AKI basic to advanced
Reading File
Finding Sources
Finding Sources
Searching PubMed
"acute kidney injury"[MeSH Terms] AND management
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the complete AKI guide.
Acute Kidney Injury (AKI) - Basic to Advanced
1. Definition & Epidemiology
AKI is defined as a rapid decline in kidney function occurring within 1 week of an injury, manifesting as an abrupt reduction in GFR with accumulation of nitrogenous waste products and loss of fluid/electrolyte homeostasis.
KDIGO 2012 definition (the current standard) - AKI is present when ANY of the following occurs:
- Serum creatinine (sCr) rises ≥0.3 mg/dL within 48 hours
- sCr rises to ≥1.5x baseline within 7 days
- Urine output (UO) <0.5 mL/kg/h for >6 hours
Epidemiology:
- Affects ~10-15% of all hospitalized patients
- Rises to 55-65% of ICU patients
- Community-acquired AKI is uncommon: <1% annual incidence
- AKI requiring dialysis has increased substantially over the past three decades
- AKI is also frequently undiagnosed in low-resource settings worldwide
(Goldman-Cecil Medicine, p. 1243; Comprehensive Clinical Nephrology, p. 984)
2. Diagnostic Criteria & Staging
Three overlapping classification systems exist. KDIGO is now the standard:
RIFLE / AKIN / KDIGO Comparison
| Parameter | RIFLE | AKIN | KDIGO |
|---|---|---|---|
| sCr definition | >50% rise over <7 days | >0.3 mg/dL OR >50% over <48 h | >0.3 mg/dL over <48 h OR >50% over <7 days |
| UO definition | <0.5 mL/kg/h >6 h | Same | Same |
KDIGO Staging
| Stage | Serum Creatinine | Urine Output |
|---|---|---|
| 1 | 1.5-1.9x baseline OR ≥0.3 mg/dL increase | <0.5 mL/kg/h for 6-12 h |
| 2 | 2.0-2.9x baseline | <0.5 mL/kg/h for ≥12 h |
| 3 | ≥3.0x baseline OR ≥4.0 mg/dL OR initiation of KRT | <0.3 mL/kg/h for ≥24 h OR anuria ≥12 h |
In children <18 years, Stage 3 also includes eGFR <35 mL/min/1.73 m²
RIFLE outcome classes - "Loss" (need for RRT >4 weeks) and "End-stage" (RRT >3 months) - are not staging criteria but outcomes.
