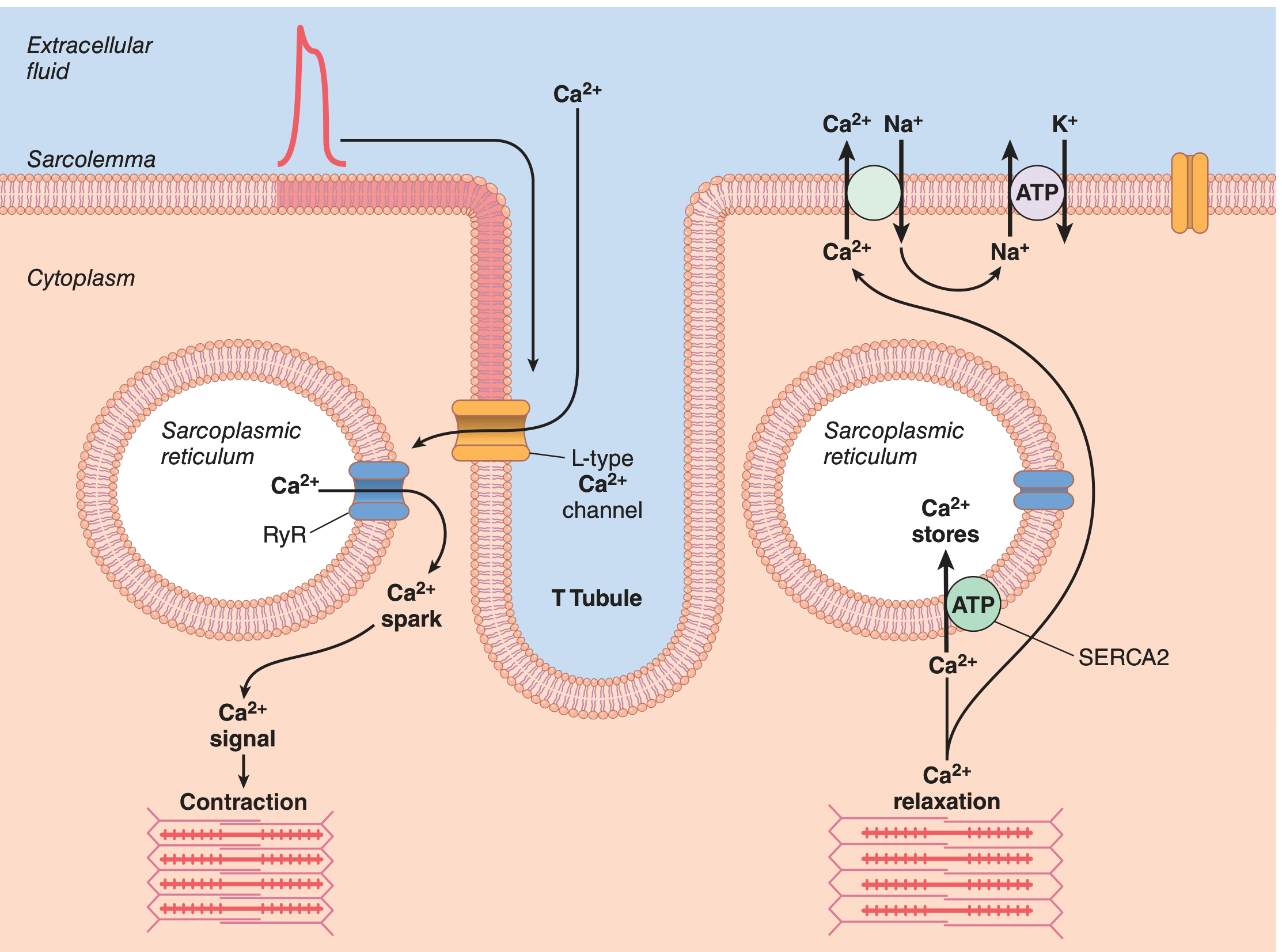
The key process linking electrical excitation to mechanical contraction:
- Action potential spreads into T tubules (5x wider in cardiac vs. skeletal muscle - hold large calcium stores)
- L-type Ca2+ channels (LTCC/dihydropyridine receptors) in T tubule membrane open - small Ca2+ influx
- This triggers ryanodine receptors (RyR2) in the sarcoplasmic reticulum (SR) to release a far larger Ca2+ store - "calcium-induced calcium release"
- Cytosolic Ca2+ rises, binds troponin C on thin filaments
- Troponin C-Ca2+ binding causes tropomyosin to shift, exposing myosin-binding sites on actin
- Cross-bridge cycling: myosin heads bind actin, ATPase activity causes power stroke (sliding filaments) → contraction
- Relaxation: Ca2+ pumped back into SR by SERCA2 (ATP-dependent), and out of cell via Na+/Ca2+ exchanger (NCX) and Ca2+-ATPase
Cardiac muscle depends on Ca2+ influx from T tubules as well as SR stores - unlike skeletal muscle which relies almost entirely on SR. This makes cardiac contractility responsive to extracellular Ca2+ and drugs like digoxin. - Guyton & Hall, p.125
5. The Cardiac Cycle
The cardiac cycle consists of 7 phases (as defined in Costanzo Physiology):
| Phase | Event | Valves | Heart Sound |
|---|---|---|---|
| A - Atrial systole | Atria contract; final ventricular filling; P wave | Mitral/tricuspid open | S4 (if present) |
| B - Isovolumetric ventricular contraction | Ventricles contract; pressure rises; all valves closed; volume constant | Mitral closes | S1 |
| C - Rapid ventricular ejection | Peak pressure; blood ejected; ventricular volume falls | Aortic opens | - |
| D - Reduced ventricular ejection | Slower ejection; min. ventricular volume; aortic pressure starts to fall | - | - |
| E - Isovolumetric ventricular relaxation | Ventricles relax; pressure falls; all valves closed; volume constant | Aortic closes | S2 |
| F - Rapid ventricular filling | Passive filling from atria; ventricular volume rises | Mitral opens | S3 (if present) |
| G - Reduced ventricular filling (diastasis) | Slow filling phase; near-equalization of atrial/ventricular pressures | - | - |
Key pressures (left heart, normal):
- LV systolic pressure: ~120 mmHg
- LV diastolic pressure: ~0-12 mmHg
- Aortic pressure: ~120/80 mmHg
Heart sounds: S1 = mitral valve closure (start of systole); S2 = aortic valve closure (start of diastole). S3 is heard in rapid filling (normal in children; pathological in adults = heart failure). S4 is heard with atrial contraction against a stiff ventricle (hypertension, hypertrophy).
6. Determinants of Cardiac Performance
Cardiac output (CO) = Heart rate (HR) × Stroke volume (SV). Normal CO at rest = ~5 L/min.