Key limitation: sCr is an insensitive marker because its rise is time-dependent. A patient can progress from Stage 1 to Stage 3 as creatinine continues to rise even with a fixed injury. The true GFR correlates poorly with AKI stage.
Acute Kidney Disease (AKD): The KDIGO working group also defined AKD as kidney disease with duration <3 months that doesn't meet AKI criteria but shows reduced GFR <60 mL/min or a >35% decline - bridging AKI and CKD.
(Brenner and Rector's The Kidney, p. 1245; Comprehensive Clinical Nephrology, p. 984)
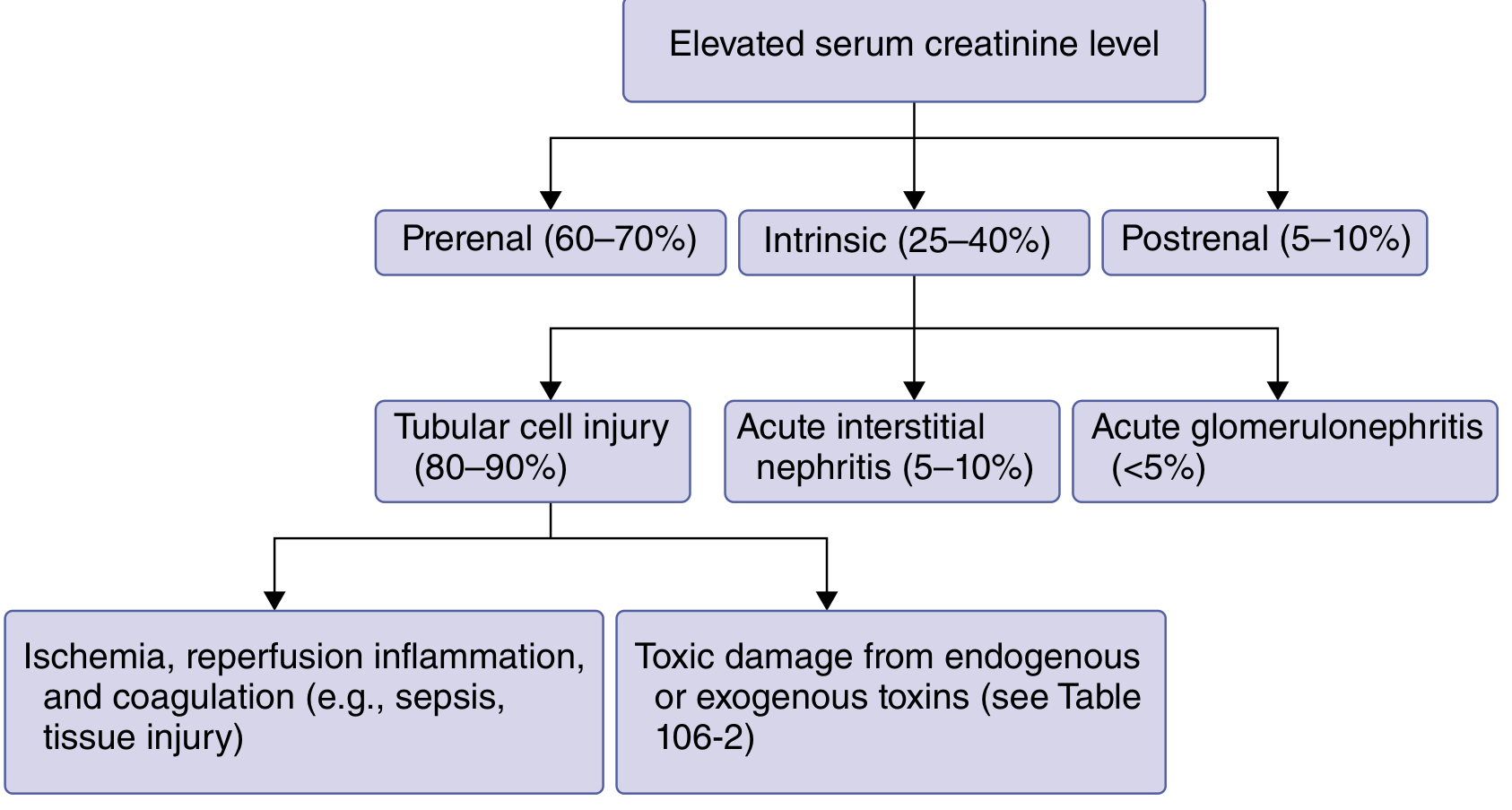
3. Classification: Prerenal / Intrinsic / Postrenal
A. Prerenal AKI (40-55% of cases; 60-70% community-acquired)
The most common cause. Kidney parenchyma is intact - the problem is hypoperfusion of structurally normal kidneys.
Pathophysiology:
- Reduced effective arterial blood volume (EABV) triggers baroreceptors
- Cascade: sympathetic activation → catecholamines → ADH release → RAAS activation
- Angiotensin II preferentially constricts the efferent arteriole to preserve GFR
- Severe/prolonged hypoperfusion → afferent constriction → GFR falls → ischemic ATN
Causes:
- True hypovolemia: hemorrhage, GI losses (vomiting, diarrhea), overdiuresis, third-spacing (pancreatitis), burns
- Decreased EABV without total body depletion: cardiogenic shock, septic shock, cirrhosis, hypoalbuminemia, anaphylaxis
- Volume-nonresponsive prerenal: CHF, liver failure, sepsis - IV fluids won't restore renal perfusion here
Diagnosis: Urinary biomarkers are NOT particularly elevated. Responds to volume/hemodynamic correction within hours.
Key labs:
- BUN:Cr ratio >20:1 (urea back-diffusion due to ADH)
- FENa <1% (avid sodium retention)
- Urine osmolality >500 mOsm/kg
- Urine sodium <20 mEq/L
- Specific gravity >1.020
(Brenner and Rector's The Kidney, p. 1197; Goldman-Cecil Medicine, p. 1243)
B. Intrinsic AKI (25-40% hospital; up to 60% in ICU)
Structural kidney damage causing an abrupt decline not restorable for days to weeks due to intensive vasoconstriction, tubular damage, cell death, and interstitial inflammation. Urinary biomarkers of tubular damage are markedly elevated.
Subtypes:
1. Acute Tubular Necrosis (ATN) - 80-90% of intrinsic AKI
- Ischemic ATN: Continuation of severe prerenal; ischemia + reperfusion injury → tubular cell death, cast formation, tubular obstruction, back-leak of filtrate
- Toxic ATN: Common nephrotoxins include:
- Antimicrobials: aminoglycosides, vancomycin, amphotericin B, acyclovir, tenofovir
- Contrast agents: radiocontrast nephropathy (risk x10 in CKD/volume-depleted patients)
- Endogenous toxins: myoglobin (rhabdomyolysis), hemoglobin (hemolysis), uric acid, calcium oxalate
- Drugs: cisplatin, cyclosporine, tacrolimus, methotrexate
- Septic AKI: inflammatory cytokines drive renal vasoconstriction + direct tubular injury
2. Acute Interstitial Nephritis (AIN) - ~15% of intrinsic AKI biopsies
- Drugs (most common): sulfonamides, penicillins, cephalosporins, NSAIDs, PPIs, checkpoint inhibitors (in ~5% of treated cancer patients)
- Infections: Legionella, leptospirosis, Yersinia, Streptococcus, TB, SARS-CoV-2, CMV, EBV
- Systemic disease: SLE, Sjögren syndrome, cryoglobulinemia
- Classic triad (fever + rash + eosinophilia) is present in <30% of cases
3. Acute Glomerulonephritis (<5%)
- Rapid-progressive GN (RPGN), vasculitis, lupus nephritis, anti-GBM disease
4. Vascular causes
- TTP/HUS, malignant hypertension, renal artery occlusion, cholesterol emboli
Diagnosis of intrinsic AKI: molecular analysis shows activation of inflammatory, ischemic, and coagulation pathways. FENa >2%, isosthenuria (urine osm ~300), granular ("muddy brown") casts in ATN, WBC casts in AIN.
(Goldman-Cecil Medicine, p. 1242-1244; Brenner and Rector's The Kidney, p. 1197+)
C. Postrenal AKI (5-10%)
Obstruction of urinary outflow. Requires bilateral obstruction (or obstruction of a solitary kidney) to raise sCr.
Sites and causes:
- Lower urinary tract (most common): BPH, prostate cancer, bladder cancer, cervical cancer, neurogenic bladder (diabetes, spinal cord disease)
- Ureteral (bilateral): retroperitoneal fibrosis, endometriosis, metastatic colon cancer, lymphoma
- Intraluminal: bilateral renal calculi, papillary necrosis, blood clots
Diagnosis: Renal ultrasound (hydronephrosis) is the first-line imaging. Prompt relief of obstruction reverses AKI.