Stroke volume is determined by three factors:
Preload (end-diastolic volume / venous return)
The Frank-Starling Law: as end-diastolic volume (EDV) increases, stretch of myocardial fibers increases, leading to greater force of contraction and a larger stroke volume. This ensures the heart ejects whatever volume is returned to it. - Costanzo Physiology, p.155
Afterload (aortic pressure / peripheral vascular resistance)
The resistance against which the ventricle must pump. Increased afterload (e.g., hypertension, aortic stenosis) reduces stroke volume for a given preload.
Contractility (inotropy)
The intrinsic force-generating capacity of the myocardium independent of preload and afterload:
- Positive inotropes (digoxin, catecholamines, Ca2+): shift the Frank-Starling curve upward - greater SV at any given EDV; increased ejection fraction
- Negative inotropes (beta-blockers, Ca2+ channel blockers, heart failure): shift curve downward
7. Coronary Blood Flow
The coronary arteries arise from the aorta just above the aortic valve. Key points:
- Left coronary artery (LCA): divides into left anterior descending (LAD - supplies anterior LV, septum) and left circumflex (supplies lateral LV)
- Right coronary artery (RCA): supplies right ventricle, inferior LV, SA node, AV node in most individuals
Blood flow pattern:
- Subepicardial flow: during both systole and diastole
- Subendocardial flow: predominantly during diastole (compressed by intramyocardial pressure during systole)
The LV extracts ~70-80% of O2 from coronary blood under basal conditions (near maximal extraction). Therefore, increases in O2 demand (exercise, increased HR, hypertrophy) can only be met by increasing coronary blood flow - not by increased extraction. Key vasodilators that increase flow (up to 6-fold): nitric oxide, adenosine, bradykinin, prostaglandins, CO2. - Goldman-Cecil Medicine; Barash Clinical Anesthesia
Summary Table: Key Numbers
| Parameter | Normal Value |
|---|---|
| Heart rate | 60-100 bpm |
| Stroke volume | ~70 mL |
| Cardiac output | ~5 L/min |
| Ejection fraction | 55-70% |
| LV systolic pressure | ~120 mmHg |
| LV diastolic pressure | 0-12 mmHg |
| Ventricular refractory period | 0.25-0.30 s |
| Atrial refractory period | ~0.15 s |
| Coronary flow reserve (max increase) | ~6-fold |
Nursing diagnosis on jaundice
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Searching the Web
NANDA nursing diagnosis jaundice hyperbilirubinemia nursing care plan 2024
Reading Web Page
https://www.nurse.com/clinical-guides/jaundice-in-adults
Reading File
I have comprehensive content from authoritative clinical textbooks and nursing resources. Let me now compile the full, detailed nursing diagnosis response.