(Goldman-Cecil Medicine, p. 1243-1244)
4. Pathophysiology of Ischemic ATN (Advanced)
The GFR loss in ATN is a summation of temporally activated systems:
- Microvascular compartment: Intense renal vasoconstriction - especially afferent arteriolar constriction reduces renal blood flow; endothelial activation promotes leukocyte adhesion
- Tubular injury:
- Proximal tubular cells lose polarity; Na-K-ATPase redistributes from basolateral to apical membrane
- Loss of brush border
- Sublethally injured cells shed apical membranes into the lumen → tubular casts → obstruction → back-pressure reduces GFR
- Sublethally injured cells detach and are shed in urine (viable + necrotic)
- Back-leak of filtrate: Damaged tubular epithelium loses integrity; glomerular filtrate leaks back across the tubular wall into the interstitium
- Innate immunity activation: Ischemia triggers NF-κB → pro-inflammatory cytokines (TNF-α, IL-6, IL-8, IL-18) → further vasoconstriction and tubular injury
- Reperfusion injury: Paradoxically, restoration of flow generates reactive oxygen species (ROS) and activates complement, worsening injury
(Brenner and Rector's The Kidney, p. 3434-3512)
5. Novel Biomarkers
Traditional markers (sCr, BUN) detect AKI only after significant GFR is lost. Novel biomarkers detect injury earlier:
| Biomarker | Source | Reflects | Notes |
|---|---|---|---|
| NGAL (neutrophil gelatinase-associated lipocalin) | Proximal tubule, neutrophils | Tubular stress/damage | Elevated in urine/plasma hours before sCr; NOT elevated in prerenal |
| KIM-1 (kidney injury molecule-1) | Proximal tubule glycoprotein (ectodomain shed) | Ischemic/toxic injury | mRNA rises more than any gene after injury; not elevated in healthy kidneys |
| IL-18 | Macrophages, proximal tubule | Ischemic injury | Urinary levels upregulated in multiple clinical settings |
| Cystatin C | All nucleated cells (filtered freely) | Earlier GFR changes | Urinary cystatin C predicts RRT need (AUC 0.86 in one cohort) |
| α1-Microglobulin | Proximal tubule dysfunction | Tubular damage | AUC 0.88 for AKI prediction at ER arrival |
| TIMP-2 × IGFBP7 | Cell cycle arrest markers | Imminent AKI risk | FDA-cleared NephroCheck test |
Key principle: Urinary NGAL and KIM-1 are elevated in intrinsic AKI, but NOT in prerenal disease - making them useful for differentiating these two categories.
(Comprehensive Clinical Nephrology, p. 984; Brenner and Rector's The Kidney, p. 651+)
6. Clinical Features
Symptoms:
- Often asymptomatic early (detected by labs)
- Oliguria (<400 mL/day) or anuria (<100 mL/day) - but AKI can be non-oliguric
- Nausea, vomiting, fatigue, confusion (uremia)
- Fluid overload: peripheral edema, pulmonary edema, hypertension
Uremia (advanced): Encephalopathy, asterixis, pericarditis, GI bleeding (platelet dysfunction), uremic frost (rare today)
Life-threatening complications:
- Hyperkalemia (most dangerous acutely - cardiac arrhythmias)
- Metabolic acidosis (non-anion gap initially, then elevated AG with uremia)
- Volume overload / pulmonary edema
- Hypo/hypernatremia
- Hypocalcemia + hyperphosphatemia
Important: Even 1 day of prerenal azotemia can produce hyponatremia, hyperkalemia, and acidosis with increased mortality. About 1/3 of hospitalized AKI cases resolve within 24 hours, ~60% by 48 hours, ~70% by 72 hours.
(Goldman-Cecil Medicine, p. 1243)
7. Diagnostic Approach
Step 1 - Confirm AKI: KDIGO criteria (above). Distinguish from CKD by prior baseline creatinine.
Step 2 - Identify category:
| Test | Prerenal | ATN | AIN | Postrenal |
|---|---|---|---|---|
| FENa | <1% | >2% | >2% | Variable |
| Urine osmolality | >500 | ~300 (isosthenuria) | Variable | Variable |
| Urine Na | <20 | >40 | >20 | Variable |
| Urine sediment | Bland / hyaline casts | Muddy brown / granular casts | WBC casts, eosinophils | Bland |
| Protein | Minimal | Tubular range | Variable | Variable |
| NGAL/KIM-1 | Normal | Elevated | Elevated | Normal |
Note: FENa can be <1% in early obstruction, contrast nephropathy, myoglobinuria, and AIN caused by NSAIDs - do not rely on it alone.
FEUrea (<35% suggests prerenal) is more reliable when the patient is on diuretics.
Step 3 - Renal ultrasound: Required in most cases to rule out obstruction, assess kidney size (CKD: small kidneys), and evaluate for hydronephrosis.
Step 4 - Consider kidney biopsy: When AIN, GN, or vasculitis is suspected and management will change.