Nursing Diagnosis: Jaundice (Hyperbilirubinemia)
Sources: Schwartz's Principles of Surgery 11th Ed; Goldman-Cecil Medicine; Sleisenger & Fordtran's GI and Liver Disease; Nurse.com Adult Jaundice Clinical Guide; NANDA-I Framework
Pathophysiology Overview
Jaundice is the yellowish staining of the skin, sclera, and mucous membranes with the pigment bilirubin. It becomes clinically detectable when serum bilirubin rises above 2.5-3 mg/dL (normal: 0.3-1.0 mg/dL). Jaundice is a symptom, not a disease - it signals disruption somewhere in bilirubin metabolism. - Schwartz's Surgery
Bilirubin metabolism - three phases:
| Phase | Location | Process | Dysfunction Causes |
|---|---|---|---|
| Pre-hepatic | Bloodstream | RBC breakdown → unconjugated bilirubin → binds albumin → liver | Hemolytic anemia, G6PD deficiency, blood transfusion reactions |
| Intrahepatic | Liver cell | Conjugation with glucuronic acid (glucuronyltransferase) | Hepatitis, cirrhosis, Gilbert's syndrome, Crigler-Najjar, drug toxicity |
| Post-hepatic | Biliary tree | Conjugated bilirubin excreted into bile → duodenum | Cholelithiasis, cholangitis, pancreatic cancer, bile duct stricture |
Nursing Assessment
Subjective Data (History)
- Onset and duration of yellow discoloration
- Color of urine (dark/tea-colored = conjugated bilirubin spilling into urine)
- Color of stool (pale/clay-colored = obstructive jaundice)
- Pruritus (itching) - from bile salt deposition in skin
- Fatigue, malaise, anorexia, nausea
- Abdominal pain (RUQ pain suggests biliary/hepatic cause)
- Fever, chills (suggest cholangitis - a surgical emergency)
- Alcohol use, drug history, recent blood transfusions, travel history
- Family history (Gilbert's syndrome affects 4-7% of population)
Objective Data (Physical Examination)
- Skin and sclerae: yellow discoloration (scleral icterus is often the first visible sign)
- Skin integrity: scratch marks, excoriations from pruritus
- Abdomen: hepatomegaly, splenomegaly, tenderness, Murphy's sign (cholecystitis), palpable gallbladder (Courvoisier's sign in malignant obstruction)
- Neurological: confusion, asterixis (hepatic encephalopathy in advanced liver disease)
- Vital signs: fever (infection/cholangitis), hypotension (sepsis)
- Nutritional status: muscle wasting, cachexia, ascites
Laboratory Investigations (to guide diagnosis and monitor)
| Test | Pre-hepatic | Hepatic | Post-hepatic |
|---|---|---|---|
| Total bilirubin | Elevated | Elevated | Elevated |
| Direct (conjugated) bilirubin | Normal/slight rise | Elevated | Markedly elevated |
| Indirect (unconjugated) | Markedly elevated | Elevated | Normal |
| ALT/AST | Normal | Markedly elevated | Mildly elevated |
| ALP/GGT | Normal | Mildly elevated | Markedly elevated |
| Urine bilirubin | Absent | Present | Present |
| Urine urobilinogen | Increased | Decreased | Absent |
NANDA-I Nursing Diagnoses
The following are the primary nursing diagnoses applicable to a patient with jaundice, organized by priority:
1. Impaired Liver Function / Impaired Metabolic Function
Related to: hepatocellular damage, biliary obstruction, hemolytic processes
As evidenced by: elevated serum bilirubin, jaundiced skin and sclerae, abnormal liver function tests, dark urine, pale stools
Nursing Interventions:
- Monitor serum bilirubin (total, direct, indirect), LFTs, PT/INR, albumin daily or per orders
- Assess and document degree of jaundice (skin, sclera, mucous membranes) at each shift
- Monitor urine color and output; test urine for bilirubin and urobilinogen
- Observe stool color (pale/acholic = biliary obstruction)
- Administer prescribed medications (ursodeoxycholic acid, corticosteroids, antivirals) as ordered
- Avoid hepatotoxic drugs (acetaminophen in excess, NSAIDs, certain antibiotics) and report any new medications to the medical team
- Prepare patient for procedures (ERCP, biliary stenting, cholecystectomy) if indicated
Expected Outcomes:
- Serum bilirubin trending toward normal range
- Patient verbalizes understanding of underlying cause and treatment plan
2. Impaired Skin Integrity / Risk for Impaired Skin Integrity
Related to: bile salt deposition in skin causing pruritus and scratching
As evidenced by: complaints of itching, excoriation marks, dry skin, jaundiced appearance