8. Management
A. General Principles
- Remove the offending cause - stop nephrotoxins (NSAIDs, ACEi/ARBs, aminoglycosides, contrast), treat infection, relieve obstruction
- Volume status optimization - most patients need volume resuscitation, but avoid fluid overload (associated with worse outcomes). Balanced crystalloids (lactated Ringer's or PlasmaLyte) are preferred over normal saline (hyperchloremic metabolic acidosis risk)
- Hemodynamic support - MAP target ≥65 mmHg; vasopressors in septic AKI
- Electrolyte management - monitor K+, Na+, HCO3-, Phos, Ca2+ closely
- Nutritional support - high catabolic state; avoid protein restriction
- Drug dose adjustment - renally cleared drugs must be dose-adjusted
B. Specific Causes
- ATN: Supportive; no proven therapy reverses established ATN. Early removal of the insult is key
- Contrast nephropathy: Pre-hydration with IV isotonic saline; minimize contrast volume; use iso-osmolar contrast; N-acetylcysteine benefit uncertain
- AIN: Remove offending drug; corticosteroids (prednisolone 0.5-1 mg/kg/day) may accelerate recovery in drug-induced AIN if no improvement within 5-7 days
- Rhabdomyolysis: Aggressive IV fluid hydration (goal UO 200-300 mL/h); alkalinization of urine with sodium bicarbonate (controversial)
- Postrenal: Bladder catheterization or ureteral stenting; post-obstructive diuresis must be monitored
C. Avoiding Common Mistakes
- Do NOT give contrast without pre-hydration in at-risk patients
- Do NOT use nephrotoxic antibiotics when alternatives exist
- Do NOT withhold adequate volume resuscitation out of fear of fluid overload
- NSAIDs block prostaglandin-mediated afferent dilation - avoid in any patient at risk
9. Renal Replacement Therapy (RRT)
When to start (KDIGO indications - "AEIOU"):
- Acidosis - metabolic acidosis pH <7.1 refractory to medical management
- Electrolytes - refractory hyperkalemia (K+ >6.5 or with ECG changes)
- Intoxication - dialyzable toxins (methanol, ethylene glycol, lithium, aspirin)
- Overload (volume) - refractory pulmonary edema
- Uremia - uremic encephalopathy, pericarditis, bleeding
Early vs. Delayed RRT (Key Trials):
| Trial | Key Finding |
|---|---|
| AKIKI (620 pts, 31 centers) | Delayed RRT (wait for clinical indications) did NOT increase 60-day mortality vs. early RRT at KDIGO Stage 3; 49% of delayed group never needed RRT |
| ELAIN (231 pts, single center) | Early RRT (KDIGO Stage 2) reduced 90-day mortality vs. waiting for Stage 3 |
| IDEAL-ICU | No mortality benefit to early initiation in septic shock AKI |
Current consensus: Routine early RRT (based on staging alone) is NOT recommended. Patients whose dialysis is delayed tend to have earlier diuresis, fewer adverse events, and shorter RRT duration. Initiate RRT based on clinical indications (AEIOU).
RRT Modalities:
Intermittent Hemodialysis (IHD):
- Sessions 3-5 hours, blood flow 200-400 mL/min
- Good for stable patients; rapid solute clearance
- Risk: intradialytic hypotension (rapid fluid shifts); avoid in hemodynamically unstable patients
- Dialysis disequilibrium: use lower blood flows initially; hypertonic dialysate Na (145 mmol/L) for stability
- Avoid dialysate K+ <2 mmol/L (arrhythmia risk)
Continuous RRT (CRRT):
- Continuous venovenous hemofiltration (CVVH), hemodiafiltration (CVVHDF), or hemodialysis (CVVHD)
- Preferred for hemodynamically unstable patients
- Slow, continuous fluid/solute removal - better hemodynamic tolerability
- Requires continuous anticoagulation (regional citrate preferred; systemic heparin second choice)
- Dose: KDIGO recommends effluent volume of 20-25 mL/kg/h (actual delivered; order higher to account for downtime)
- Requires meticulous hourly fluid balance management
SLED (Sustained Low-Efficiency Dialysis):
- Hybrid modality: longer sessions (6-12 h) at lower flow rates
- Intermediate hemodynamic tolerability; can be done overnight
- Good option when CRRT infrastructure unavailable
No modality has shown superior survival; choice based on hemodynamic status, logistics, and expertise. KDIGO recommends CRRT and IHD in a complementary fashion.