Nursing Interventions:
- Assess skin condition every shift; document any abrasions, excoriations, or breaks
- Keep fingernails short and clean to minimize skin damage from scratching
- Apply cool, damp cloths or cool compresses to pruritic areas for relief
- Use mild, pH-balanced soaps; pat skin dry (do not rub)
- Apply emollients/moisturizers regularly; avoid alcohol-based lotions
- Maintain cool, low-humidity room environment (reduces pruritus intensity)
- Administer antipruritic medications as prescribed:
- H1 antihistamines (diphenhydramine, hydroxyzine)
- Bile acid resins (cholestyramine) - bind bile salts in gut
- Opioid antagonists (naltrexone) - for refractory pruritus
- Rifampicin (second-line; monitor for hepatotoxicity)
- Dress patient in soft, loose-fitting, non-irritating cotton clothing
- Educate patient to avoid scratching; suggest gentle patting instead
Expected Outcomes:
- Patient reports reduced severity of pruritus (numeric scale)
- No new skin breakdown or infection
3. Imbalanced Nutrition: Less Than Body Requirements
Related to: anorexia, nausea, impaired bile secretion affecting fat digestion, hepatic dysfunction affecting nutrient metabolism
As evidenced by: decreased oral intake, weight loss, muscle wasting, hypoalbuminemia, fatigue
Nursing Interventions:
- Assess nutritional status: weight, BMI, albumin, pre-albumin, dietary intake
- Provide small, frequent meals rather than large meals
- Offer high-carbohydrate, moderate-protein, low-fat diet (in obstructive jaundice where fat digestion is impaired due to lack of bile)
- Administer fat-soluble vitamin supplements (A, D, E, K) as prescribed - especially in obstructive jaundice where bile is absent from gut
- Monitor for signs of Vitamin K deficiency (prolonged PT/INR, easy bruising, bleeding)
- Administer IV Vitamin K or FFP if coagulopathy is present
- Consult dietitian for individualized nutritional support
- Encourage oral fluid intake; monitor for dehydration
- Administer antiemetics before meals if nausea is present
- Provide oral care before meals to improve appetite
Expected Outcomes:
- Patient maintains or regains stable weight
- Adequate caloric and protein intake documented
- Vitamin K-dependent coagulation factors normalize
4. Acute/Chronic Pain
Related to: biliary colic, hepatic capsule distension, inflammation, obstructive pathology
As evidenced by: patient reports of RUQ or epigastric pain, guarding, restlessness, facial grimacing
Nursing Interventions:
- Assess pain location, quality, severity (0-10 scale), radiation, onset, and aggravating/relieving factors
- Administer analgesics as prescribed; evaluate and document effectiveness
- Position patient for comfort (semi-Fowler's or side-lying may reduce pain)
- Apply warmth to abdomen (if not contraindicated) for biliary colic
- Note: Pain with fever, rigors, and jaundice = Charcot's triad (cholangitis) - escalate immediately
- Monitor for peritoneal signs (rigid abdomen, rebound tenderness) suggesting perforation
Expected Outcomes:
- Patient reports pain controlled at acceptable level
- Patient demonstrates non-pharmacologic pain management strategies
5. Risk for Deficient Fluid Volume
Related to: nausea and vomiting reducing oral intake, fever (in cholangitis/hepatitis), ascites, decreased albumin and oncotic pressure
As evidenced by: decreased urine output, dry mucous membranes, elevated BUN/creatinine
Nursing Interventions:
- Monitor intake and output strictly (including ascites drainage if applicable)
- Monitor vital signs for signs of dehydration or hypovolemia (tachycardia, hypotension)
- Assess skin turgor, mucous membrane moisture, daily weight
- Administer IV fluids as ordered
- Monitor electrolytes (Na+, K+, Mg2+) - cirrhotic patients prone to hyponatremia, hypokalemia
- Administer diuretics (spironolactone, furosemide) for ascites if prescribed; monitor response
Expected Outcomes:
- Balanced fluid intake and output
- Stable hemodynamic parameters
6. Risk for Disturbed Thought Processes (Hepatic Encephalopathy)
Related to: accumulation of ammonia and other toxins from impaired hepatic detoxification
As evidenced by (early signs): subtle personality changes, forgetfulness, sleep disturbances, asterixis (hand flapping tremor)
Nursing Interventions:
- Assess neurological status and orientation at each shift using a structured scale (West Haven criteria)
- Test for asterixis (ask patient to dorsiflex wrists with arms outstretched)
- Monitor serum ammonia levels
- Administer lactulose as prescribed (goal: 2-3 soft stools/day to reduce ammonia absorption)
- Administer rifaximin if prescribed (non-absorbed antibiotic reducing gut bacteria ammonia production)
- Restrict dietary protein only if encephalopathy is present (not routine - patients need adequate nutrition)
- Maintain safety: bed rails up, call light within reach, fall prevention measures
- Minimize sedating medications; avoid benzodiazepines if possible (worsen encephalopathy)
- Orient patient frequently; involve family in monitoring changes
Expected Outcomes:
- Patient remains oriented to person, place, time
- No asterixis; stable serum ammonia
7. Deficient Knowledge
Related to: new diagnosis, unfamiliarity with disease process, treatment plan, lifestyle modifications
As evidenced by: patient/family asking questions, non-compliance, incorrect statements about condition
Nursing Interventions:
- Assess current level of knowledge and learning readiness
- Teach about the cause of jaundice and expected course of illness
- Explain all diagnostic tests and procedures in plain language
- Instruct on dietary modifications (low-fat diet, avoid alcohol, adequate hydration)
- Educate about medications: purpose, dose, side effects, adherence
- Warn against hepatotoxic substances: alcohol, herbal supplements, excess paracetamol
- Teach warning signs requiring immediate medical attention: sudden worsening of jaundice, high fever with rigors (cholangitis), confusion, black tarry stools (GI bleeding), severe abdominal pain
- Provide written discharge instructions; reinforce with verbal teaching
- Arrange follow-up appointments and explain the importance of repeat labs
Expected Outcomes:
- Patient correctly states the cause and treatment plan
- Patient identifies warning signs that require emergency care
- Patient demonstrates medication compliance
8. Anxiety / Fear
Related to: uncertainty about diagnosis (especially if malignancy suspected), invasive procedures, prognosis
As evidenced by: expressed worry, tearfulness, sleep disturbance, restlessness
Nursing Interventions:
- Establish therapeutic relationship; use active listening techniques
- Provide clear, honest information about diagnosis and what to expect
- Allow patient and family to express fears and concerns
- Facilitate access to chaplain, social worker, or psychologist if appropriate
- Involve patient in care planning to restore sense of control
- Explain all procedures before performing them
Expected Outcomes:
- Patient reports reduced anxiety
- Patient demonstrates coping strategies
Summary: Priority Nursing Diagnoses at a Glance
| Priority | NANDA Diagnosis | Key Focus |
|---|---|---|
| 1 | Impaired Liver/Metabolic Function | Monitor LFTs, bilirubin, trigger investigation |
| 2 | Impaired Skin Integrity | Pruritus management, skin care |
| 3 | Imbalanced Nutrition: Less Than Body Requirements | Diet, fat-soluble vitamins, antiemetics |
| 4 | Acute/Chronic Pain | RUQ pain, biliary colic, Charcot's triad alert |
| 5 | Risk for Deficient Fluid Volume | Fluid balance, electrolytes |
| 6 | Risk for Disturbed Thought Processes | Encephalopathy, lactulose, safety |
| 7 | Deficient Knowledge | Education on disease, medications, warning signs |
| 8 | Anxiety / Fear | Psychosocial support |
Special Considerations
Neonatal jaundice (physiological vs. pathological): Requires monitoring of transcutaneous bilirubin, phototherapy management, feeding support, and parental education. Risk for kernicterus (bilirubin encephalopathy) in neonates if untreated.
Obstructive jaundice: High risk for cholangitis (Charcot's triad: fever + RUQ pain + jaundice; Reynold's pentad adds hypotension + confusion) - this is a surgical/endoscopic emergency requiring urgent ERCP or decompression.
Cirrhotic jaundice: Associated with decompensation (median survival ~1.6 years once jaundice appears) - requires comprehensive symptom management and goals-of-care discussions. - Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.