(Brenner and Rector's The Kidney, p. 2816; Goldman-Cecil Medicine, p. 1245)
10. Special Situations (Advanced)
Hepatorenal Syndrome (HRS-AKI)
- AKI in cirrhosis with portal hypertension; functional renal failure due to severe splanchnic vasodilation
- ICA criteria: AKI (sCr rise ≥0.3 mg/dL or ≥50%) in cirrhosis, no response to 2 days of volume expansion + diuretic withdrawal
- HRS-1 (now HRS-AKI): rapidly progressive (formerly AKF); HRS-2: more gradual
- Treatment: vasoconstrictors (norepinephrine or terlipressin) + albumin infusion; liver transplant is definitive
Cardiorenal Syndrome (CRS)
- Type 1 CRS: acute heart failure → AKI (right-sided congestion raises renal venous pressure; left-sided failure reduces cardiac output)
- Both reduced output AND venous congestion contribute independently to AKI
- Management: careful decongestion while maintaining renal perfusion; avoid excessive diuresis
Contrast-Induced AKI (CI-AKI)
- sCr rise within 48-72 hours of contrast exposure
- Risk factors: pre-existing CKD (eGFR <45), diabetes, volume depletion, NSAID/ACEi use, high contrast volume
- Prevention: IV isotonic crystalloid (1-1.5 mL/kg/h for 3-12 h pre- and post-procedure); iso-osmolar contrast; minimize volume; hold nephrotoxins
AKI in Sepsis
- Most common cause of AKI in the ICU (~50% of ICU AKI)
- Mechanism: combined hemodynamic (vasodilation + microvascular dysfunction) + direct inflammatory/cytokine-mediated tubular injury
- Fluid resuscitation with balanced crystalloids; vasopressors for MAP ≥65 mmHg
- Early source control is the most important intervention
11. AKI-to-CKD Transition & Prognosis
- Mortality: Hospital mortality ~10-30%; ICU AKI mortality up to 50-60% depending on severity and comorbidities
- Recovery: ~70% of hospitalized AKI resolves within 72 hours; those requiring RRT have 30-60% in-hospital mortality
- AKI → CKD: AKI is a major risk factor for CKD development and progression - incomplete recovery leaves scar tissue (tubular atrophy + interstitial fibrosis)
- Risk of progression to CKD is proportional to AKI severity, number of AKI episodes, and degree of recovery
- AKI → cardiovascular events: AKI is independently associated with long-term cardiovascular morbidity (hypertension, heart failure)
- Post-discharge follow-up: all AKI patients should have kidney function checked at 3 months; those with AKD or incomplete recovery need nephrology referral
Prevention:
- Identify high-risk patients early (elderly, CKD, diabetes, CHF, hypovolemia)
- Avoid or minimize nephrotoxins
- Ensure adequate hydration before contrast/surgery
- Electronic AKI alert systems have been shown to improve detection and outcomes (Meta-Analysis, JAMA Network Open 2024, PMID: 39190304)
12. Quick Summary Table
| Feature | Prerenal | ATN | AIN | Postrenal |
|---|---|---|---|---|
| Frequency | 40-55% | 80-90% of intrinsic | 15% of intrinsic | 5-10% |
| Mechanism | Hypoperfusion | Ischemia/toxin | Drug/infection/immune | Obstruction |
| Urine sediment | Hyaline casts | Muddy brown casts | WBC + eosinophil casts | Bland |
| FENa | <1% | >2% | >2% | Variable |
| NGAL/KIM-1 | Normal | Elevated | Elevated | Normal |
| Reversibility | Rapid (hours) | Days-weeks | Weeks (if drug stopped) | Rapid after relief |
| Key treatment | Volume/hemodynamics | Remove insult + support | Stop drug ± steroids | Relieve obstruction |
Sources: Brenner and Rector's The Kidney (8e) - Chapters 28/65; Goldman-Cecil Medicine - Chapter 106; Comprehensive Clinical Nephrology (7e) - Chapter 72; Sabiston Textbook of Surgery - Chapter 26; Current Surgical Therapy (14e)
Recent evidence update (2024-2026): Electronic AKI alert systems improve recognition and may improve outcomes (systematic review, PMID 39190304). Balanced crystalloids (vs. normal saline) continue to be supported in septic resuscitation with AKI (systematic review, PMID 39891147).
This is a shared conversation. Sign in to Orris to start your own chat.